
Abstract
Background:
Large (4.5 mm) and/or transpatellar bone tunnels have been associated with patellar fracture after medial patellofemoral ligament (MPFL) reconstruction. To avoid this outcome, many surgeons now employ suture anchors to affix the MPFL graft to the patella.
Purpose:
To evaluate the risk of patellar fracture and other outcomes associated with smaller (3.2-mm), short, oblique patellar tunnels as compared with suture anchor fixation in MPFL reconstruction.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A single institution’s electronic medical record was queried for all patients undergoing MPFL reconstruction between March 2010 and December 2018. A chart review of operative reports was utilized to identify those who had undergone MPFL reconstruction. Patients undergoing revision MPFL reconstruction or reconstruction with fully transpatellar bone tunnels were excluded. The incidence of patellar fracture and outcomes were evaluated from chart review. The mean duration of follow-up was >2 years.
Results:
A total of 384 knees in 352 patients undergoing primary MPFL reconstruction were identified. Small (3.2-mm), short, oblique tunnels were used for patellar fixation in 215 cases, and suture anchors were utilized in 169 cases. The small, oblique tunnels and suture anchor techniques both resulted in a low incidence of patellar fracture, with rates of 0.47% and 0%, respectively. The use of suture anchors was associated with an increased risk of subluxation or dislocation compared with small, oblique tunnels (odds ratio, 3.98; P = .028). No significant difference was found in the need for revision MPFL reconstruction surgery with suture anchors (odds ratio, 1.925; P = .66).
Conclusion:
The use of small, oblique tunnels with hamstring autograft is a safe means of patellar fixation in MPFL reconstruction. The use of small, oblique tunnels for patellar fixation versus 2 suture anchors can result in material cost savings with no significantly increased risk for fracture as well as an overall reduction in complication rates.
Recurrent patellar instability is a relatively common condition that results in lateral subluxation or dislocation of the patella from the trochlear groove. 4 Patellar dislocations occur with an incidence of 5.8 per 100,000 people and at an increased frequency in younger age groups (10-20 years old), women, athletes, and those with chronic conditions that result in ligamentous laxity. 6 Various anatomic factors may predispose an individual to being at greater risk of sustaining a dislocation event, and those who sustain a prior patellar dislocation are at increased risk of a subsequent event, with recurrence rates nearing 40%. 14 Physical therapy with an emphasis on proprioception exercises as well as strengthening of the vastus medialis obliquus (VMO) and hip abductors is the mainstay of treatment for an initial patellar dislocation. In instances of recurrent dislocation, operative intervention may be indicated. 14 Operative intervention in the case of deficient medial soft tissue restraints involves a functional anatomic reconstruction of the medial patellofemoral ligament (MPFL), the primary medial static stabilizer of the patella. The MPFL provides passive stability to the patella during early flexion before the patella engages with the trochlea. 3, 22 At the time of MPFL reconstruction, consideration is also placed on the performance of adjunctive procedures if evaluation reveals additional abnormal anatomy contributing to the patient’s recurrent instability. 1,10,20
Numerous graft sources, techniques, and fixation methods have been described with favorable outcomes during reconstruction of the MPFL. 9 Several techniques exist for fixation of the graft to the patella, including the use of suture anchors, interference screws, and bone tunnels. To date, no particular method has emerged as superior with regard to clinical outcome. 6,17,19,28 Specifically, the use of transpatellar bone tunnels and suture anchors for patellar fixation has been shown to demonstrate good or excellent functional outcome. 11,12,15,25 These techniques do, however, offer their respective advantages and disadvantages. Russ et al 21 showed that the use of bone tunnels with interference screw fixation offers a biomechanically stronger fixation than the use of suture anchors. Despite being biomechanically weaker, the authors did find that suture anchor fixation nevertheless allows for a reconstruction that withstands greater loads before failure than the native MPFL. 21 The use of suture anchors also minimizes the risk of violating the articular surface when reaming tunnels and decreases the risk of patellar fracture, which can necessitate further surgery. 14 While the use of 4.5-mm, transverse patellar tunnels with looped graft for patellar fixation has been associated with an increased risk for patellar fracture, outcomes from using 2 smaller (3.2-mm), short, oblique patellar tunnels have not been studied in case series or in comparison with other existing methods. 23 As no technique has emerged as the standard of care, and with there being a lack of studies directly comparing clinical outcomes between the use of dual patellar suture anchors and dual, small, oblique bone tunnels for patellar fixation, this retrospective study aims to compare clinical outcomes and complications between these 2 techniques in patients who underwent MPFL reconstruction at our institution. We hypothesized that the use of small (3.2-mm), oblique patellar tunnels for patellar fixation during MPFL reconstruction would not be associated with an increased risk of patellar fracture in comparison with the use of suture anchors.
Methods
Data Collection
This study was granted exempt status, and under federal regulations, full institutional review board approval was not required. Retrospective chart review was performed by authors M.J.D., T.E.M., M.L., and Z.R.B. to identify patients from March 2010 to December 2018 that underwent MPFL reconstruction. Each identified patient’s chart was evaluated for data collection.
All procedures were performed by 1 of 6 fellowship-trained orthopaedic surgeons (including D.R.D.) at a single academic institution. If indicated by the attending surgeon, MPFL reconstruction was combined with a tibial tubercle osteotomy, with or without distalization for patella alta. An ipsilateral gracilis or semitendinosus autograft or allograft was used for each patient based on surgeon preference. A gracilis graft was preferable to a semitendinosus graft because of the 3.2-mm size of the oblique tunnel technique used in this study. The larger size of the semitendinosus graft typically requires larger bone tunnels in the patella, potentially increasing the risk of patellar fracture. The inclusion criterion for the study was limited to primary MPFL reconstruction. Patients who had undergone prior MPFL reconstruction with a graft were excluded. Patients who underwent concomitant femoral osteotomies or trochleoplasty procedures were also excluded. Patient characteristics, including age and sex, were recorded. Laterality, graft type, and concomitant procedures were also recorded. The primary outcome of interest was the incidence of particular complications, specifically subsequent patellar fracture, recurrent subluxation or dislocation, and the need for revision MPFL reconstruction. Written operative reports, intra- and postoperative imaging, and postoperative clinic notes were used to identify the outcomes of interest. Patellar instability or dislocation was determined by subjective patient reporting and documentation of instability events that were validated by a physical examination or further surgical interventions. Patients were managed intra- and postoperatively depending on the attending surgeon’s own clinical judgment. Standard indications were used to determine the need for concomitant procedures. 6 An anteromedializing tibial tubercle osteotomy was performed in addition to MPFL reconstruction when the tibial tubercle–trochlear groove distance was found to be greater than 20 mm as determined on a computed tomography scan. A concomitant distalization of the tibial tubercle was included if patella alta was found to be present, as determined by a Caton-Deschamps index measurement greater than 1.2 on a lateral radiograph of the knee in 30° of flexion. 6
Surgical Technique
Small (3.2-mm), Short, Oblique Patellar Tunnels for Patellar Fixation
The MPFL reconstruction was undertaken in the manner previously described by Smith et al 24 to re-create the sail shape of the native MPFL, with its attachment on the proximal half of the patella. After the medial aspect of the patella was prepared, 2 short tunnels were drilled obliquely through the patella using a 3.2-mm drill bit. The first of these was drilled in the upper third of the medial border of the patella just anterior to the articular surface. The surgeon’s hand was dropped as the drill was advanced to obtain as steep an angle as possible while maintaining a bony bridge. The drill bit naturally and partially encroached upon the articular cartilage, but this is outside any major weightbearing zone. The Beath pin used to shuttle the graft through the patella was placed in the first tunnel and used as a guide to ensure that the proximal and distal tunnels were parallel to one another with their anterior exit occurring approximately one-third of the diameter across the patella. The second tunnel was then drilled 1 cm distal to the first (Figure 1). Next, the previously harvested hamstring tendon graft was looped through the holes from medial to lateral proximally and lateral to medial distally (Figure 2).
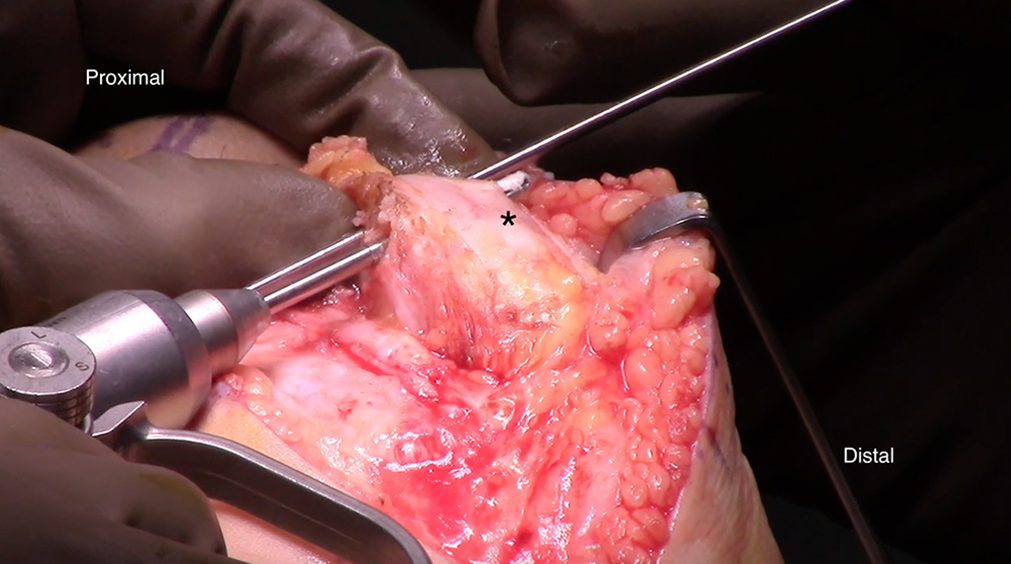
Left knee image. The surgeon uses a 3.2-mm drill bit to create 2 short, oblique patellar tunnels. The drill is started just anterior to the articular cartilage of the medial patellar facet and is oriented so that the tunnels exit the anterior patella (*) in its proximal half.

Left knee image. The graft used for medial patellofemoral ligament reconstruction is passed through the short, oblique patellar tunnels and is extended medially.
The graft was then passed between layers 2 and 3 of the medial knee to the Schöttle point as confirmed with fluoroscopy (Figures 3 and 4). Once isometry was established and maintained throughout full range of motion, the 2 free ends of the graft were pulled into a bone tunnel and secured to its femoral attachment with an absorbable interference screw.
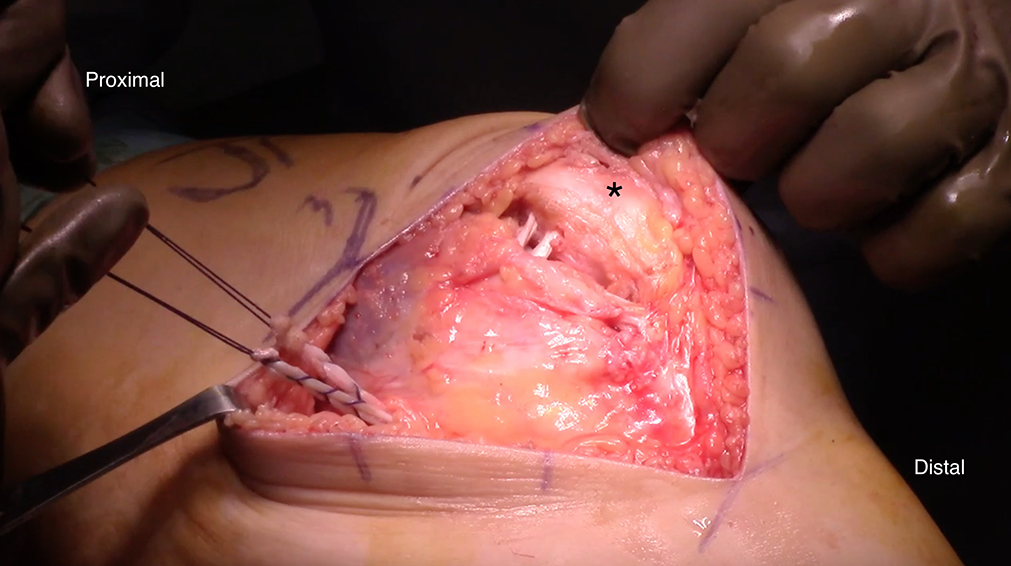
Left knee image. The graft is passed between layers 2 and 3 of the medial knee in anticipation of subsequent fixation to the femur at the Schöttle point. The asterisk indicates the patella.

Standard (A) tangential or Merchant view and (B) lateral view radiographs of a right knee depicting the radiographic landmarks for graft fixation. Red arrow identifies Schöttle point; blue arrows note the position of bone tunnels.
Dual Suture Anchor Patellar Fixation
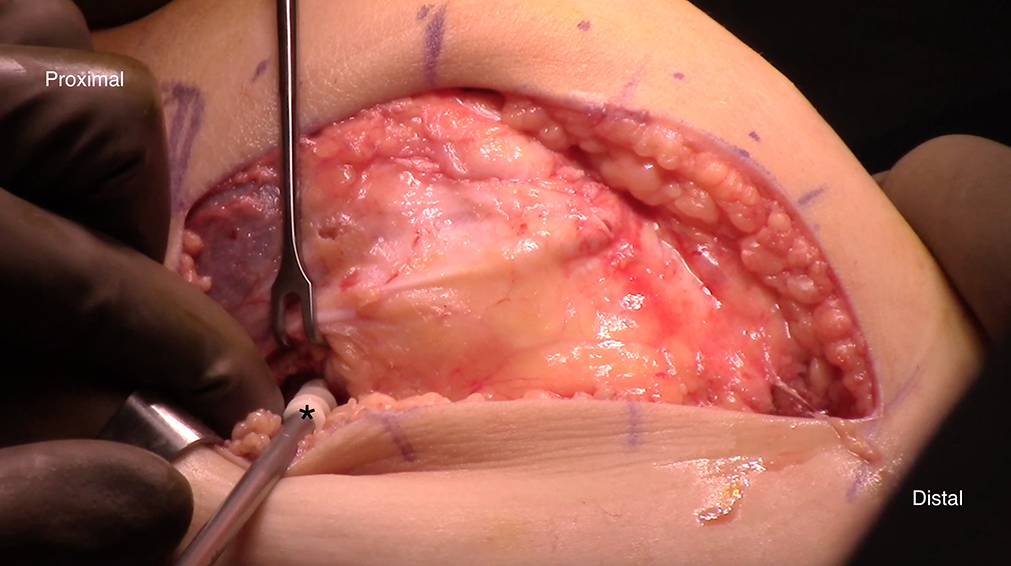
Rather than drilling 2 small (3.2-mm), short oblique tunnels, 2 suture anchors (Gryphon Suture Anchor; Johnson & Johnson) were secured to the medial patellar border. The first suture anchor was placed just distal to the VMO attachment, and the second suture anchor was placed 1 cm distal to the first (Figure 5). The graft was then secured to the suture anchors. Establishment of isometry and use of a femoral interference screw occurred as described above (Figure 6).

Right knee image. (A) A second suture anchor is placed in the medial patellar (*) border 1 cm distal to a previously placed suture anchor. (B) The graft is subsequently secured to the suture anchors.
Left knee image. After confirming isometry of the graft throughout full range of motion, the 2 ends of the graft are secured to the femoral attachment at the Schöttle point using an absorbable interference screw (*).
Statistical Analysis
Statistical analysis was performed with IBM SPSS Statistics Version 24 (IBM Corporation) and R Version 3.6.0 (R Studio). Since all variables were categorical, chi-square or Fisher exact tests were used to evaluate associations between variables. Given the sample size and the rarity of evaluated outcomes, a Firth logistic regression was also performed for further data validation. Patients with hybrid gracilis/semitendinosus grafts (n = 3), hybrid auto-/allografts (n = 1), and unknown hamstring graft type (n = 1) were excluded from analysis. A P value less than .05 was necessary to reject the null hypothesis and be considered statistically significant.
Results
The current study included 384 knees in 352 patients. A total of 215 (56.0%) knees underwent patellar fixation with small, oblique bone tunnels (61.4% women; mean age, 23.16 ± 9.99 years), and 169 (44.0%) knees received suture anchors for fixation (64.5% women; mean age, 24.28 ± 9.38 years). The mean duration of follow-up was >2 years. A total of 196 (51.0%) knees underwent isolated MPFL reconstruction, and 188 (49.0%) were combined with other concomitant procedures (Table 1). The majority of grafts were gracilis tendons (69.8%) and autograft (82.8%). A further breakdown of graft type by method of patellar fixation is provided in Table 2.
Patient Characteristics for Those Who Underwent Primary MPFL Reconstruction a
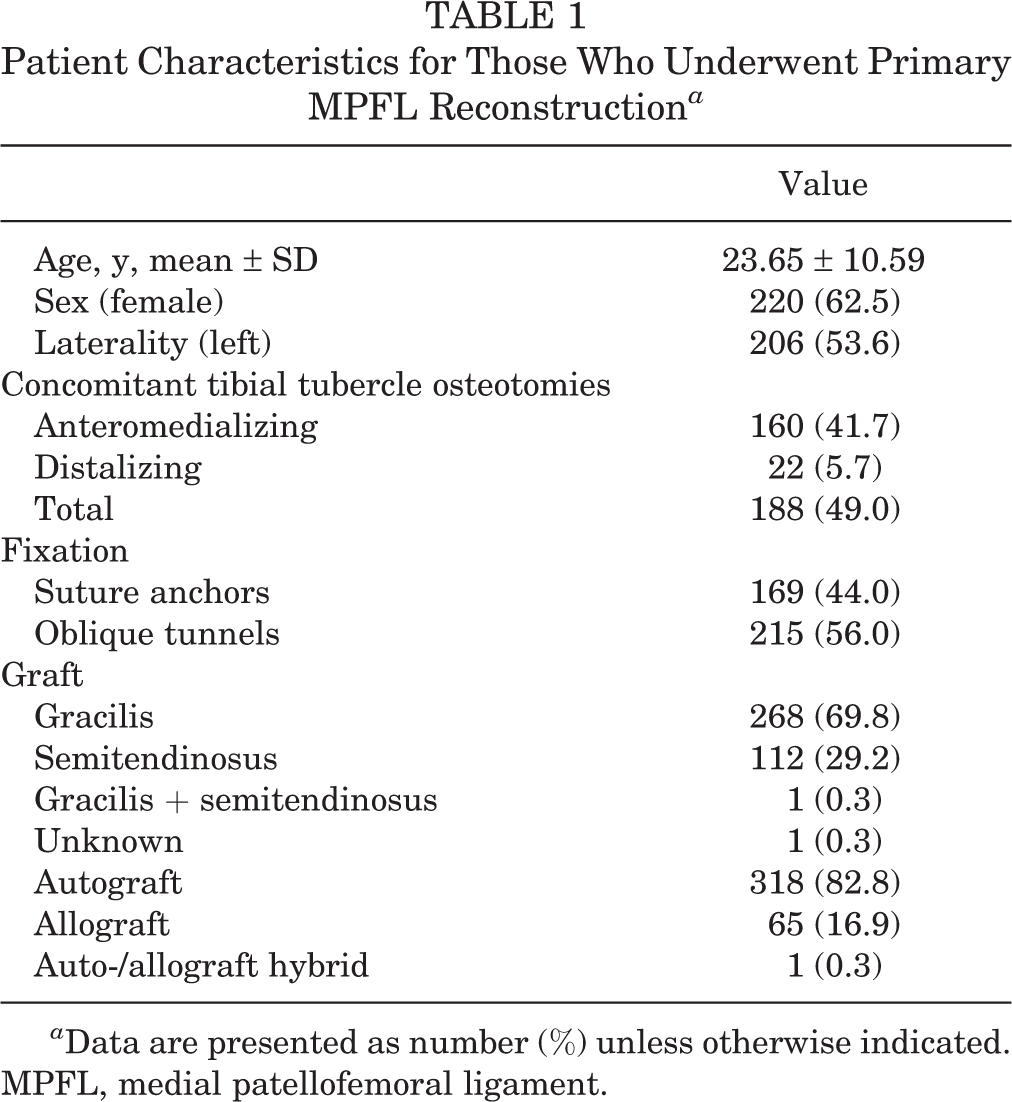
a Data are presented as number (%) unless otherwise indicated. MPFL, medial patellofemoral ligament.
Outline Regarding the Graft Type Used in Relation to the Method of Patellar Fixation

There was 1 reported patellar fracture, which occurred approximately 16 weeks postoperatively in a patient who received a looped semitendinosus autograft for primary MPFL reconstruction in conjunction with a tibial tubercle osteotomy, and use of small, oblique bone tunnels for patellar fixation. The overall incidence of patellar fracture in knees receiving small, oblique bone tunnels for patellar fixation was 1 out of 215 knees (0.47% incidence), and the overall incidence of patellar fracture in knees receiving dual suture anchors for patellar fixation was 0% (Table 3).
Comparison of MPFL Reconstruction Outcomes Between the Use of Small (3.2-mm), Oblique Patellar Tunnels and Suture Anchors for Patellar Fixation a
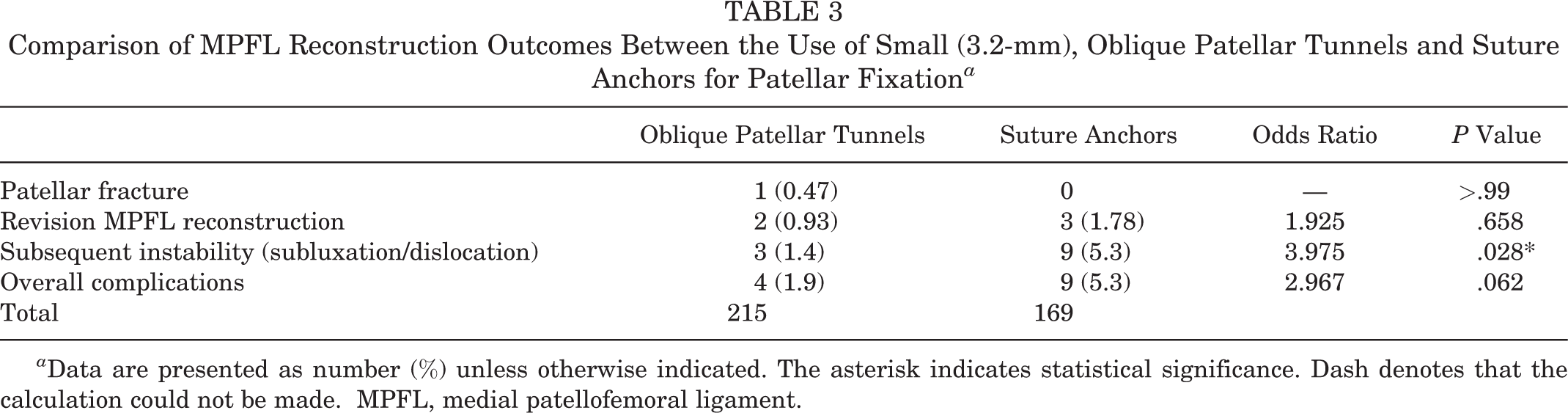
a Data are presented as number (%) unless otherwise indicated. The asterisk indicates statistical significance. Dash denotes that the calculation could not be made. MPFL, medial patellofemoral ligament.
With regard to the other primary outcomes of interest, there were 12 knees in which subsequent subluxation or dislocation events were reported, with 3 (1.4% incidence) occurring in patients who received small, oblique bone tunnels and 9 (5.3% incidence) occurring in patients who received suture anchors for patellar fixation. The use of suture anchors was associated with a statistically significant increased risk of subluxation or dislocation compared with small, oblique tunnels (odds ratio [OR], 3.98; 95% CI [1.06-14.92]; P = .028) (Table 3). These results were validated by a Firth logistic regression (P = .006) (Table 5). Five total knees required revision MPFL reconstruction, with 2 (0.93% incidence) occurring in patients who received small, oblique bone tunnels and 3 (1.78% incidence) occurring in patients who received suture anchors for patellar fixation. There was not a statistically significant difference in the need for revision MPFL reconstruction between the 2 methods for patellar fixation (OR, 1.93; P = .658) (Table 3).
Finally, we observed an overall complication rate of 3.4% (13) among all procedures included in this study. While we found an almost 3 times greater incidence of complications occurring in the group undergoing patellar fixation with suture anchors (5.3%) in comparison with the group undergoing fixation with small, oblique bone tunnels (1.9%), this difference fell short of reaching statistical significance (OR, 2.97; P = .062) (Table 3). In an effort to further isolate the impact of patellar fixation on the primary outcomes of interest, several subanalyses were undertaken to examine for confounding and determine the impact of graft type and the performance of concomitant tibial tubercle osteotomies on the incidence of patella fracture, subluxation or dislocation events, and need for revision surgery. No other statistically significant correlations with the primary outcomes were found with respect to graft type used or concomitant procedures performed (Tables 4 and 5).
Comparison of Primary Outcomes Between Anteromedializing and Distalizing Tibial Tubercle Osteotomies a

a Data are presented as number (%) unless otherwise indicated. Dash means that the calculation was unable to be performed due to the small values. MPFL, medial patellofemoral ligament.
Firth Logistics Regression Analysis Comparing the Patellar Fixation Methods Used, Graft Types, and Concomitant Osteotomies With Primary Surgical Outcomes a
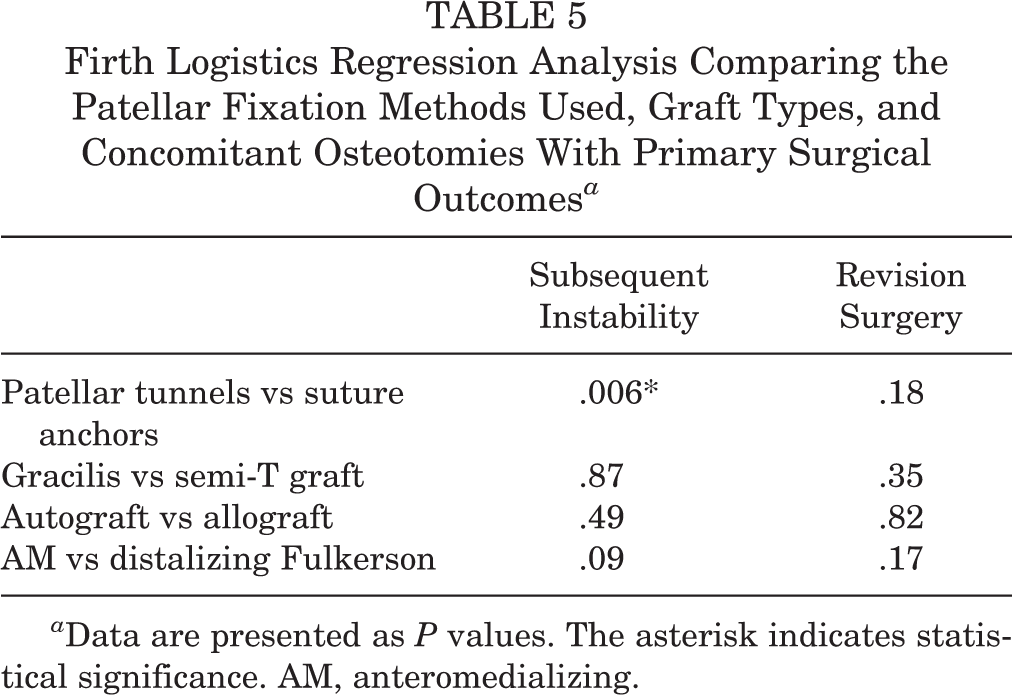
a Data are presented as P values. The asterisk indicates statistical significance. AM, anteromedializing.
Discussion
Our study includes the largest series to date on outcomes with the use of small (3.2-mm), oblique patellar tunnels. The most important finding from our study was that the use of small (3.2-mm), oblique patellar bone tunnels was not associated with an increased risk of patellar fracture in comparison with the use of suture anchors for patellar fixation. Patellar fractures as a complication after MPFL reconstruction have been reported multiple times in the literature, particularly in association with 4.5-mm transverse patellar tunnels. 5,13,16,27 Many of the descriptions of patellar fractures after MPFL reconstruction occur in case reports or small case series, which has made the true incidence of patellar fractures difficult to elucidate. 2,5,7,8,11 –13 Recently, separate independent studies by Parikh et al 18 and Schiphouwer et al 23 described the incidence of patellar fracture with the use of 4.5-mm, transverse bone tunnels in larger series. Parikh et al reported 6 patellar fractures in a series of 179 knees undergoing MPFL reconstruction (3.35% incidence). Moreover, Schiphouwer et al found a similar incidence of patellar fractures using this technique, with fractures occurring 7 times in a series of 192 knees (3.65% incidence). As larger bone tunnels can create stress risers that increase the risk of fracture, proponents of suture anchor fixation have cited this as rationale for favoring their use. 14 Our study’s findings are significant as there was no increased risk of patellar fracture with the use of smaller (3.2-mm), oblique patellar bone tunnels.
In addition to establishing noninferiority of small, oblique 3.2-mm tunnels with regard to the risk for patellar fracture, the use of small oblique tunnels was associated with a 3 times less likelihood for recurrent subluxation or dislocation events in comparison with the use of suture anchors for patellar fixation. Within the scope of our study, it is not clear what factors led to this decreased risk of subluxation or dislocation events, but it is possible that these factors could be in part due to the biomechanical strength of graft fixation. Anchor pullout is possible with any anchor, while osseous tunnels and a looped graft eliminate that possibility. Previously, the use of patellar bone tunnels with interference screw fixation was seen as being biomechanically stronger than the use of suture anchors. 21 However, the same authors showed that suture anchor fixation still provides for a reconstruction that withstands greater loads before failure in comparison with the native MPFL. 21 Various technique differences among surgeons performing these procedures could also contribute to differences in recurrent instability. Additionally, concomitant osseous procedures were performed in 127 out of 215 (59.1%) of the small, oblique tunnel reconstructions, while concomitant osseous procedures were only performed in 55 out of 169 (32.5%) reconstructions that utilized suture anchors. In our study, the lower rate of subluxation events seen in the small, oblique tunnel cohort could possibly be attributed to the higher rate of addressing other underlying anatomic risk factors that predispose patients to recurrent instability at the same time as the MPFL reconstruction. Importantly, even though our study found an increased risk of recurrent subluxation or dislocation events with the use of suture anchors, we did not find that this led to a significantly increased incidence of revision surgery compared with the use of small, oblique patellar tunnels.
The use of small (3.2-mm), oblique patellar tunnels also offers several other advantages and disadvantages in comparison with the use of suture anchors. The use of looped grafts through oblique tunnels leads to an increase in tendon-to-bone contact for healing and offers a more cost-effective option by eliminating 2 suture anchors. 14 The 3.2-mm drill bit used to create the small, oblique tunnels costs $84 (Synthes Implant Pricing, 2012) but can be reused. 26 When also factoring in the added cost of each suture anchor and an allograft (approximately $1100), it is possible to realize savings of greater than $1200 per case. 28 The drawbacks of using small, oblique patellar tunnels remain the risk of articular surface violation and the need for a longer graft. 14 While the use of suture anchors for patellar fixation has its drawbacks, it is likely to remain a commonly utilized option for patellar fixation during MPFL reconstruction because of its track record of good outcomes and surgeon preference. 6,11,12,15,17,25,28 Further research should continue to compare outcomes and complications between these 2 methods as well as investigate other factors that can influence the success of MPFL reconstruction. For example, it remains unclear whether there is an underlying reason why our study found that MPFL reconstructions utilizing small, oblique bone tunnels and semitendinosus graft were approximately 22 times more likely to require revision surgery compared with the use of small, oblique bone tunnels and gracilis graft. However, this finding could be influenced by the relatively small number of patients undergoing oblique tunnel fixation using a semitendinosis graft (n = 27) compared with a gracilis graft (n = 249).
The main limitation of this study is its retrospective nature. As such, there was no standardization in protocol regarding postoperative management. It is also possible that patients may have been seen at an outside facility for patellar fracture, subluxation or dislocation events, or revision surgery, and we would not have been able to identify this occurrence. There is no reason, however, to believe that this loss of follow-up would differ between the small, oblique tunnel and suture anchor groups. Additionally, as nearly half of our knees (49.0%) did not undergo isolated MPFL reconstruction, but rather had other concomitant osseous procedures, it is unclear the influence that these adjunctive procedures could have had on outcome, although no significant correlation was observed using multiple subanalyses. Despite these limitations, the very large sample size contained within this study helps to reduce the effects that confounding variables or isolated lack of capture may have had on the results of the study.
Conclusion
Compared with the use of suture anchors for patellar fixation, the use of small (3.2-mm), oblique bone tunnels is not associated with an increased risk for patellar fracture. The use of small, oblique bone tunnels also results in a decreased risk of recurrent subluxation or dislocation events. The use of small (3.2-mm), short, oblique patellar tunnels led to an almost 3 times decrease in overall complications among our study group in comparison with the use of suture anchors for patellar graft fixation. Small (3.2-mm), short, oblique patellar tunnels can be a safe and reliable method of patellar graft fixation in MPFL reconstruction.
Footnotes
Final revision submitted April 8, 2020; accepted April 22, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.R.D. has received research support from Aesculap/B. Braun, Moximed, and Zimmer; consulting fees from DePuy Mitek/Medical Device Business Services; and royalties from Smith & Nephew and Springer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the University of Virginia Institutional Review Board for Health Sciences Research (study No. 21389).