
Abstract
Background:
Athletic endeavor can require the “athletic shoulder” to tolerate significant load through supraphysiological range and often under considerable repetition. Outcome measures are valuable when determining an athlete’s safe return to sport. Few data are available to guide a clinician’s choice from the variety of measures available.
Purpose:
To describe the use of quantifiable objective outcome measures and patient-reported outcome tools after glenohumeral joint stabilization, specifically in an athletic population. The secondary aim of our study was to assess whether the method of measurement used was clearly described and standardized to aid clinical interpretation.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic search of MEDLINE, Scopus, SPORTDiscus, and Web of Science databases was performed in December 2018 based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. After the application of selection criteria, a full review of identified papers, and screening of reference lists, a total of 62 studies were included in the review. All studies were independently appraised for quality, predefined data fields were populated and cross-checked for accuracy, and results were then summarized from these data fields.
Results:
Of the 62 included studies, 94% used a quantifiable objective clinical outcome. A majority (85%) of the studies measured range of motion, 21% recorded muscle strength, 5% measured electromyographic activity, 5% examined shoulder kinematics, and 3% assessed joint proprioception after surgery. However, only 18% of the studies clearly described a standardized method of measuring the outcome. Nearly all (95%) of the studies used at least 1 patient-reported outcome measure. The Rowe score was most commonly used (35%).
Conclusion:
We must standardize and clearly describe the use of quantifiable objective outcome measures to aid clinical interpretation. A concerted effort should also be made to standardize the use of patient-reported outcome tools after shoulder stabilization in the athletic population.
Keywords
Shoulder instability may present as pain or a sense of displacement (subluxation or dislocation), caused by a combination of structural (traumatic and atraumatic) and neurological system disturbances. 54 It is a relevantly common complaint in the athletic population, as many athletic pursuits are extremely demanding of the shoulder. 19,48 During overhead sports such as baseball and swimming, the shoulder joint must withstand significant repetitive loads, often in ranges that exceed normal physiological parameters. In contact sports such as American football, rugby, and wrestling, direct traumatic instability may result. Performance may be limited, or in many cases inhibited, and athletes often undergo reconstructive surgery for symptoms of shoulder instability. 19 Despite surgical reconstruction of injured structures, a relatively high frequency of further shoulder instability occurs, most notably in young athletes in contact sports (5.9%-51%). 2,92,107 It remains unclear when athletes can safely return to sport (RTS) after glenohumeral joint stabilization and what criteria surgeons and clinicians should use to guide their decision making. Furthermore, the decision to return an athlete to competition has significant implications ranging from the safety of the athlete to performance factors and litigation issues.
Outcome measures play a key role in informing RTS decision making. A battery of tests, including patient-reported outcome (PRO) measures, clinical objective measurements, and sport-specific functional tests, are often used to determine an athlete’s readiness to RTS after lower limb injuries. 7,30 Clinical tests are used to assess specific impairments (eg, muscle strength, range of motion). 87 Functional tests assess overall function, providing information on specialized movements in sport, exercise, and occupations; for example, the countermovement jump, a functional test of the lower limb, is not an isolated assessment of knee function but is considered a measurement of lower limb explosive power. 69,87 Psychosocial factors also appear important in the RTS decision-making process. 8,36,71,78 The biopsychosocial model for RTS decision making advocates a multidisciplinary approach, with regular assessments of functional tests, health, well-being, and motivation and frequent review of goals in the athletic population. 7
However, RTS criteria after shoulder stabilization remain elusive. In a recent systematic review by Ciccotti et al, 26 75% of studies used time from surgery as the sole criterion to dictate RTS after anterior shoulder stabilization. 26 Selecting appropriate outcome measures is a critical step in RTS decision making.
The primary aim of the current study was to describe the use of quantifiable objective outcome measures and PRO tools after surgical glenohumeral joint stabilization, specifically in an athletic population. The secondary aim of our study was to assess whether the method of measurement used was clearly described and standardized to aid clinical interpretation.
Methods
Protocol and Registration
This systematic review was registered (42017064094) with Prospero (Centre for Reviews and Dissemination), University of York, on April 5, 2017. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement was used.
Search Strategy
An electronic database search of MEDLINE, Scopus, SPORTDiscus, and Web of Science was conducted by 2 authors (E.F. and N.M.), from inception to December 2018, using multiple keywords and Boolean phrases (Table 1). The database searches were accompanied by searches of the reference lists of the included articles, and ongoing trials were searched on the WHO International Clinical Trials Registry Platform and ClinicalTrials.gov.
Search Terms Used for All 4 Databases a

a An asterisk indicates truncation (any words starting with this string of characters) (eg, athl* will get athlete, athletes, athletic, etc).
Study Selection
Included studies had to meet the following criteria: participants must have been recruited from an athletic population, they must have undergone a surgical procedure for glenohumeral joint instability, and the outcome of surgery must have been assessed by a quantifiable objective outcome measure and/or a PRO measure. As recommended by Araújo and Scharhag, 5 we used 4 criteria to define the term athlete: a person (1) training in sports aiming to improve his or her performance; (2) actively participating in sport competitions; (3) formally registered in a local, regional, or national sport federation as a competitor; and (4) having sport training and competition as his or her major activity or focus of interest. We chose a broad definition of “glenohumeral joint instability” because the intent of the review was to describe the outcome measures used after shoulder stabilization rather than to study surgical interventions. Glenohumeral joint stabilization was inclusive of arthroscopic Bankart repair, arthroscopic reverse Bankart repair, arthroscopic Latarjet procedure, remplissage procedure, open Bankart repair, open Latarjet procedure, and superior labral anterior-posterior repair. Patients who had ancillary procedures such as biceps tenotomy, bicep tenodesis, and rotator cuff repair or acromioclavicular stabilization performed at the time of stabilization were excluded. Patients younger than 13 years were excluded, because children with open physes may present with different pathoanatomy after a dislocation. 29 Studies with level 5 evidence as per Oxford Centre for Evidence-Based Medicine 2011 level of evidence criteria 51 and studies not published in English were also excluded.
Potentially eligible papers were independently screened by 2 of the authors (E.F. and N.M.). Disagreements between reviewers were resolved in a consensus meeting. If consensus was not reached, another author (E.C.F.) was consulted to reach a decision.
Data Extraction
Two authors (E.F. and N.M.) used predefined data fields to extract data independently and then crossed-checked their databases for accuracy. We included data on patient characteristics, type of surgical intervention, patient’s athletic status, type of sport participation, and hours of sport participation per week. For the purpose of this study, athletes were classified as playing at a competitive level if they actively competed in competition and/or were registered in a local, regional, or national federation.
Outcome Data Extracted
Quantifiable Objective Clinical Outcomes
We appraised studies for the use of a standardized method of measuring objective clinical outcomes.
Range of Motion (ROM)
We considered studies to have used a standardized method of measuring ROM if the authors documented the measuring tool used, planes of motion measured, and position of the participant during testing. If ROM was recorded as part of a quantitative shoulder outcome score and the authors provided information on how they recorded this outcome (eg, Constant-Murley score), this was also documented.
Muscle Strength
Strength outcome measures were similarly assessed. We considered studies to have used a standardized method of measuring strength if the authors documented the plane in which they measured strength, the measuring tool used, and position of the participant during testing. If strength was recorded as part of a quantitative shoulder outcome score and the authors provided information on how they recorded this outcome (eg, Constant-Murley Score), this was also documented.
Other Quantifiable Objective Clinical Outcomes
We also assessed electromyography (EMG), kinetics and kinematics data capture, and shoulder proprioception for a standardized method of measurement.
Other Clinical Outcomes
We recorded the results of objective tests for assessing shoulder instability, shoulder joint laxity, and muscle integrity. Patient satisfaction outcome was recorded, including the simple single question of satisfaction and any validated measure of patient satisfaction. If patient satisfaction was recorded as part of a quantitative shoulder outcome score (eg, American Shoulder and Elbow Surgeons score), this was not separately documented in this category. We also recorded radiological assessment.
Return to Sport
Mean time to RTS was recorded. For the purpose of this review, RTS was the point at which the athlete returned to his or her sport, at any level (not taking into account level of participation). 7 Both RTS and return to play were treated as equivalent terms.
Patient-Reported Outcomes
PROs refer to ratings and reports about the health status of a patient and are based on data provided by a patient or by a person who can report on the patient’s behalf, without amendment or interpretation by a clinician. 112 We reported all PRO tools used to assess postoperative outcomes, whether clinician derived or patient derived. If different variations of the PRO tool existed, we recorded the specific variation used by the investigator. For example, the Rowe score, a scoring system for the postoperative assessment of Bankart repairs, has 4 different versions. 55
We also noted whether the PRO measure was generic (measuring aspects of health status and quality of life that are common to most patients: eg, 36-item Short Form Health Survey), disease specific (for a specific type of shoulder problem: eg, Western Ontario Shoulder Instability), or sport specific (eg, Athletic Shoulder Outcome Scoring System), or whether it evaluated psychosocial factors (eg, Injury Psychological Readiness to Return to Sport). 114
Data Synthesis
The results were summarized in a tabular fashion; we completed a qualitative analysis only. Poor study quality and the associated high risk of bias precluded a meta-analysis of the articles in this review. 50
Assessment of Risk of Bias and Level of Evidence
We used a simplified version of the Downs and Black checklist as proposed by Trac et al 108 to assess study quality (see Appendix 1, available as supplemental material). Subscales in this tool include reporting, external validity, internal validity, selection bias, and power. Trac et al changed the scoring of question 27 from 5 points to 1 point, such that the 27 questions have a total score of 28. 32,108 Two authors (E.F. and N.M.) independently appraised and then cross-checked studies for agreement. If consensus was not reached, another author (E.C.F.) was consulted to reach a decision. The level of evidence was assessed using the Oxford Centre for Evidence-Based Medicine 2011 level of evidence criteria and was rated by 2 authors (E.F. and N.M.). 51
Results
Literature Selection
The online search of the 4 databases yielded a total of 2557 articles. After exclusion of duplicates, 1709 abstracts were assessed for eligibility. Full-text articles were obtained for 445 studies. An initial 347 articles were identified from the online database search according to the inclusion and exclusion criteria, and an additional 98 publications were identified through secondary screening measures (reference and citation searches and manual searches of a high impact factor orthopaedic journal). Of the 445 studies, we excluded 383 for the following reasons: 229 studies included participants who were not athletes, 94 studies were excluded due to their design, 28 studies did not use a quantitative outcome measure and/or PRO measure, 18 studies entailed a population that did not undergo surgical glenohumeral stabilization, 8 studies were not published in the English language, 3 studies entailed an intervention carried out on cadavers, and 3 studies were commentary reviews in books. This review therefore covers a total of 62 articles. The search results, according to PRISMA guidelines are shown in Figure 1.

Literature selection algorithm using PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) guidelines.
The quality of the studies included was variable. Quality appraisal scores (modified Downs and Black checklist 108 ) ranged from 4 to 25 out of a possible 28 points, with an average score of 13.5. Appendix 2 (available as supplemental material) presents a review of the methodological quality and risk for bias assessment of the 62 studies. Table 2 is a summary of the level of evidence of the included studies.
Level of Evidence

Patient Characteristics
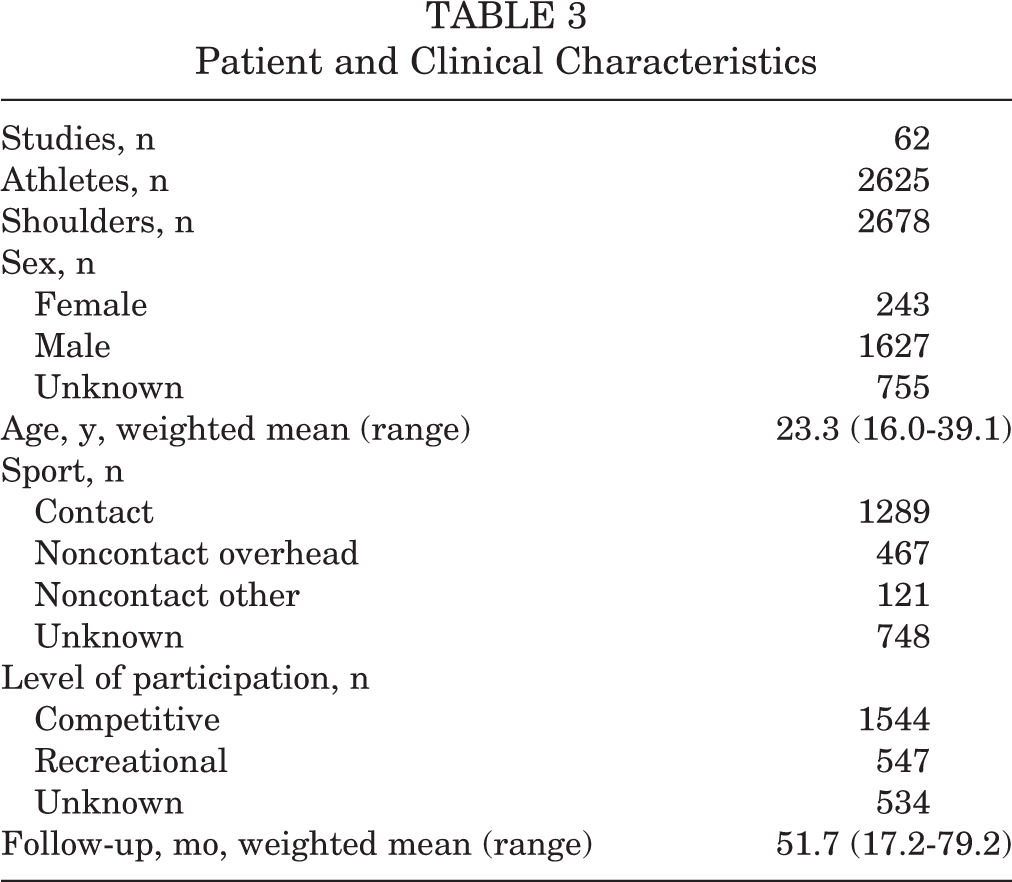
Patient characteristics are shown in Appendix 3 (available as supplemental material) and summarized in Table 3.
Patient and Clinical Characteristics
Quantifiable Clinical Objective Outcome Measures
A total of 58 (94%) studies used some form of quantifiable objective clinical outcome to measure the effectiveness of surgical intervention. Only 11 (18%) studies ¶ described a standardized method of measuring the outcome. Of these, 7 studies 12,17,18,22,31,60,72 measured ROM and/or muscle strength, 2 studies 38,110 measured shoulder proprioception, and 2 studies 24,65 collected data with a 3-dimensional motion analysis system reporting on the biomechanics of shoulder and body during throwing. Further, 3 studies 24,38,72 described a standardized method of measuring surface EMG muscle activity. The remaining 47 of the 58 studies did not quantify how they measured the objective outcomes used. Quantifiable outcome measures and other clinical outcome measures are summarized in Appendix 4 (available as supplemental material).
Range of Motion
A total of 53 (85%) studies included ROM as an outcome; however, only 6 (10%) studies 12,17,18,31,60,72 described a standardized method of measuring ROM. We found that 4 studies 12,17,18,60 measured ROM as part of the Constant-Murley score, detailing plane of measurement, measurement tool, and position of participant during testing. Meller et al 72 measured ROM according to the principles of the American Shoulder and Elbow Surgeons. Douoguih et al 31 also detailed plane of measurement, measurement tool, and position of participant during testing. In the remaining 47 of the 53 studies, it was not possible to identify the measurement tool and/or the position in which the participant was tested.
Of the 53 studies that included ROM as an outcome, 43 recorded external rotation range in neutral and/or 90°, 32 studies measured flexion range, 28 studies measured internal rotation in neutral and/or 90°, and 21 studies measured abduction range. Eight of the 53 studies failed to report the plane in which ROM was measured.
Muscle Strength
Muscle strength testing was recorded in 13 (21%) studies, with 5 (8%) studies 12,17,18,60,72 demonstrating a standardized method of measurement. Of these, 4 studies 12,17,18,60 measured muscle strength as part of the Constant-Murley score, detailing plane of measurement, measurement tool, and position of participant during testing. Meller et al 72 measured isokinetic strength in the Biodex chair at velocities of 60, 120, and 180 deg/s. Flexion and extension were tested in the sagittal plane, abduction and adduction were tested in the plane of the scapula, and rotation was tested in the transverse plane with the arm abducted 15°.
We noted that 4 studies 17,18,39,72 used a handheld dynamometer, 2 studies 72,77 used an isokinetic dynamometer, and 2 studies 12,60 used a spring balance device to record strength. A further 2 studies 61,97 measured strength manually, and the remaining 3 studies 22,68,113 did not report the tool used to measure strength.
Other Quantifiable Objective Clinical Outcomes
Overall, 5 (8%) studies 24,38,65,72,110 described a standardized method of collecting another type of quantifiable objective outcome, aside from ROM and muscle strength. Of these, 2 studies 24,65 collected data with a 3-dimensional motion analysis system while participants threw fastballs, reporting on the biomechanics of shoulder and body during throwing. A further 3 studies 24,38,72 incorporated the measurement of surface EMG muscle activity in their studies. Chalmers et al 24 measured muscle activity during pitching. Fremerey et al 38 measured muscle activity with the arm held in neutral, 90° of abduction with an extended elbow joint and during maximal isometric abduction, external rotation, and flexion, all at 90°. Meller et al 72 collected EMG muscle activity simultaneously to record isokinetic strength. Further, 2 studies 38,110 examined shoulder joint proprioception after surgery: Fremerey et al assessed joint position sense using the passive angle reproduction test, whereas Uhring et al 110 assessed shoulder proprioception as the ability to reproduce an angle in flexion or abduction (55°, 90°, 125°) using a laser pointer on a wall-mounted target.
Other Clinical Outcomes
Clinical Tests
A total of 24 (39%) studies used clinical examination tests as an outcome measurement. Of these, 17 studies # recorded objective instability (anterior apprehension and relocation test and/or posterior subluxation test), 7 studies 12 –14,42,53,89,109 reported shoulder joint laxity (anterior and posterior drawer tests or sulcus test), and 2 studies 95,99 used special tests for assessing shoulder muscle integrity (liftoff and belly press test).
Radiological Findings
A total of 17 (27%) studies ** incorporated radiological findings as an outcome measure. The modalities they used included radiography, computed tomography, and magnetic resonance imaging.
Patient Satisfaction
We noted that 7 (11%) studies 68,74,76,90,93,102,113 collected information on patient satisfaction. The majority of these studies reported an overall percentage of patient satisfaction.
Time to Return to Sport
Mean time to RTS (Table 4) was reported for 472 athletes in 12 studies. ††
Mean Time to Return to Sport (RTS)

Patient-Reported Outcomes
In total, 59 (95%) studies used at least 1 PRO measure: 19 studies used a single PRO tool, 25 studies used 2 PRO tools, 7 studies used 3 PRO tools, and 8 studies used 4 or more PRO tools. The various PRO measures used are represented in Appendix 5 (available as supplemental material) and summarized in Table 5.
Patient-Reported Outcome Measures Used in the Included Studies

The Rowe score was used most frequently in the studies we reviewed. We found that 22 studies ‡‡ contained the 3 items of stability, motion, and function; 6 studies 56,74,77,79,95,100 used the 4 items of function, stability, pain, and motion; 3 studies 13,16,15 recorded pain, motion, stability, function, and strength; and 1 study 91 included stability, motion, and function. Further, 7 studies 6,25,46,63,64,75,90 provided no information about the version of Rowe score they used.
A total of 7 (11%) studies 18,24,39,42,70,76,101 used a generic health questionnaire in combination with a disease-specific PRO tool, whereas 22 (35%) studies §§ used a visual analog scale to assess pain in combination with a disease-specific and/or generic health questionnaire. Further, 8 (13%) studies 15,22,37,42,72,73,85,86 recorded the results of a sport-specific questionnaire in combination with a disease-specific and/or generic health questionnaire. No studies included in our review used a PRO tool to assess psychosocial factors.
Baseline Reporting of Outcome Measures
More than half of the studies (32/62) ∥ ∥ recorded baselines scores of PROs before surgical intervention.
Discussion
Our systematic review of the literature investigating the use of outcome measures after shoulder stabilization in athletes found that most studies used a quantifiable objective measure. However, measurement tools used and method of collecting outcome measures were often poorly described and not standardized. We also noted that few studies attempted to assess an athlete’s ability to meet the demands that RTS would place on the shoulder. Nearly all studies included the use of at least 1 PRO measurement; however, there was substantial variability in the use of PROs in this population, making it difficult to compare study outcomes. Even when studies used the same PRO, some of the individual components used varied, again limiting comparability.
Standardization and the Clinical Application of Quantifiable Outcome Measures
Our review revealed that only 18% of the studies investigating outcome measures of surgical intervention for shoulder instability in athletes entailed a comprehensive method for quantifying the outcome measurement. Furthermore, only 10% of the studies described a standardized method of measurement for the most commonly used objective outcome measure, ROM. Evidence suggests that reduced ROM is a predictive factor for shoulder injury in healthy throwing athletes. 27,94,116 A reliability study showed high inter- and intratester reliability for a variety of test positions for measuring glenohumeral joint rotation. 28 This is possibly an important area to clarify and suggests that future investigators should describe a method of measurement that is standardized. This should allow for comparison of studies and synthesis of normative ROM data for RTS.
Research has also shown evidence of a relationship between shoulder injury and muscle strength deficits in some sports 27,33,103 ; however, only 24% of the included studies in this review used muscle strength as an outcome measure, with 8% of the studies using a standardized method of measuring muscle strength. A more robust, quantifiable method of measuring strength will allow for better interpretation of the literature. We propose that when measuring ROM and strength, authors describe the plane in which they measured motion or strength, the measuring tool used, and the position of the participant during testing.
Only 2 studies investigated the effect of surgery on shoulder joint proprioception, despite research showing that proprioception is altered in people with shoulder pathology. 3,119 If shoulder proprioception is impaired, it may not be possible for a person to engage appropriate muscles to stabilize the shoulder during functional and sporting activities, potentially leaving the shoulder more susceptible to injury. 1,40 In addition, studies have identified the negative impact of fatigue on shoulder joint position during sports activity. Perhaps testing shoulder joint position sense in a fatigued state may be beneficial to ensure that athletes are not prematurely cleared for return to play. 49 However, we acknowledge that assessment of joint proprioception is likely to be poorly used due to the challenge of quantifying proprioceptive impairments in a joint as mobile as the shoulder.
Suitability of Quantifiable Outcome Measures for an Athletic Population
Ideally, outcome measures selected for an athletic population should assess athletic performance and identify athletes potentially at risk of reinjury after surgery. Our review highlighted that ROM and muscle strength (isometric or isokinetic peak torque) are the most frequently captured quantifiable outcome measures after surgical correction of shoulder instability in the athletic population. These are the same measures used in a nonathletic population and do not examine function or dynamic movement. Studies of lower limb injury have highlighted the role of strength, and particular components of strength (eg, rate of force development and explosive strength) have been identified as potential risk factors for reinjury. 4,62 Angelozzi et al 4 found that 6 months after anterior cruciate ligament (ACL) reconstruction, maximum voluntary isometric contraction levels had returned but decreased rate of force development persisted in the reconstructed limb. Knezevic et al 62 highlighted that at 6 months after ACL reconstruction, explosive strength of the involved quadriceps was 14% lower than the presurgery values despite maximum strength of quadriceps recovering to the presurgery level. Explosive strength (the ability to quickly exert a high level of muscle force) is often considered more important for maximizing movement performance than maximum strength 106 and is thought to be an important variable in stabilizing posture in response to mechanical perturbations. 35 In sports such as tennis, rugby, and basketball, the upper limb has to exert force quickly and withstand mechanical perturbations. Future studies investigating the influence of explosive strength and rate of force development (eg, plyometric push-ups, the Athletic Shoulder test 11 ) on RTS outcomes may be of interest.
The kinetic chain theory characterizes the body as a linked system of segments, often working in a proximal-to-distal manner. 34 Based on the proximal-to-distal concept, the quality of shoulder function depends on the function of the trunk and lower limb musculature. 84 Failure of the kinetic chain could lead to a decrease in glenohumeral joint stability and an associated increased risk of reinjury in athletes. Assessment of the kinetic chain in athletes may be warranted, particularly in ground-stance overhead athletes (eg, tennis, baseball); however, no study in our review attempted to assess the role of the kinetic chain in aiding successful RTS.
On-field functional performance tests are sometimes used in lower limb injury. For shoulder function, tests such as the seated medicine ball throw 111 and the upper quarter version of the Y-balance upper quarter test 104 have been described for evaluating throwing performance and weightbearing shoulder stability, respectively. Borms et al 20 demonstrated that isokinetic shoulder rotational strength moderately to strongly correlated with the seated medicine ball throw. However, they found no relationship between shoulder strength and the Y-balance upper quarter test, suggesting that this test may assess other variables within the kinetic chain (eg, thoracic mobility, core). 115 As far as we are aware, no published data are available examining the threshold of these tests that equates to prognosis of reinjury. 115 The closed kinetic chain upper extremity stability test (CKCUEST) is a performance test that provides a score for an upper extremity task in a closed kinetic chain position. 43 In a cohort of collegiate football players, Pontillo et al 80 found that players who scored less than the cutoff of 21 touches for the CKCUSET during preseason were more likely to be injured in-season. CKCUEST is the only functional upper quadrant test of which we are aware that has been shown to be predictive of shoulder injury and may be useful for clinicians to consider in reinjury prognosis and RTS after shoulder stabilization. However, we must bear in mind that the closed chain design of the CKCUEST may not provide specific information regarding the ability to perform open chain tasks such as throwing.
Variability in the Choice of Patient-Reported Outcome Measures Used
This systematic review identified 16 different PRO measures used in the literature to assess athletes’ perceptions of their improvement after surgery. The most prevalent PRO measure used by investigators is the Rowe score; however, 4 different versions of the Rowe score were used across this literature. Jensen et al 55 assessed the correlation and agreement of the various Rowe score versions and concluded that the 4 versions of the Rowe score can lead to significantly different results. This inevitably raises issues about data comparability and synthesis when different versions are used. Our study highlighted that the majority of PRO measures used were disease specific, with 95% of the included studies using at least 1 disease-specific questionnaire. Only 13% of studies used a sport-specific questionnaire to measure the ability of athletes to resume their preinjury sporting activity. Athletes are different from the general population and have higher levels of physical function. Disease-specific and generic health questionnaires may, at best, not detect sport-specific impairments; at worst, such questionnaires may underestimate sport or activity-specific deficits, which might predispose the athlete to reinjury. 98
Ardern et al 9 showed that preoperative psychological responses were associated with the likelihood of successful return to preinjury level at 12 months after ACLR. Olds et al 78 demonstrated that psychosocial factors and fear of reinjury are associated with risk of recurrent shoulder instability after a first-time traumatic shoulder dislocation. However, no study included in our review specifically evaluated an athlete’s psychological responses to the initial injury, to surgery, and to the recovery journey. The Anterior Cruciate Ligament-Return to Sport Index has been shown to be a useful prognostic tool for RTS after an ACL injury. 10 Gerometta et al 41 showed that a similar scale, the Shoulder Instability Return to Sport after Injury (SIRSI), is a valid and reliable scale to help identify athletes’ psychological readiness to RTS after traumatic anterior shoulder dislocation. Studies incorporating use of the SIRSI scale, alongside other psychological factors shown to positively correlate with RTS in the lower limb 8,96 (motivation, self-confidence, and slight fear), are warranted in this cohort.
We recommend that clinicians and surgeons use a disease-specific questionnaire such as the Western Ontario Shoulder Instability Index or the Oxford Shoulder Instability Questionnaire alongside a questionnaire (eg, SIRSI) that assesses an athlete’s psychological readiness to RTS, which is not detectable by established clinical scores.
Limitations
This systematic review has limitations. We chose a broad definition of glenohumeral joint instability to ensure that all relevant outcome measures used after shoulder stabilization were captured. However, the wide variety of conditions included was, in turn, a likely factor in the heterogeneity of outcome measures used and their application. Despite our attempt to extract data specific to subgroups of athletes, outcome measures were often not reported in uniform cohorts, and therefore it was not possible to extract specific outcome measures used for subsets of athletes (eg, contact athletes, throwing athletes). The studies included in this review were generally low in methodological quality based on the Downs and Black checklist. Only 14% of the included studies were conducted prospectively, and the majority of the studies assessed surgical management of shoulder instability in athletes retrospectively. Conducting more sufficiently powered prospective investigations should decrease bias in the outcome measures used, subsequently allowing for more accurate comparisons of clinical studies.
Conclusion
This review identified that the majority of the included studies used a quantifiable clinical outcome measure and a PRO tool. However, failure to clearly describe a standardized method of measurement of objective outcomes hindered study comparison and clinical interpretation. The finding that the method used for outcome assessment was not standardized for a large percentage of studies suggests a means of improving the quality of future literature describing the assessment of shoulder instability. Shoulder joint proprioception and the kinetic chain are areas of interest after glenohumeral joint stabilization, but they were poorly assessed in the papers we reviewed. Sport-specific functional tests and psychosocial factors were not explored in the studies included in our review. A concerted effort should be made to standardize the use of PRO tools so readers can synthesize the literature in a meaningful way, both for clinical use and subsequent research. Finally, authors should describe the sport (eg, collision sport) and level of participation (eg, recreational or competitive) to facilitate comparison across studies.
Supplemental Material
Supplemental Material, DS_10.1177_2325967120950040 - Outcome Measures After Shoulder Stabilization in the Athletic Population: A Systematic Review of Clinical and Patient-Reported Metrics
Supplemental Material, DS_10.1177_2325967120950040 for Outcome Measures After Shoulder Stabilization in the Athletic Population: A Systematic Review of Clinical and Patient-Reported Metrics by Edel Fanning, Natasha Maher, Ann Cools and Eanna C. Falvey in Orthopaedic Journal of Sports Medicine
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.