
Abstract
Background:
The orientation of the acetabulum has a fundamental role in impingement and instability of the hip, and the spinopelvic parameters are thought to predict the sagittal orientation of the acetabulum (SOA). However, similar to the acetabular version (axial orientation) and inclination (coronal orientation), the cephalic or caudal orientation of the acetabulum in the sagittal plane, or SOA, may primarily be an intrinsic feature of the acetabulum itself.
Purpose:
To determine whether the spinopelvic parameters predict the sagittal orientation of the acetabulum in individuals without lumbar deformity.
Study Design:
Cross-sectional study; Level of evidence, 4.
Methods:
A retrospective analysis was performed in 89 patients (94 hips; 62 female, 27 male; mean ± SD age, 45.9 ± 15.4 years) without lumbosacral deformity who underwent magnetic resonance arthrogram (MRA) for assessment of hip pain. The SOA was determined in the sagittal cut MRA. A line was drawn at the distal limit of the anterior and posterior acetabular horns longitudinally to the transverse ligament, and the angle between this line and the axial plane represented the SOA. The sacral slope, pelvic incidence, and spinopelvic tilt were determined using a 3-dimensional cursor and the axial, sagittal, and coronal cuts. All MRA studies were performed with the patient in the supine position.
Results:
The SOA had a mean ± SD cephalic orientation of 18° ± 6.6°. No significant correlation was observed between the SOA and the sacral slope (r = –0.03; P = .77). A weak correlation was observed between the SOA and the pelvic incidence (r = 0.22; P = .03) and between the SOA and the spinopelvic tilt (r = 0.41; P < .01).
Conclusion:
The SOA cannot be presumed based on the spinopelvic parameter. Similar to the well-known parameters to assess the axial and coronal orientation of the acetabulum, the assessment of the SOA demands acetabular-specific parameters. Additional studies are necessary to assess the SOA in asymptomatic hips, including disparities between genders. Clinically significant values for abnormal SOA of the acetabulum remain to be defined.
Keywords
The orientation of the acetabulum has a fundamental role in impingement and instability of the hip. 13,20 Multiple studies have assessed the axial and coronal orientation of the acetabulum with regard to hip impingement and instability. 1,4,18,24,27,28,30 The acetabular version (axial orientation) or inclination (coronal orientation) is considered an intrinsic feature of each acetabulum, whereas the sagittal orientation of the acetabulum (SOA) is thought to be determined by the spinopelvic orientation in the sagittal plane. 5,14,17 Similar to the axial and coronal orientation of the acetabulum, the SOA influences the occurrence of impingement and instability at the hip and may affect the surgical techniques applied to the hip. 17 However, the SOA is a sporadic subject of research, and even reports on redirectional acetabular osteotomies usually ignore their effects on the SOA. 6,9,21,26 Three cadaveric studies have investigated the SOA using the acetabular notch 12,22 or the distal ends of the anterior and posterior acetabular horns as reference for its measurement 10 (Figure 1).

Lateral view of the left hip. (A) The sagittal orientation of the acetabulum is assessed by the angle between the axial plane (blue line) and the distal limit of the anterior and posterior acetabular horns (arrows, red line). (B) Cadaveric specimen demonstrating the semilunar surface of the acetabulum, represented by the acetabular roof, anterior horn, and posterior horn.
The association of hip and spine symptoms is frequent in orthopaedic practice and is referred as hip-spine syndrome. 23 Three parameters have been used when assessing the relationship between the hip, pelvis, and lumbar spine in the sagittal plane: pelvic incidence, sacral slope, and spinopelvic tilt. 2,11,15,29 The pelvic incidence is the sum of 2 complementary angles: pelvic tilt and sacral slope. 15 Because the pelvic incidence is fixed for any given patient, the sum of pelvic tilt and sacral slope is a constant value: When one increases, the other necessarily decreases. 11
Deformities at the lumbar spine may change the sagittal orientation of the hip and pelvis. 3 However, to our knowledge, the relationship between the SOA and the spinopelvic parameters has not been evaluated in individuals with hip pain and without deformity at the lumbar spine. The purpose of this study was to determine whether the spinopelvic parameters predict the sagittal orientation of the acetabulum in individuals without lumbar deformity. The hypothesis was that the spinopelvic parameters would present a strong correlation with the SOA.
Methods
This study was carried out in an urban academic tertiary-care orthopaedic facility and was approved by the hospital’s institutional review board. A retrospective review was performed in 341 patients who had a first office visit between October 2018 and September 2019. The patients were screened for the following inclusion criteria: availability of magnetic resonance arthrogram (MRA) of the hip, absence of Tönnis osteoarthritis grade 2 or 3, absence of ipsilateral hip surgery, and absence of contralateral hip arthroplasty. Exclusion criteria were acetabular dysplasia (lateral center-edge angle <25° on anteroposterior pelvic radiograph 30 ), history of lumbar fusion, spondylolisthesis, L5/S1 transitional vertebral morphology, and incomplete MRA. Complete MRA studies included 3-mm cuts of the hip in the sagittal, axial, and coronal planes; a sagittal cut of the pelvis at midline; and axial and coronal plane images of the pelvis. All MRA studies were performed with the patient in a supine position. In total, 94 hips in 89 patients (62 women and 27 men) with a mean ± SD age of 45.9 ± 15.4 years were studied (Figure 2). A fellowship-trained board-certified hip surgeon screened the images and performed the measurements.
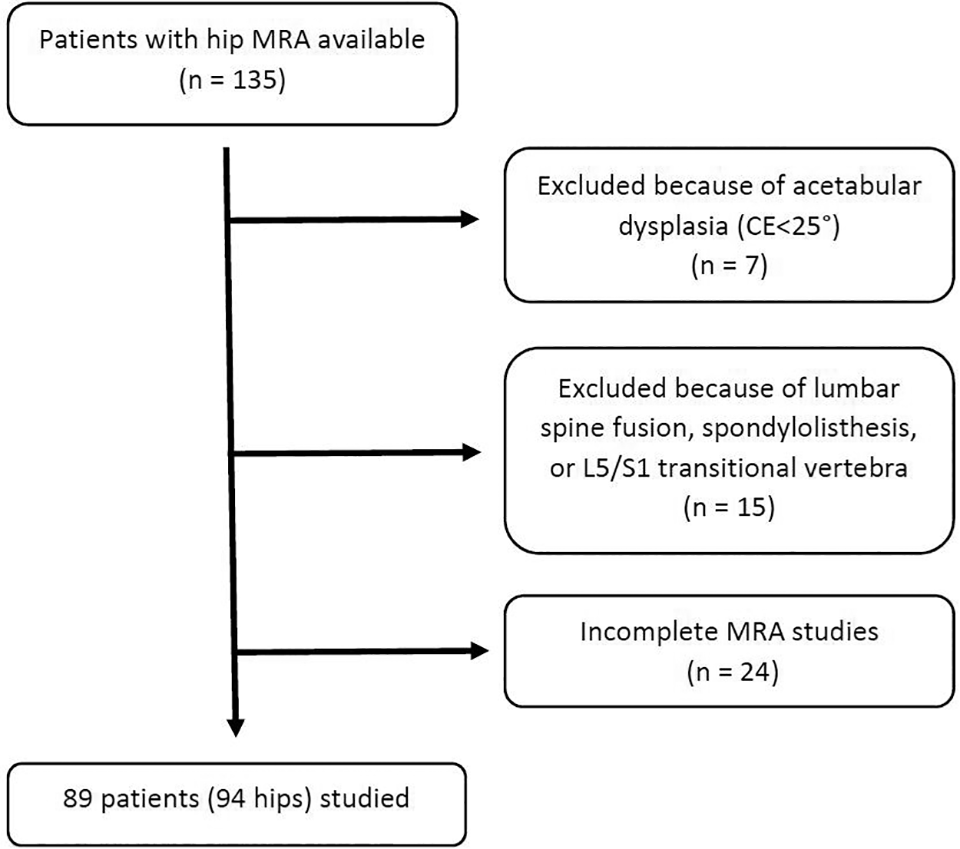
Diagram of patient selection. CE, center-edge angle; MRA, magnetic resonance arthrogram.
Magnetic Resonance Assessments
Sagittal MRA cuts were used to assess the SOA. The acetabular fossa was localized, and the image chosen for the assessment demonstrated the transverse ligament of the acetabulum running between the distal ends of the anterior and posterior acetabular horns (Figure 3A). A first line was drawn tangent to the distal limit of the anterior and posterior acetabular horns along the transverse ligament, and the angle between this line and the axial plane represented the SOA (Figure 3B). The axial plane was used as reference for the SOA, as this plane was also the reference to determine the sacral slope.
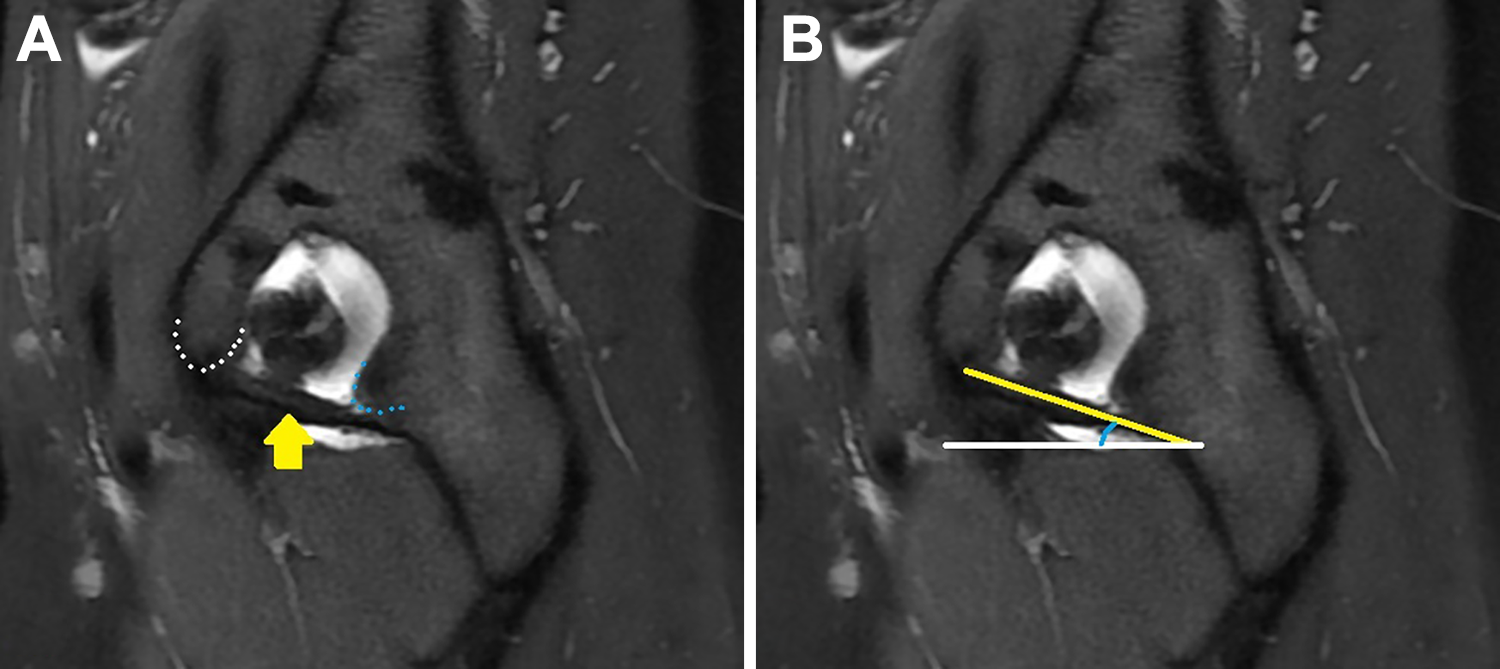
Sagittal cut of a hip magnetic resonance arthrogram. (A) Transverse ligament (yellow arrow) running between the distal limits of the anterior (white dotted line) and posterior (blue dotted line) acetabular horns. (B) The angle between the yellow and white lines represents the sagittal orientation of the acetabulum.
A midline magnetic resonance imaging sagittal scan of the pelvis was used to measure the sacral slope, pelvic incidence, and spinopelvic tilt (DICOM viewer; Inteleviewer, Intelerad). 17 The sacral slope was represented by the angle between the axial plane and a line tangent to the superior end-plate of S1 (Figure 4A). 29 Axial and coronal images of the pelvis were used to define the bicoxofemoral axis (the line between the geometric center of both femoral heads) 15 (Figure 4B), and a 3-dimensional cursor was used to project this axis into the midline sagittal cut. 17 The pelvic incidence was the angle between the perpendicular to the sacral plate at its midpoint and the line connecting this point to the bicoxofemoral axis (Figure 4C). The spinopelvic tilt was the angle between the vertical line and the line joining the middle of the sacral plate and the bicoxofemoral axis (Figure 4D). 2 The spinopelvic tilt was calculated by subtracting the sacral slope from the pelvic incidence. 15
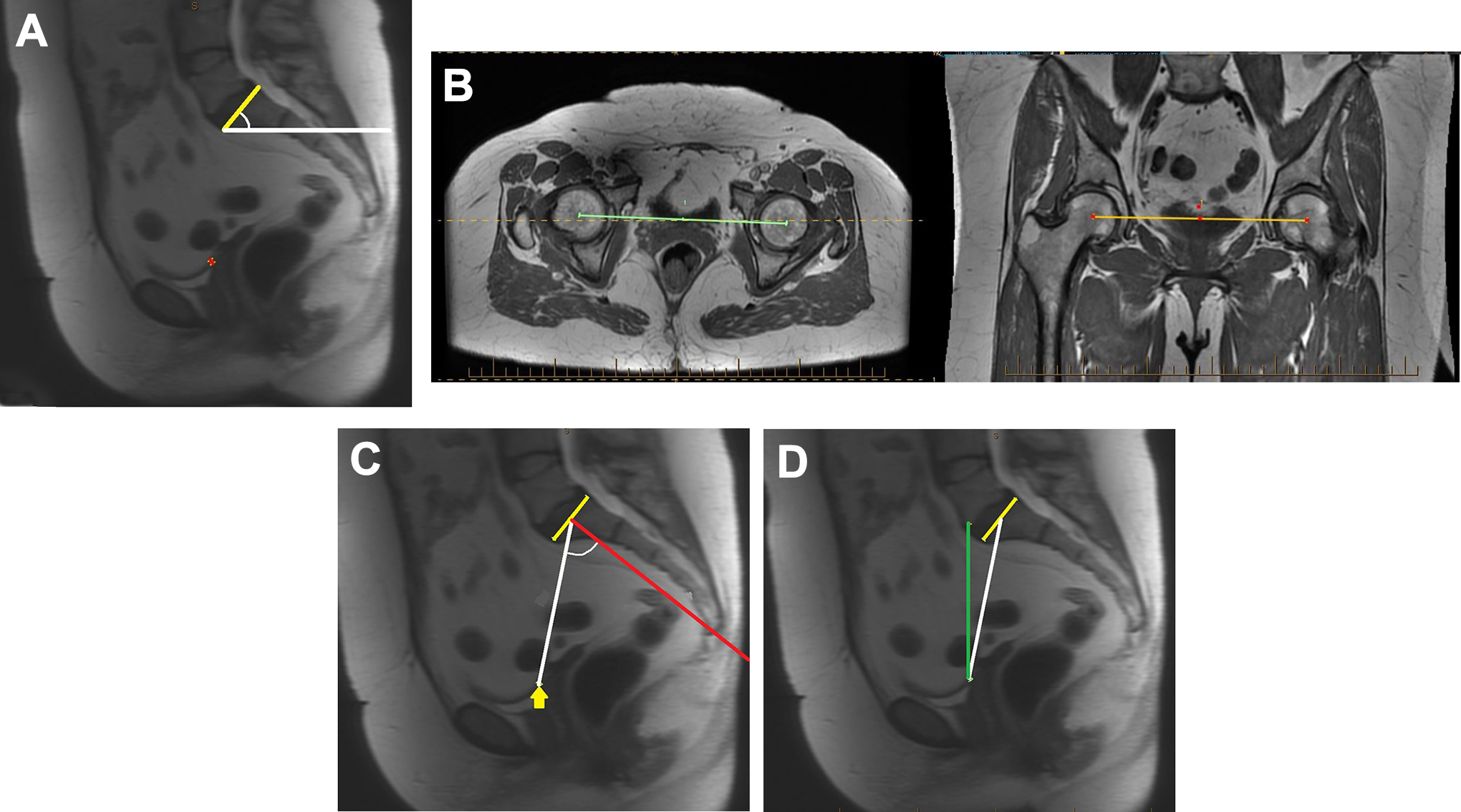
Assessment of the spinopelvic parameters in a midline sagittal cut of a pelvic magnetic resonance imaging scan. (A) Sacral slope, represented by the angle between a horizontal line (white line) and a line tangent to the superior end-plate of S1 (yellow line). (B) Bicoxofemoral axis defined in the axial and coronal planes. (C) Pelvic incidence, represented by the angle between the perpendicular line (red line) to the sacral plate at its midpoint and the line (white line) connecting this point to the bicoxofemoral axis (yellow arrow). (D) Spinopelvic tilt, represented by the angle between the vertical line (green line) and the line joining the middle of the sacral plate and the center of the bicoxofemoral axis (white line).
Statistical and Reliability Analysis
The normality of data distribution was determined using the Kolmogorov-Smirnov (K-S) test. A normal distribution was observed for the SOA (K-S test, 0.06; P = .86), the sacral slope (K-S test, 0.09; P = .4), the pelvic incidence (K-S test, 0.06; P = .83), and the spinopelvic tilt (K-S test, 0.08; P = .48). Student t tests for independent samples were used to assess sex-related differences, and P values of <.05 were considered significant. In the 5 patients with both hips included, the mean of the measurements performed in the right and left acetabula was considered in order to assess sex-related differences. Pearson coefficients were calculated to examine correlations between variables, and P values of <.05 were considered significant.
The imaging measurements were tested for intra- and interrater reliability in 20 hips randomly chosen from the 94 included hips. The intrarater reliability was determined based on a second measurement performed by the main investigator at least 10 days after the original measurement. The measurements performed by a senior orthopaedic surgery resident (S.J.N.) were compared with those of the main investigator (M.H.) to determine the interrater reliability. Precision of measurement by a single observer (intrarater reliability) and between observers (interrater reliability) was determined by calculating the 95% CI between the repeated measurements and their average. The intraclass correlation coefficients for the radiographic and MRA measurements are presented in Table 1. The statistical analysis was performed using MedCalc Version 19.2.1 software.
Intra- and Interrater Reliability of the Imaging Parameters a

a ICC, intraclass correlation coefficient.
Results
The acetabula had a mean ± SD cephalic orientation of 18° ± 6.6°. The acetabula were less cephalically oriented (P < .01) in female hips (16° ± 6.2°) than in male hips (22° ± 5.7°). Table 2 summarizes the imaging measurements for the 94 hips (89 patients) included in this study.
No significant correlation was observed between the SOA and the sacral slope (r = –0.03; P = .77) (Figure 5A). A weak correlation was observed between the SOA and the pelvic incidence (r = 0.22; P = .03) (Figure 5B) and between the SOA and the spinopelvic tilt (r = 0.41; P < .001) (Figure 5C).
Magnetic Resonance Parameters of the 94 Hips (89 Patients) Studied a

a Values are expressed in degrees as mean ± SD (range).

Scatter diagram and regression line according to the sagittal orientation of the acetabulum (SOA) and (A) the sacral slope, (B) pelvic incidence, and (C) spinopelvic tilt.
Discussion
The study results indicated that the SOA is essentially an intrinsic feature of the native acetabulum itself; that is, in individuals without lumbar spine fusion or spondylolisthesis, the cephalic or caudal orientation of the acetabulum in the sagittal plane is not primarily defined by the lumbopelvic orientation (Figure 6). Considering that the value of pelvic incidence is fixed for any given patient, the relationship between the SOA and pelvic incidence would be the same, independent of the body posture. 11 The position in which patients undergo their MRA studies should be considered when interpreting the correlation between the SOA and sacral slope or spinopelvic tilt.
Changing from a supine or standing position to a sitting position decreases the sacral slope on average 50% and increases the spinopelvic tilt on average 200%. 7,16 As consequence, the correlation between the SOA and the sacral slope or spinopelvic tilt will change from a supine to a sitting position. The assessments of the present study were performed in images obtained with the patient in a supine position. The translation of the present study findings to the standing position is supported by the fact that the mean sacral slope (39°) and spinopelvic tilt (8°) differed <5° from those described in studies in which the spinopelvic parameters were assessed on standing radiographs (Table 3).

Images for 2 patients with similar spinopelvic parameters and very different sagittal orientation of the acetabulum (SOA). (A, B) Patient (left hip) with 8° of transverse ligament slope, 34° of sacral slope, and –2° of spinopelvic tilt. (C, D) Patient (right hip) with 33° of SOA, 33° of sacral slope, and 2° of spinopelvic tilt.
Values for Sacral Slope, Pelvic Incidence, and Spinopelvic Tilt Reported in the Literature a

a Values are expressed in degrees as mean ± SD.
In patients with high-grade spondylolisthesis or lumbar fusion, 19 the influence of the spinopelvic parameters on the SOA may be more significant than that observed in patients included in the present study. Patients with spondylolisthesis typically present a significantly decreased sacral slope with secondary change in the sagittal orientation of the acetabulum (Figure 7). 3 Patients with hip dysplasia were not included in the present study, considering the possibility of abnormal morphology of the anterior and posterior acetabular horns and consequent loss of accuracy to assess the SOA. Increased sacral slope has been reported in patients with hip osteoarthritis secondary to acetabular dysplasia. 3

Increased cephalic orientation of the acetabulum due to lumbosacral spine deformity and arthrodesis. (A) Sagittal magnetic resonance arthrogram demonstrating an acetabular cephalic orientation of 35°. (B) Sagittal computed tomography of the same patient. Note the decreased sacral slope due to spondylolisthesis and subsequent arthrodesis.
The SOA can have clinical and surgical repercussions in patients with hip pain. Patients with increased (more cephalic) SOA have decreased femoral head coverage anteroinferiorly and increased coverage posteroinferiorly. A more cephalic SOA, associated with a steep anterior acetabular horn, predisposes to anteroinferior hip instability. 10 Meanwhile, a less cephalic SOA, associated with a steeper posterior horn and decreased femoral torsion, predisposes to posteroinferior instability (Figure 8). 3 A decreased SOA predisposes to anterosuperior femoroacetabular impingement (Figure 9). Acetabula with less cephalic orientation could explain the presence of the high-cross sign in patients with pincer-type femoroacetabular impingement, and this is a potential subject of research. The relationship between the SOA and the ligamentous structures on hip impingement or instability is another subject to be studied. Acetabular redirectional osteotomies may change the acetabular orientation on the coronal and axial planes and provoke femoroacetabular impingement. 6,9,21,26 The rotation of the acetabular fragment in the sagittal plane also has the potential to provoke anterosuperior impingement, and the assessment of SOA on computed tomography or magnetic resonance scans could contribute to a more precise surgery. The determination of the SOA may be beneficial before lumbar spine surgeries involving fusion and/or correction of deformities. We have observed a number of patients with acetabula cephalically oriented >30° assuming a posture of trunk flexion to increase the anterior coverage of the femoral head, particularly when increased femoral torsion is associated. For instance, the patient presented in Figure 7, who was excluded from the current study because of the presence of spondylolisthesis, had a cephalic orientation of 35° and increased femoral torsion bilaterally. This patient could walk with less discomfort by bending her trunk forward and internally rotating her hip, and this posture could balance the pelvic and femoral malalignment by increasing the anterior coverage of the femoral head.

Magnetic resonance images of a patient with recent history of posterior right hip dislocation while skiing. The sagittal cut (left) demonstrates decreased cephalic orientation (8°) of the acetabulum associated with decreased femoral torsion (1°).

(A) Magnetic resonance arthrogram demonstrating decreased (3°) cephalic orientation of the acetabulum in the sagittal plane in a patient with anterosuperior impingement and (B) associated labral tear (yellow arrow).
Limitations to this study should be noted. First, the patients included had hip pain and nonarthritic hips, and the measured SOA may not reflect the values observed in nonsymptomatic individuals or in those with hip osteoarthritis. Second, the spinopelvic parameters were assessed on MRAs performed with the patient supine; spinopelvic parameters traditionally have been evaluated on standing radiographs, and modification in the orientation of the pelvis is a possibility from supine to standing. However, the average values of the spinopelvic parameters observed in our sample were comparable with those presented in studies with standing radiographs, and the pelvic incidence is independent from the patient positioning.
Conclusion
The SOA cannot be presumed based on the spinopelvic parameters. Similar to the well-known parameters to assess the axial and coronal orientation of the acetabulum, the assessment of the SOA demands acetabular-specific parameters. Additional studies are necessary to assess the SOA in asymptomatic hips, including disparities between sexes. Clinically significant values for abnormal SOA of the acetabulum remain to be defined.
Footnotes
Final revision submitted June 5, 2020; accepted June 23, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: H.D.M. has received research support and faculty/speaking fees from Smith & Nephew, educational support from Pylant Medical, and nonconsulting fees from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Baylor Scott and White Institutional Review Board.