
Abstract
Background:
Radiographic tibiofemoral (TF) osteoarthritis (OA) is common in patients after anterior cruciate ligament (ACL) reconstruction at long-term follow-up. The association between radiographic OA and patient-reported outcomes has not been thoroughly investigated.
Purpose:
To determine the association between radiographic TF OA and patient-reported outcome measure (PROM) scores at 16 years after ACL reconstruction.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This study was based on 2 randomized controlled studies comprising 193 patients who underwent unilateral ACL reconstruction. A long-term follow-up was carried out at 16.4 ± 1.7 years after surgery and included a radiographic examination of the knee and recording of PROM scores. Correlation analyses were performed between radiographic OA (Kellgren-Lawrence [K-L], Ahlbäck, and cumulative Fairbank grades) and the PROMs of the International Knee Documentation Committee (IKDC) subjective knee form, Lysholm score, and Tegner activity scale. A linear univariable regression model was used to assess how the IKDC score differed with each grade of radiographic OA.
Results:
Of 193 patients at baseline, 147 attended the long-term follow-up. At long-term follow-up, 44.2% of the patients had a K-L grade of ≥2 in the injured leg, compared with 6.8% in the uninjured leg. The mean IKDC score at follow-up was 71.2 ± 19.9. Higher grades of radiographic OA were significantly correlated with lower IKDC and Lysholm scores (r = –0.36 to –0.22). Patients with a K-L grade of 3 to 4 had significantly lower IKDC scores compared with patients without radiographic OA (K-L grade 0-1). Adjusted beta values were –15.7 (95% CI, –27.5 to –4.0; P = .0093; R 2 = 0.09) for K-L grade 3 and –25.2 (95% CI, –41.7 to –8.6; P = .0033; R 2 = 0.09) for K-L grade 4.
Conclusion:
There was a poor but significant correlation between radiographic TF OA and more knee-related limitations, as measured by the IKDC form and the Lysholm score. Patients with high grades of radiographic TF OA (K-L grade 3-4) had a statistically significant decrease in IKDC scores compared with patients without radiographic TF OA at 16 years after ACL reconstruction. No associations were found between radiographic TF OA and the Tegner activity level.
Keywords
With the rapid development of anterior cruciate ligament (ACL) reconstruction techniques during the past few decades, outcomes after ACL reconstruction in terms of function and joint stability of the knee have consistently improved. 5 However, when looking at long-term follow-up studies (>10 years), a significant proportion of patients have reported high levels of knee pain and low activity levels. 21,30
The contributory causes of impairment of knee function in these patients are still uncertain. Although normal aging and continued instability of the knee surely explain some of the reduction in activity level at 15 years after ACL reconstruction, other variables associated with surgical results may also explain these findings. Radiographic knee osteoarthritis (OA) is found in up to 50% of patients at 10 to 20 years after an ACL injury 23 and could be regarded as a likely contributor. However, the general association between radiographic OA and patient-reported outcomes has often been discordant in the literature, with some studies reporting weak associations and a high prevalence of asymptomatic patients with prevalent radiographic OA. 2,14 While inconsistency in the recording and classification of outcome scores, radiographic classification systems, and cutoff limits may account for some of the reported variability across studies, 2,32 other variables, such as psychosocial factors, may influence the experience of pain and may account for some of the reported discordance. 16,26,33
In light of this research, the association between radiographic tibiofemoral (TF) OA and patient-reported outcomes among patients undergoing ACL reconstruction needs to be investigated. To date, few studies have investigated the association between radiographic TF OA and patient-reported outcomes when looking at long-term follow-up after ACL reconstruction (>10 years). 9,28 Moreover, few studies have accounted for the severity of radiographic TF OA but have instead compared mean scores for those with and without radiographic TF OA, and they have not focused exclusively on patients undergoing ACL reconstruction. 25,27 One of the longest follow-up studies to date that has considered the severity of radiographic TF OA, published by Oiestad et al, 28 reported that patients with severe radiographic TF OA (Kellgren-Lawrence [K-L] grade 4) had significantly lower scores on all subscales of the Knee injury and Osteoarthritis Outcome Score (KOOS) at 10 to 15 years after ACL reconstruction. When looking at other outcome measures and radiographic classification systems, studies are lacking.
Considering the emphasis placed on the prevalence of radiographic OA in studies evaluating results after ACL reconstruction, there is a need to further examine the association between radiographic TF OA and patient-reported outcomes in patients who have undergone ACL reconstruction. The aim of this study was to determine the association between 3 different patient-reported outcome measures (PROMs) and 3 commonly used radiographic OA classification systems at 16 years after ACL reconstruction. It was hypothesized that radiographic TF OA would be associated with lower scores for the examined PROMs.
Methods
Patients
The study population in this long-term follow-up study consisted of a merger of 2 cohorts from 2 previous randomized controlled trials. 4,10,20 Patients in the original cohorts had sustained a unilateral ACL rupture and were treated surgically using ipsilateral hamstring tendon (HT) or bone–patellar tendon–bone (BPTB) autografts. Patients were included in the cohorts if they had an isolated, complete ACL rupture. Patients with and without concurrent meniscal injuries (defined as involving less than one-third of the meniscus) or minor chondral lesions (Outerbridge grade 1 or 2) were included in the original cohorts. Patients with multiligament injuries or excessive chondral lesions that required surgical interventions other than debridement were excluded. Patients who sustained an ACL injury during contact and noncontact activities were included. Patients who had undergone previous ACL reconstruction were excluded. Patients were randomized preoperatively to graft choice as described in the original studies by Laxdal et al 20 and Ejerhed et al. 10 Because cohorts from 2 previous randomized controlled trials were included, the HT graft group consisted of 3 different HT graft types. ACL reconstruction was all carried out between September 1995 and January 2000. The reconstruction procedures were performed at 3 different locations and conducted by 1 of 6 different surgeons. Patients who sustained an additional reinjury during the follow-up period and patients who required additional surgical interventions for their knee during follow-up were all included in the study.
Surgical Technique and Rehabilitation
The surgical technique for both the HT and the BPTB graft groups has been described thoroughly in the original studies by Laxdal et al 20 and Ejerhed et al. 10 Patients underwent ACL reconstruction using either a transtibial or a medial portal along with HT and BPTB autografts, according to the original studies. 10,20 Rehabilitation for all the patients was similar, with immediate full weightbearing activity through full range of motion allowed. Closed kinetic chain exercises were commenced immediately after surgery. External loads from 30° of flexion through hyperextension were avoided during the first 6 weeks after surgery. After 3 months, running was allowed, while contact sports were allowed after 6 months at the earliest, provided that patients had attained full strength, coordination, and balance compared with that of the contralateral leg during functional testing.
Clinical Assessment and Follow-up
The PROMs of the Tegner activity scale, 31 Lysholm score, 31 and International Knee Documentation Committee (IKDC) subjective knee form 17 were used to evaluate patient-reported outcomes at a mean time of 16.4 years after surgery. The Tegner activity scale, the IKDC form, and the Lysholm score are knee-specific PROMs used to evaluate symptoms, patient function, and sports activity level in patients with a large variety of knee conditions, including patients undergoing ACL reconstruction. The Tegner activity scale measures activity levels from 1 to 10, with 1 being the least knee-strenuous activity. The IKDC form has scores ranging from 0 to 100 to measure symptoms, function, and sports activity. For the Lysholm score, a score ranging from 0 to 100 is calculated based on 8 different symptom domains evaluating both function and more subjective measures, such as pain and instability. For both the IKDC form and the Lysholm score, a score of 100 indicates no knee-related symptoms. A preoperative evaluation was performed by several independent physical therapists, and a long-term clinical follow-up was performed by 1 research assistant (D.S.). These examiners had not been involved in the surgical procedure or rehabilitation of the patients.
Radiographic Assessment
Standard weightbearing radiographic imaging, including frontal, lateral, and patellofemoral skyline projections of the knee, of both the injured and contralateral knees at long-term follow-up was performed. The K-L, Ahlbäck, and cumulative Fairbank grades were used to assess radiographic TF OA. 1,11,19 The K-L classification system is used to evaluate radiographic OA and accounts for both osteophytes and joint space narrowing (JSN) on a scale from 0 to 4, with grade 2 most commonly set as the cutoff for prevalent radiographic OA. 19 The Ahlbäck system grades radiographic OA based solely on JSN on a scale from 0 to 5, with grade ≥1 being considered prevalent radiographic OA. 1 For the cumulative Fairbank system, the cumulative number of positive findings, ranging from 0 to 6, is calculated for each patient. Findings are rated dichotomously based on joint flattening, narrowing, and ridging. 22 Patellofemoral radiographic OA was classified as none (0), mild (1), moderate (2), or severe (3). 22 The radiographic assessments were performed by a senior radiologist, specializing in orthopaedic radiography. The intrarater reproducibility of the radiologist in the study had kappa values ranging between 0.55 and 1.00 for the Ahlbäck and Fairbank grades. 22
Statistical Analysis
Descriptive data and inference were calculated using the statistical analysis software SAS 9.4 for Windows (SAS Institute). Descriptive data were reported as means with SDs and medians with range. The Spearman rank correlation was used to analyze correlations between radiographic TF OA according to the K-L, Ahlbäck, and cumulative Fairbank grades and the PROMs of the IKDC form, Lysholm score, and Tegner activity scale. The Spearman rank correlation coefficients were graded according to the classification system of Chan 6 as poor, fair, moderately strong, or very strong. A linear univariable regression model was used to investigate how radiographic TF OA according to the K-L grade affected patient-reported outcomes according to the IKDC score. Age and sex were adjusted for confounding in all the analyses because female sex and older age have both been associated with worse knee symptoms, function, and the development of knee OA. 12,29 Significance levels were set at .05.
Results
A total of 193 patients were eligible from the original cohorts (Figure 1), and 147 of these patients attended the long-term follow-up at, on average, 16.4 ± 1.7 years after ACL reconstruction (95 male and 52 female). Overall, 86 (58.5%) patients underwent ACL reconstruction using an HT autograft, while 61 (41.5%) received a BPTB autograft (Table 1). The mean time from ACL injury to reconstruction was 34.5 ± 54.8 months, and the mean age at the time of ACL reconstruction was 27.3 ± 8.3 years (Table 1). Concomitant injuries in addition to the ACL tear were found in 97 (66%) of 147 patients at baseline. Minor meniscal injuries accounted for 74 out of 97 (76.3%) of these injuries (Table 2).
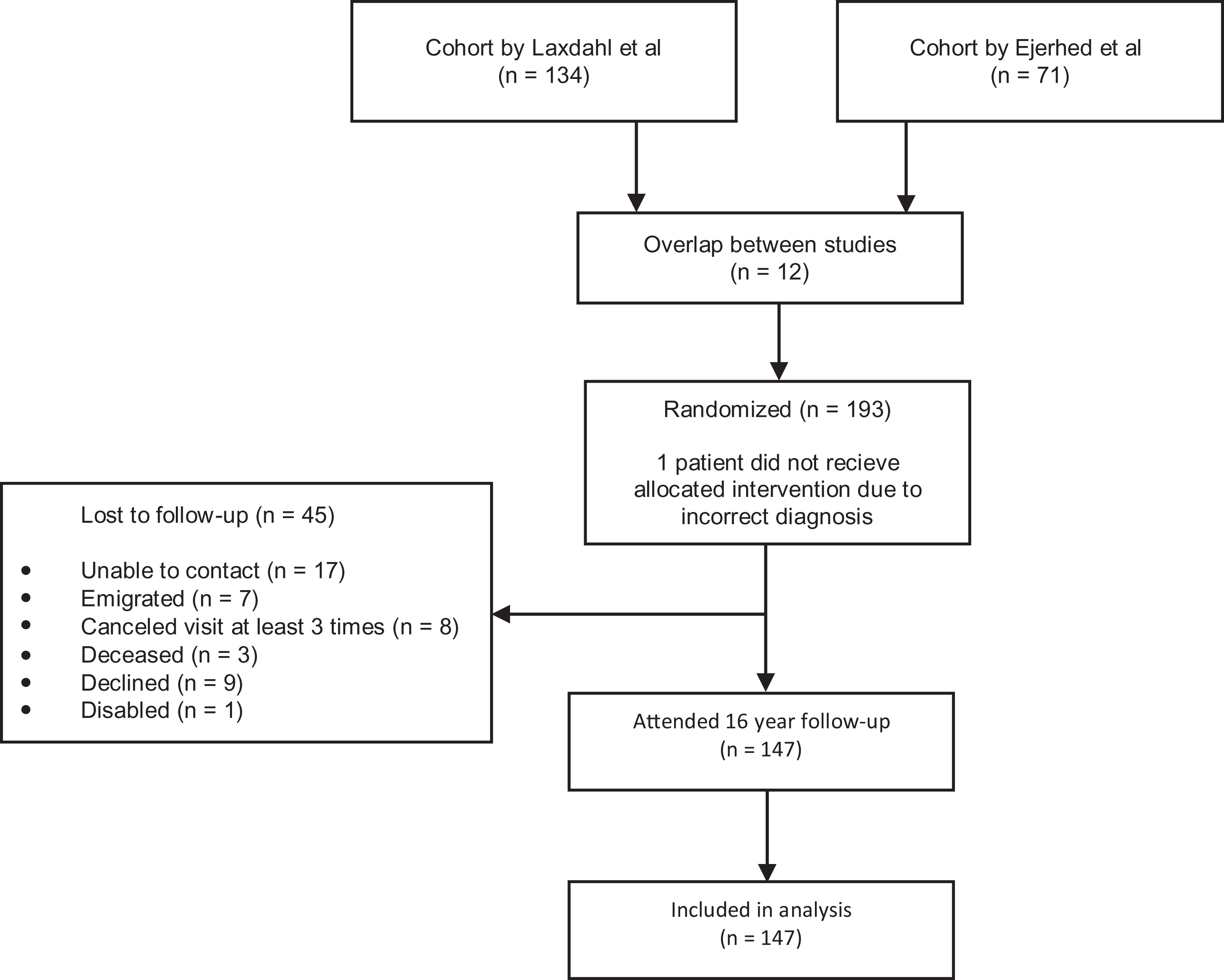
Flowchart of included patients.
Baseline Characteristics (n = 147) a

a Values are presented as n (%) or mean ± SD/median (range). ACL, anterior cruciate ligament.
Associated Minor Injuries at Surgery for Each K-L Grade a
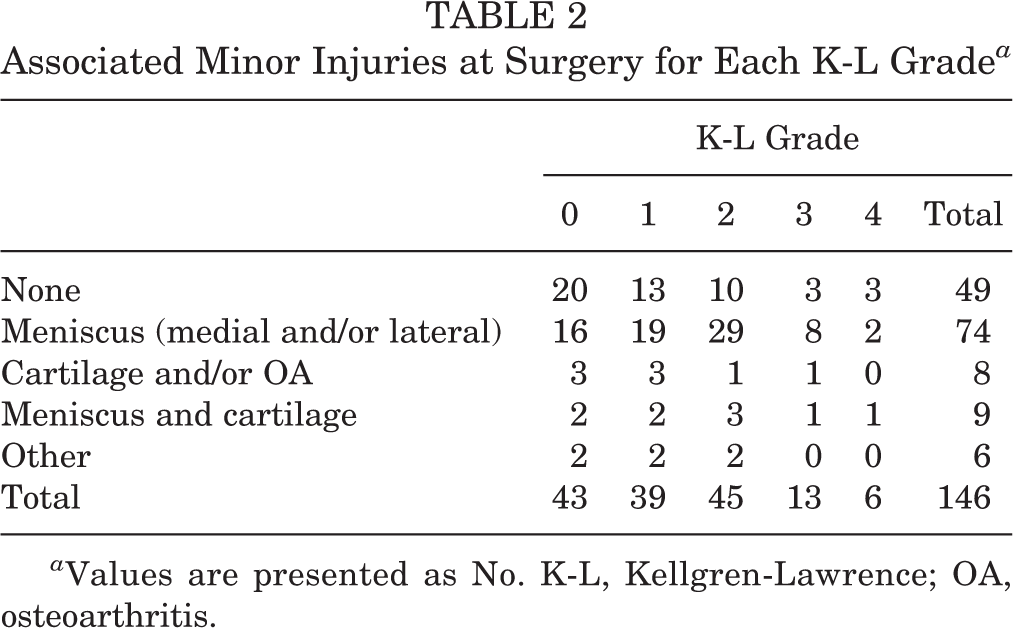
a Values are presented as No. K-L, Kellgren-Lawrence; OA, osteoarthritis.
Of the 147 patients, 74 (50.3%) underwent additional knee surgery during the follow-up period, and the causes of additional surgery during follow-up are presented in Table 1. At follow-up, 44.2% of the patients had a K-L grade of ≥2 on their injured side compared with 6.8% on the uninjured side (Table 3). Radiographic patellofemoral OA was present in 18 (12.2%) of 147 patients (Table 3). The mean IKDC score at follow-up was 71.2 ± 19.9, and the mean Lysholm score at follow-up was 80.2 ± 16.0 (Table 4).
Radiographic Findings

PROM Scores at Follow-up a

a Values are presented as n (%) or mean ± SD/median (range). IKDC, International Knee Documentation Committee; PROM, patient-reported outcome measure.
Table 5 presents the unadjusted and adjusted correlations between the analyzed PROMs and the different radiological classification systems. Higher grades of radiographic TF OA according to the K-L, cumulative Fairbank, and Ahlbäck medial-side grades were significantly correlated with lower IKDC and Lysholm scores (r = –0.36 to –0.22). There were no significant correlations between the Tegner activity scale and any of the radiological classification systems. The Ahlbäck lateral-side grade was not correlated with any of the analyzed PROMs. Figure 2 presents the mean scores for each PROM for each K-L grade. In the linear regression model, patients with grades 3 and 4 radiographic TF OA according to the K-L classification system had significantly lower IKDC scores than did patients without radiographic TF OA (K-L grade 0-1). The adjusted beta value for K-L grade 3 was –15.7 (95% CI, –27.5 to –4.0; P = .0093; R 2 = 0.09) and for K-L grade 4 was –25.2 (95% CI, –41.7 to –8.6; P = .0033; R 2 = 0.09) (Table 6).
Correlation Between Radiographic TF OA and PROMs a

a IKDC, International Knee Documentation Committee; K-L, Kellgren-Lawrence; OA, osteoarthritis; PROM, patient-reported outcome measure; rs , Spearman correlation coefficient; TF, tibiofemoral.
b Adjusted for sex and age using partial correlation.
cStatistically significant.

Patient-reported outcome measure (PROM) scores for each Kellgren-Lawrence grade. IKDC, International Knee Documentation Committee. X, O, + within the box, means; horizontal bar inside the box, median; upper limit of the box, 75% percentile; lower limit of the box, 25% percentile; IQR, within the upper and lower limits of the box; X, O, + outside the box, outliers; lower end of whisker, minimum observation above lower fence; upper end of whisker, maximum observation below upper fence.
Univariable Linear Regression of IKDC Score for K-L Grades a

a Beta, P, and R 2 values are based on original values and not on stratified groups. IKDC, International Knee Documentation Committee; K-L, Kellgren-Lawrence.
b Adjusted for sex and age using linear regression.
Discussion
The main result of this study was that TF OA according to the K-L, cumulative Fairbank, and Ahlbäck medial-side grades showed poor but statistically significant correlations with more knee-related limitations according to the PROMs of the IKDC form and Lysholm score. In addition, grades 3 and 4 radiographic TF OA, according to the K-L score, explained inferior results according to the IKDC score in the linear regression model. Only a small part of the variance in the regression model was, however, explained by radiographic TF OA based on the coefficient of determination of the model.
This study is one of few that have examined the association between radiographic TF OA and long-term knee function in patients who have undergone ACL reconstruction. This study also examined several PROMs and radiographic OA classification systems, which provide comprehensive knowledge when evaluating surgical results at long-term follow-up after ACL reconstruction.
A study similar in design to the present study, published by Oiestad et al, 28 has previously examined the association between radiographic TF OA and patient-reported outcomes at 10 to 15 years after ACL reconstruction. Oiestad et al reported significantly lower scores on all subscales of the KOOS for patients with severe radiographic TF OA (K-L grade 4) compared with those without radiographic TF OA. The present study confirms these results, with significantly lower IKDC scores reported for patients with radiographic TF OA of K-L grades 3 and 4. A relevant difference between this study and the study by Oiestad et al is the use of different PROMs for evaluating prevalent symptoms, with Oiestad et al using the KOOS and the present study instead using the IKDC form and the Lysholm score for symptom evaluation. Another study conducted by Culvenor et al, 9 also examining radiographic TF OA at 5 to 10 years after ACL reconstruction, reported, in contrast to Oiestad et al, that the severity of radiographic TF OA was not associated with increased symptoms among patients, with the exception of the KOOS subscale of pain. Additional studies evaluating the association between radiographic TF OA and prevalent symptoms among patients with ACL injury have found inferior KOOS scores for patients with radiographic TF OA compared with those without radiographic TF OA. 24,25 These studies did not, however, focus exclusively on patients who had undergone ACL reconstruction but instead on patients with ACL injuries. In addition, these studies did not take radiographic severity into account in their analysis. Instead, only patients with and without radiographic TF OA were compared. 24,25
In the study by Oiestad et al, 28 it was reported that all subscores of the KOOS were inferior for those with severe radiographic TF OA. Certain subscales, however, such as knee-related quality of life and function in sports and recreation, showed the greatest decrease in scores. 28 The present study did not investigate the association between radiographic TF OA and individual subscales of symptoms in each PROM and therefore adds no additional knowledge relating to whether certain symptom domains are more closely related to radiographic TF OA. It is, however, worth noting that the present study found no significant correlations between the Tegner activity level and radiographic TF OA, which is similar to the results of Oiestad et al who also found no difference in the Tegner activity level when comparing patients with and without radiographic TF OA. It is therefore evident that, although patients with prevalent radiographic TF OA experience more symptoms than those without, activity levels generally decline independently of the development of radiographic TF OA. 30
Even though the present study found significant correlations between radiographic TF OA and the IKDC form and Lysholm score, the strength of the correlations was mainly poor. 6 The correlations remained statistically significant when adjusted for age and sex. Supporting the poor correlations of the Spearman correlation analysis, the regression model also showed weak associations, with an R 2 value for grades 3 and 4 radiographic TF OA of only 0.09.
When considering the patient implications of the findings of the regression model that high-grade radiographic TF OA explained inferior PROM scores, the study by Irrgang et al 18 evaluating the responsiveness of the IKDC form showed that a 15-point decrease in the IKDC score reflected substantially worse symptoms. Interestingly, in the present study, the beta values for patients with grades 3 and 4 radiographic TF OA exceeded this cutoff value compared with those for patients without radiographic TF OA. 18 Considering the R 2 value of the model, the strength of the regression model was, however, low, indicating that only 9% of the presented variance could be explained by radiographic TF OA.
Based on the results of this study, high-grade radiographic TF OA could be regarded as a likely contributor to inferior outcomes at long-term follow-up, but it should only be regarded as a small part of the puzzle when attempting to determine the genesis of impairment among patients after ACL reconstruction. Low-grade radiographic TF OA after ACL reconstruction appears less likely to explain inferior outcomes among patients undergoing ACL reconstruction. When evaluating surgical methods for ACL reconstruction, based on these results, radiographic TF OA is an altogether relevant outcome measure. Many other variables may, however, also contribute to a patient’s experience of pain and also naturally affect impairment and function, as described by the widely accepted biopsychosocial model of pain. 13 Considering that the associations between radiographic TF OA and self-reported symptoms among patients undergoing ACL reconstruction in previously mentioned studies have also been weak, this indicates that a weak association between radiographic TF OA and patient-reported outcomes at long-term follow-up after ACL reconstruction is plausibly evident.
When examining the association between radiographic OA and patient-reported outcomes among other cohorts, previous systematic reviews, such as that by Bedson and Croft, 2 have reported large interstudy variability across studies, with associations varying dependent on both radiographic views and radiographic classification systems used. Different classification systems focus on different radiological features, with some considering osteophytes and other systems, such as the Ahlbäck system, focusing solely on JSN. This could, of course, affect the grading cutoff. The results in this study, with very few patients having high-grade radiographic TF OA (grade 3-4) according to the Ahlbäck grade, may suggest that the grading system is not sensitive enough for a diagnosis of radiographic TF OA in the context of this study. Previous comparisons between the Ahlbäck and K-L classification systems have indicated greater intraobserver reliability but weaker correlations with arthroscopic findings for the Ahlbäck grade, which may contribute to the findings. 32 The correlations may also have been affected by the small number of patients with severe radiographic TF OA according to the Ahlbäck grade. In addition, osteophytes have been suggested to be associated more accurately with greater pain compared with that of JSN, 7 which may also be part of the explanation of why the K-L and cumulative Fairbank grades had stronger correlations with the examined PROMs than did radiographic TF OA according to the Ahlbäck lateral-side grade.
The strengths of this study include the large number of patients as well as the fact that patients were unaware of the radiological state of their knee at long-term follow-up. The potential nocebo effect commonly attained when patients are aware of the negative radiographic state of their body was therefore eliminated, removing the risk that patients had attained psychological contributors known to increase the experience of pain based on the results of their radiographs. 3,8,15 Multiple surgeons involved in the surgical procedure as well as the mix between BPTB and HT grafts can also be considered a strength of the study.
This study has some limitations. One obvious limitation of this study was the inability to differentiate between symptoms potentially originating directly from ACL surgery and injuries and the symptoms originating from prevalent radiographic OA because the examined PROMs include questions on sporting activity level, pain, and giving way in the knee, which could be attributed to both the results of ACL reconstruction and radiographic symptomatic OA. Moreover, a high percentage of the patients at baseline had injuries in addition to their ACL injury, with these patients being evenly distributed among the different K-L grades at long-term follow-up. In addition, 50.3% underwent additional surgery during the follow-up period, and it is therefore possible that additional injuries sustained during the follow-up period may also have contributed to an increase in symptoms among patients, as additional surgery was not adjusted for in the correlation and regression models. Further research is needed to provide information about the relative importance of other possible contributors to long-term outcomes after ACL reconstruction.
With a dropout rate of 46 patients at long-term follow-up from the initial 193 patients at baseline, a potential risk of skewness in the study population at follow-up compared with baseline cannot be ruled out especially because a dropout analysis was not carried out. Last, radiographic classification in the present study only accounted for radiographic TF OA and not radiographic patellofemoral OA, which could be regarded as a limitation because radiographic patellofemoral OA has been reported to be associated with more knee pain and increased knee-related symptoms than has radiographic TF OA. 9
Conclusion
There was a poor but significant correlation between radiographic TF OA and more knee-related limitations, as measured using the IKDC form and the Lysholm score. Patients with high grades of radiographic TF OA (K-L grade 3-4) had a statistically significant decrease in IKDC scores compared with that in patients without radiographic TF OA at 16 years after ACL reconstruction. No associations were found between radiographic TF OA and the Tegner activity level.
Footnotes
Final revision submitted March 10, 2020; accepted April 3, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research funding was received from the Western Sweden County Council (to J.K.). J.K. has been a lecturer for ConMed Sweden. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics review board of Gothenburg.