
Abstract
Background:
A musculocutaneous nerve (MCN) injury is a rare complication of the Latarjet procedure. Most of these injuries are neurapraxias and resolve with time; however, permanent injuries can occur. Understanding the anatomy and relationship of the MCN to the coracoid process is essential to prevent injuries.
Purpose:
To provide realistic, in situ–referenced measurements for the Latarjet procedure.
Study Design:
Descriptive laboratory study.
Methods:
A total of 12 matched-pair cadaveric specimens (24 fresh-frozen shoulders) were dissected. Coracoid osteotomy was performed, and the MCN and its respective twigs were identified. Measurements were made from the coracoid process to the entry site of the nerve twigs and trunk into the coracobrachialis muscle.
Results:
Overall, 70.8% of specimens had twigs; however, there was a discrepancy in the presence (41.7%) and number (75.0%) of twigs in the paired specimens. The most proximal twigs were, on average, 33.5 ± 8.1 mm (range, 21.9-47.6 mm) from the coracoid process. The main trunk was, on average, 51.1 ± 14.4 mm (range, 16.7-71.9 mm) from the coracoid process. In 33.3% of specimens, the nerve entered the coracobrachialis at a distance shorter than 5 cm below the coracoid process, and this increased to 91.7% when the twigs were accounted for.
Conclusion:
The previously described safe zone of 5 cm below the coracoid process may not be reliable to protect the MCN or its twigs. Using 3 cm would decrease the chances of damaging a twig or the main trunk. In 33.3% of the specimens, the nerve entered the coracobrachialis at a distance shorter than 5 cm below the coracoid process, and this increased to 91.7% when twigs were accounted for.
Clinical Relevance:
As the Latarjet procedure is an emerging technique, it is essential to be aware of the anatomic structures and the relation between different neural structures to anatomic points of reference. Therefore, the results of this study add significant information for a safe surgical procedure for the majority of patients suffering from shoulder instability.
Keywords
Surgical approaches to address anterior shoulder instability involve coracoid osteotomy to perform coracoid transfer for the Latarjet procedure. This technique requires mobilization of the coracoid process and rerouting of muscles on the coracoid, which can result in injuries to the neurovascular structures around the coracoid, specifically the musculocutaneous nerve (MCN). 2,4 This nerve courses anteriorly through the arm to provide motor innervation to the coracobrachialis through a number of twigs, as described by Flatow et al. 4 The MCN has been cited to be approximately 5 cm from the base of the coracoid, and this area has been referred as the safe zone for orthopaedic shoulder surgery. 1,5,8,11 –13
Michel Latarjet was one of the first surgeons to study the anatomy of the nerve in relation to the coracoid process. 9 He observed a number of twigs branching off the MCN to innervate the coracobrachialis before the main nerve penetration. Twigs were noted as anywhere between 20 and 120 mm, with a majority between 30 and 78 mm. 6 Although rare, a neurovascular injury can occur in anterior shoulder instability procedures. The vast majority of these injuries are temporary neurapraxias; however, lesions causing permanent damage have been reported. The incidence of neural lesions after the Latarjet procedure is reported to be up to 18.4%. 15 If the MCN is considered only, the rate drops down to about 5%. 3,12 –15
Understanding the relationship of the MCN to the coracoid process is crucial, as iatrogenic injuries can occur during surgical exposure of the anterior shoulder. 2 The aim of this study was to investigate the relationship of the MCN to the coracoid process and analyze the twigs branching off the MCN.
Methods
A total of 12 matched-pair, fresh-frozen cadaveric specimens (8 male and 16 female shoulders) were used (provided through MedCure). All shoulder specimens, with a mean age of 64.8 ± 9.3 years (range, 45-75 years), were thawed overnight at room temperature and dissected to define the anatomy of the MCN and its relationship to the coracoid process.
In each case, the skin and subdermal fat were removed from the shoulder. The deltopectoral interval was identified and retracted, exposing the coracoid and the clavipectoral fascia. The upper border of the pectoralis major insertion on the humerus was removed to aid in visualization. An osteotome was used to remove 2 cm of the coracoid tip, reflecting the coracoid distally (Figure 1). Care was taken not to compromise any anatomic structures. Each twig of the MCN was traced back to the main trunk, and the MCN itself was followed to the lateral cord of the brachial plexus (Figure 2). Any adhesions of the conjoined tendon to the underlying subscapularis and surrounding tissue that did not trace back to the MCN were noted and cut.
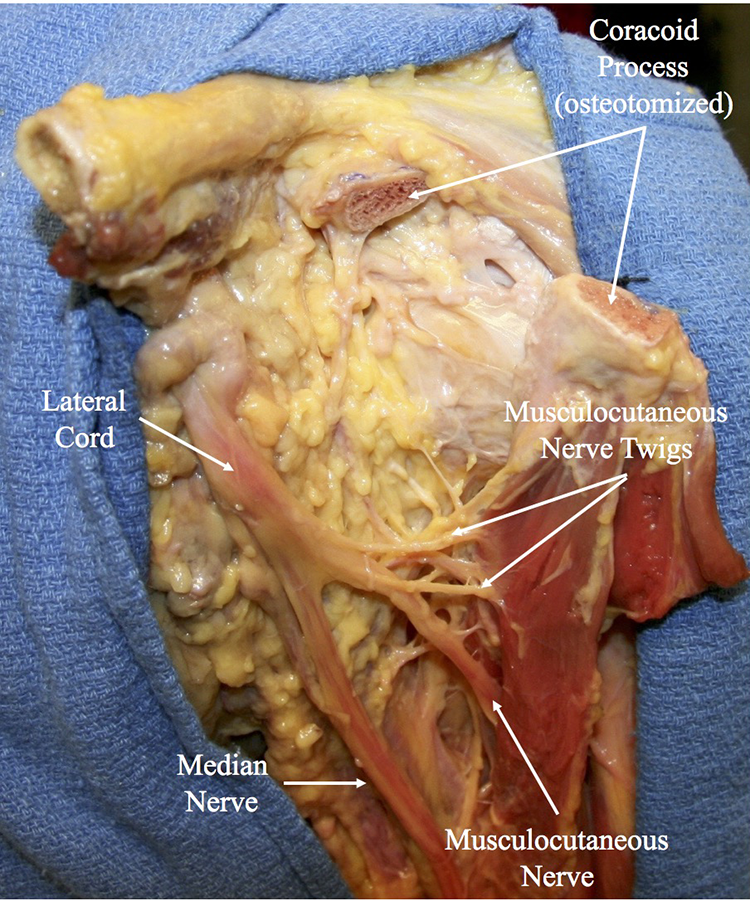
Cadaveric specimen with an osteotomized coracoid process and the conjoined tendon reflected distally to reveal the musculocutaneous nerve penetration.

Cadaveric specimen with the musculocutaneous nerve twigs and main trunk penetrating the coracobrachialis muscle.
Using a digital caliper (Mitutoyo), the distance was measured between the inferior border of the osteotomized coracoid tip and the point of penetration of the MCN into the coracobrachialis muscle. In addition, the distance was measured to the point of penetration of each nerve twig into the coracobrachialis muscle. There were 2 independent observers (H.S., J.S.Y.) who agreed on all measurements as well as the presence or absence of any twigs.
The University of Connecticut has confirmed with its institutional review board that projects conducted in our biomechanics laboratory that utilize deidentified specimens do not constitute human participant research, and therefore, no review was required.
Statistical Analysis
Descriptive results were calculated as means with standard deviations and ranges. Results were also reported as frequencies and percentages if necessary. Analysis was conducted with SPSS Version 22.0 (IBM).
Results
MCN Twigs
Each of the specimens was examined for twigs arising from the main nerve trunk. Twigs were present in 70.8% of the specimens. The first twig was noted in 17 (70.8%) specimens, entering the coracobrachialis at a mean of 33.5 ± 8.1 mm (range, 21.9-47.6 mm). A second twig was observed in 6 (25.0%) specimens, entering the coracobrachialis at a mean of 40.0 ± 4.4 mm (range, 34.1-47.1 mm). A third twig was only observed in 3 (12.5%) specimens, entering the coracobrachialis at a mean of 52.4 ± 7.3 mm (range, 45.5-60.0 mm). Table 1 lists these measurements for the 12 paired specimens.
Distance (mm) of the Entry Site of the Twigs and Main Trunk of the Musculocutaneous Nerve From the Coracoid Process a

a Dashes refer to the absence of a twig.
The measurements of the twigs were stratified according to the distance from the coracoid process (Table 2). Twigs were present at a distance of less than 3 cm in 41.2% of the specimens, 58.8% of the specimens had twigs between 3 and 5 cm, and none of the specimens had twigs at a distance of greater than 5 cm. Once a twig was identified, the mean distance to the main trunk was 22.2 ± 9.3 mm (range, 5.6-44.0 mm).
Percentages of Specimens With Twigs and the Main Trunk of the Musculocutaneous Nerve Stratified by Distance From the Coracoid Process

Main MCN Trunk
The main trunk innervated the coracobrachialis at a mean of 51.1 ± 14.4 mm (range, 16.7-71.9 mm). The most proximal main trunk was located at 16.7 mm and did not have any twigs, while the most proximal main trunk with twigs inserted into the coracobrachialis at 34.7 mm. The nerve entered the coracobrachialis muscle closer than 5 cm from the coracoid tip in 33.3% of the specimens. The measurements of the main trunk were stratified according to the distance from the coracoid process (Table 2). The main trunk was present at a distance of less than 3 cm in 8.3% of the specimens, 25.0% of the specimens had the main trunk between 3 and 5 cm, and 66.6% of the specimens had the main trunk at a distance of greater than 5 cm.
Discrepancies in Matched Pairs
The matched-pair specimens were analyzed for differences in the presence of twigs and the number of twigs. Overall, 41.7% of the specimens had inconsistencies in the presence of twigs, and 75.0% of specimens had variations in the number of twigs present (Table 3).
Discrepancies in the Matched-Pair Specimens With Respect to the Presence of Twigs and the Number of Twigs Present
Discussion
The main finding of this study was that the main trunk of the MCN entered the coracobrachialis muscle at a mean of 51.1 mm (range, 16.7-71.9 mm). Twigs were observed entering the coracobrachialis as close as 21.9 mm from the coracoid process. Based on this study, the safe zone of 5 cm below the coracoid process may place the MCN at risk, as 33.3% of the specimens had the nerve entering the coracobrachialis closer than 5 cm. This increased to 91.7% when twigs were accounted for.
Flatow et al 4 conducted an anatomic study using 93 specimens to investigate the relationship of the MCN to the coracoid process. They noted at least 1 and frequently numerous small twigs entering the coracobrachialis muscle proximal to the main trunk of the MCN. These twigs originated from the lateral cord in 7% of the specimens. The MCN penetrated the muscle at an average of 56 mm (range, 31-82 mm). However, small twigs entered the muscle as close as 17 mm, with an average distance of 31 mm. 4 The nerve entered the muscle closer than 50 mm below the coracoid in 29% of the specimens and in 74% of cases if the twigs were accounted for. 4
Clavert et al 2 investigated the anatomic relationship of the MCN and the coracobrachialis as well as the change in this relationship after coracoid transposition. The mean distance between the inferior tip of the coracoid process and nerve entry into the muscle was 55.7 mm, and the first motor twig entering the coracobrachialis was less than 50 mm in 75% of cases, with a mean value of 40.6 mm. A nerve injury was reported be a complication of the Latarjet procedure, caused by lengthening (from 47.2 to 48.43 mm) of the nerve and a change in the penetration angle (from 121° to 136°) of the nerve into the muscle. 2 A similar study was conducted by LaPrade et al, 7 who investigated the potential benefit of prior neurolysis before the Latarjet procedure. They showed the MCN entry into the conjoined tendon at a median of 57.1 mm (range, 23.5-92.9 mm) from the tip of the coracoid and after neurolysis of 56.5 mm (range, 43.0-82.2 mm) (P = .32). After the Latarjet procedure, the entry points were remeasured, and the MCN entry into the conjoined tendon was at a median of 35.6 mm (range, 27.3-84.5 mm) from the 3-o’clock position of the glenoid and 43.8 mm (range, 20.2-58.3 mm) (P = .83) for the specimens that underwent neurolysis. Therefore, they concluded that routine neurolysis may not necessarily be helpful, as the MCN did not significantly change in distances. Ozturk et al 10 conducted a cadaveric study in which 21.5% of the specimens had a distance from the coracoid process to the nerve entry shorter than 50 mm, and this increased to 76% when thin branches were accounted for.
Even though the degree of motor function resulting from these twigs is unknown, one should still be aware of their presence to avoid iatrogenic injuries, as the twigs have been reported to provide main motor innervation to the coracobrachialis. 4 However, as there have been no electromyographic or pathological analyses of the twigs, it is unclear if the twigs are mixed nerves or pure motor nerves. It is also unclear how much effect sacrificing 1 twig would have on the coracobrachialis muscle. A safe zone of 3 cm below the coracoid process appears to be reasonable, as only 37.5% of the specimens had twigs at a distance of less than 3 cm, and only 8.3% of specimens had the main trunk present at a distance of less than 3 cm. Based on our study, using the previously stated safe zone of 5 cm below the coracoid process would place 91.7% of nerve twigs and 25.0% of main nerve trunks at a risk for injuries.
When comparing the matched-pair specimens, differences in both the presence and the number of nerve twigs were observed. Overall, 41.7% and 75.0% of the matched-pair specimens differed in the presence and number of nerve twigs, respectively. Awareness of these anatomic variations is important for the surgeon to avoid iatrogenic nerve injuries.
These data are clinically important, especially during the Latarjet procedure. In our practice when performing the Latarjet procedure, after coracoid osteotomy has been performed, the surgeon dissects the twigs and main trunk of the MCN in every case. In the nerve monitoring study by Delaney et al 3 on the Latarjet procedure, the highest amount of alerts on the MCN was found when securing the coracoid process to the glenoid. We believe that our technique allows us to safely mobilize the coracoid process and conjoined tendon through the subscapularis split without putting undue pressure on the twigs and MCN.
Limitations of this study include possible variations in the anatomic identification of the entry point into the muscle, which was addressed by having 2 observers agree on measurements. The study was conducted using fresh-frozen cadaveric specimens in which physiological muscle tension was absent.
Conclusion
Innervation of the coracobrachialis by the MCN can occur in close proximity to the coracoid process. In 33.3% of the specimens, the nerve entered the coracobrachialis at a distance shorter than 5 cm below the coracoid process, and this increased to 91.7% when twigs were accounted for. Surgeons must be cognizant of these variations at the level of the nerve entry into the coracobrachialis muscle to avoid iatrogenic injuries. Awareness of this is especially important for a surgeon aiming to perform coracoid osteotomy and transfer for the surgical treatment of recurrent anterior instability of the shoulder.
Footnotes
Final revision submitted May 26, 2020; accepted June 19, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: The University of Connecticut Health Center/UConn Musculoskeletal Institute has received direct funding for this study from Arthrex; the company had no influence on the study design, data collection, or interpretation of the results or the final article. J.S.Y. has received educational support from Arthrex and DePuy Synthes. T.W. has received grants from Arthrex and Linvatec and educational support from Arthrex, Linvatec, and Smith & Nephew. R.A.A. has received educational/research support from Arthrex and DonJoy and consulting fees from Biorez and DePuy Synthes. A.D.M. has received research support from Arthrex, consulting fees from Arthrex and Astellas Pharma, and honoraria from Arthrosurface. A.V. has received consulting fees from DJO Global. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.