
Abstract
Background:
Tibial rotation is an important topic in anterior cruciate ligament (ACL) surgery, and many efforts are being made to address rotational stability. The exact role of the ACL in controlling tibial rotation in clinical studies is unknown.
Purpose:
To quantify the effect of ACL reconstruction on the amount of tibial rotation based on the current available literature.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A literature search of the PubMed and EMBASE databases was performed in August 2019. Two independent reviewers reviewed titles and abstracts as well as full-text articles. A total of 2383 studies were screened for eligibility. After screening of titles and abstracts, 178 articles remained for full-text assessment. Ultimately, 13 studies were included for analysis. A quality assessment was performed by means of the RoB 2.0 (revised tool for Risk of Bias in randomized trials) and the ROBINS-I (Risk Of Bias In Non-randomized Studies–of Interventions) tools.
Results:
According to the studies using computer-assisted surgery that were included in this review, ACL reconstruction resulted in an average reduction in tibial rotation of 17% to 32% compared with preoperatively; whether the range of tibial rotation returned to preinjury levels remained unclear. In the current literature, a gold standard for measuring tibial rotation is lacking. Major differences between the study protocols were found. Several techniques for measuring tibial rotation were used, each with its own limitations. Most studies lacked proper description of accompanying injuries.
Conclusion:
ACL reconstruction reduced the range of tibial rotation by 17% to 32%. Normal values for the range of tibial rotation in patients with ACL deficiency and those who undergo ACL reconstruction could not be provided based on the current available literature owing to a lack of uniform measuring techniques and protocols. Therefore, we advocate uniformity in measuring tibial rotation.
Rupture of the anterior cruciate ligament (ACL) is a common sports injury, often leading to prolonged absence or even cessation of sports activities. Next to its primary role in restraining anterior tibial translation, the ACL is an important factor in the rotational stability of the knee. 4,7 Although current practice supports ACL reconstruction (ACLR) as an important factor in returning to sports activities, and good results after transtibial ACLR are generally achieved, 1,5 a large group of patients still report residual laxity in the form of “giving way” and/or a positive pivot shift. 1 To address this phenomenon, the double-bundle reconstruction technique and the “anatomic” reconstruction technique have been developed. Both techniques show better control in vitro of rotational laxity. 28,30 In recent years, accessory extra-articular stabilizing techniques (eg, anterolateral ligament reconstruction, Lemaire procedure) have been reintroduced to better control rotational laxity. However, a scientific basis to support this trend is lacking.
In vivo, the available studies use only subjective tests to measure the amount of postoperative rotational laxity (eg, pivot shift test). Because no generally accepted gold standard for measuring tibial rotation exists, comparing outcomes between studies is not possible. The conclusions and outcomes on the amount and direction of tibial rotation in ACL deficiency and after ACLR are contradictory. As well, increased internal rotation and increased external rotation have been reported. This leads to inconclusive results. We aimed to set the first step in developing a standard, valid, and reproducible protocol for measuring tibial rotation.
The purpose of this systematic review was to assess the influence of the reconstructed ACL on objectively measured tibial rotation. Two research questions were formulated:
Does range of tibial rotation increase after rupture of the ACL?
Does ACLR lead to decreased range of tibial rotation?
Methods
In August 2019, a literature search was performed in the PubMed database using the following search terms: (anterior cruciate ligament[tiab] OR ACL[tiab] OR “Anterior Cruciate Ligament”[Mesh]) AND (“Rotation”[Mesh] OR rotat*[tiab]) AND (“Tibia”[Mesh] OR tibia[tiab] OR tibial[tiab] OR knee[tiab]) NOT (animal NOT human).
Next, the Embase database was searched using (‘tibia’/exp OR tibia: ab, ti OR tibial: ab, ti OR knee: ab, ti) AND (‘rotation’/exp OR rotat*: ab, ti) AND (‘anterior cruciate ligament’/exp OR ‘anterior cruciate ligament’: ab, ti OR acl: ab, ti NOT (animal NOT human). Duplicates were removed through use of RefWorks. Titles and abstracts were screened to match the inclusion criteria. Exclusion criteria were as follows:
Pivot-shift test without quantification of rotational instability
Newly developed devices to measure tibial rotation, without any form of reference
Any descriptions other than internal or external rotation in degrees
Patients included with concomitant injury to the anterolateral structures
Studies using cadavers
Studies using motion capture systems or in vivo tracking systems
Studies without English or Dutch full text available
Following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, 2 independent reviewers (M.J.M.Z., B.J.R.) assessed titles, abstracts, and full-text articles. In case of debate on inclusion of an article, a third independent reviewer (R.L.D.) was consulted. Next, a quality assessment was performed, in which the same 2 reviewers independently assessed the methodological quality of all of the selected studies. For nonrandomized trials, the 7-item ROBINS-I (Risk Of Bias In Non-randomized Studies–of Interventions) tool was used. 29 To assess the quality of the included randomized trials, the 5-item RoB 2.0 (revised tool for Risk of Bias in randomized trials) tool was used. 17 Both tools are recommended by the Cochrane Scientific Committee to be used in systematic reviews.
Results
A total of 2383 studies were screened for eligibility. After screening of titles and abstracts, 222 studies remained for full-text assessment. We found that 44 articles had no English full text available or were abstract-only reports of scientific presentations. After reading the remaining 178 full text articles, another 165 articles were excluded based on the criteria listed above. Ultimately, 4 studies describing patients with ACL deficiency and 9 studies describing tibial rotation in patients with ACLR were included for analysis (Figure 1). All included full-text articles were explored for the amount of tibial rotation measured. If applicable, internal and external tibial rotation were noted separately. An overview of reported values of tibial rotation is provided in Tables 1 and 2.

Flow diagram detailing the results of the literature search using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. ACL, anterior cruciate ligament.
Range of Tibial Rotation During Testing at Fixed Flexion Angle a

a Values for rotation are reported in degrees as mean or as mean ± SD. ACL, anterior cruciate ligament; adolesc, adolescent; AMP, anteromedial; CAS, computer-assisted surgery; CT, computed tomography; DB, double bundle; def, deficient; F, female; int, intact; M, male; MRI, magnetic resonance imaging; NA, not applicable; NR, not reported; recon, reconstruction; SB, single bundle; TT, transtibial.
Range of Tibial Rotation During Dynamic Testing in Patients With ACL Deficiency a

a Values for tibial rotation are reported in degrees as mean ± SD. ACL, anterior cruciate ligament; def, deficient; int, intact; MRI, magnetic resonance imaging.
Patients With ACL Deficiency
There were 4 studies on patients with ACL deficiency (Table 3). 6,13,15,23 In 2 studies, 6,15 magnetic resonance imaging (MRI) was used to evaluate tibial rotation. Haughom et al 15 applied a compressive force of 44-N axial load and 3.35-N internal and external rotational torque and reported a significant difference between patients with ACL deficiency and those with intact ACL. As well, a significant difference between ACL-deficient knees and the contralateral intact knees was reported. Barrance et al, 6 when studying unloaded knees, did not demonstrate a significant difference in rotation between patients with intact ACL and patients with ACL deficiency.
Characteristics of Studies on ACL Deficiency a

a 3D, 3-dimensional; ACL, anterior cruciate ligament; ACLD, ACL deficiency; CAS, computer-assisted surgery; CLI, contralateral intact; CT, computed tomography; MRI, magnetic resonance imaging; NA, not applicable.
Using 3-dimensional (3D) computed tomography (CT) and biplanar fluoroscopy, Miyaji et al 23 studied tibial rotation in patients performing a wide-based squat. No significant difference was shown between ACL-deficient knees and contralateral intact knees in terms of range of tibial rotation. Grassi et al 13 used computer-assisted surgery (CAS) to evaluate knee kinematics in patients with ACL deficiency. Grassi et al tried to link the kinematic pattern, acquired by CAS, to bony morphologic status, which was evaluated by MRI. Those investigators reported an indirect correlation between the lateral posterior tibial slope and rotational laxity.
Patients After ACLR
We retrieved 9 studies 9 –12,16,18,20,22,26 in which ACL-reconstructed knees were analyzed for the range of tibial rotation. In 6 ACLR studies, 9 –12,20,22 a CAS system was used during surgery to perform pre- and postoperative measurements. The other 3 studies 16,18,26 were classified as “other evaluation method” (Tables 4 and 5).
Characteristics of Studies on ACL Reconstruction Evaluated by CAS a

a ACL, anterior cruciate ligament; ACLD, ACL deficient; ACLR, ACL reconstruction; AMP, anteromedial portal; CAS, computer-assisted surgery; DB, double bundle; RCT, randomized controlled trial; SB, single bundle; TT, transtibial.
Characteristics of Studies on ACL Reconstruction Evaluated by Other Methods a

a 2D, 2-dimensional; 3D, 3-dimensional; ACL, anterior cruciate ligament; CT, computed tomography; DB, double bundle; MRI, magnetic resonance imaging; SB, single bundle.
b No data available on DB reconstruction group.
c Same patient pre- and postoperative.
Computer-Assisted Surgery
In 6 studies, CAS software was used to measure range of tibial rotation before and after ACLR. 9 –12,20,22 In all of these studies, a manual force was applied in order to rotate the tibia. Maximum internal and external rotations were applied to the foot of the anesthetized patient, and associated values of maximum internal and external rotation of the knee were recorded. All studies showed a reduction in total range of tibial rotation of between 17% and 32% after ACLR (Tables 1 and 2). We identified 2 studies that compared single-bundle reconstruction with double-bundle reconstruction. 11,20 Debieux et al 11 detected no significant difference regarding range of tibial rotation between the 2 techniques. Lee 20 found less total rotation at 30° and 60° of flexion after double-bundle reconstruction compared with single-bundle reconstruction. Apart from the fact that the amount of the applied force rotation was not recorded, all of these studies using CAS were graded to have a moderate to severe risk of bias in selection of patients and/or confounding (Figures 2 and 3).
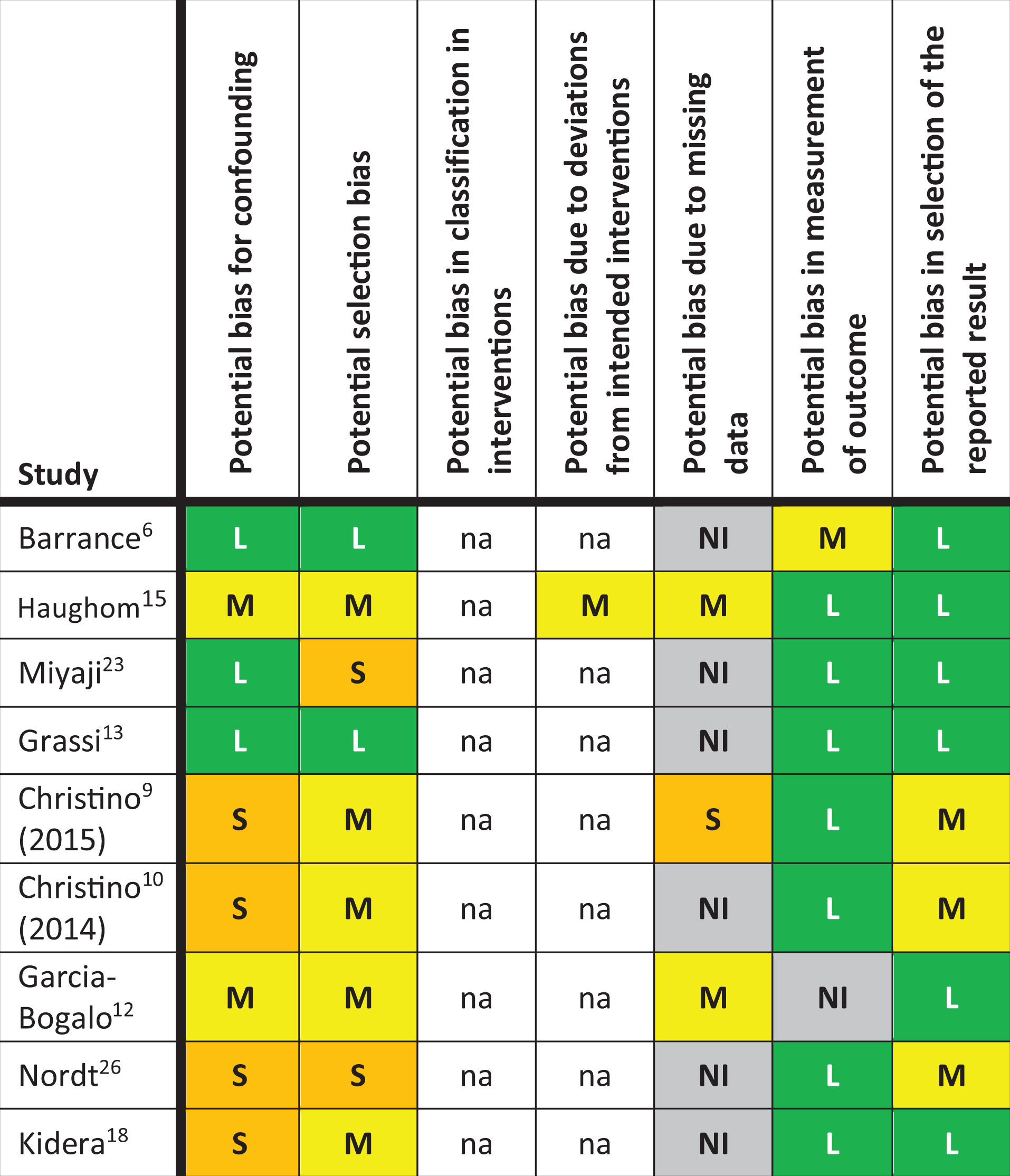
Analysis according to the ROBINS-I (Risk Of Bias In Non-randomized Studies–of Interventions) tool for potential bias in the included nonrandomized trials. L, low risk of bias; M, moderate risk of bias; na, not applicable; NI, no information; S, serious risk of bias.
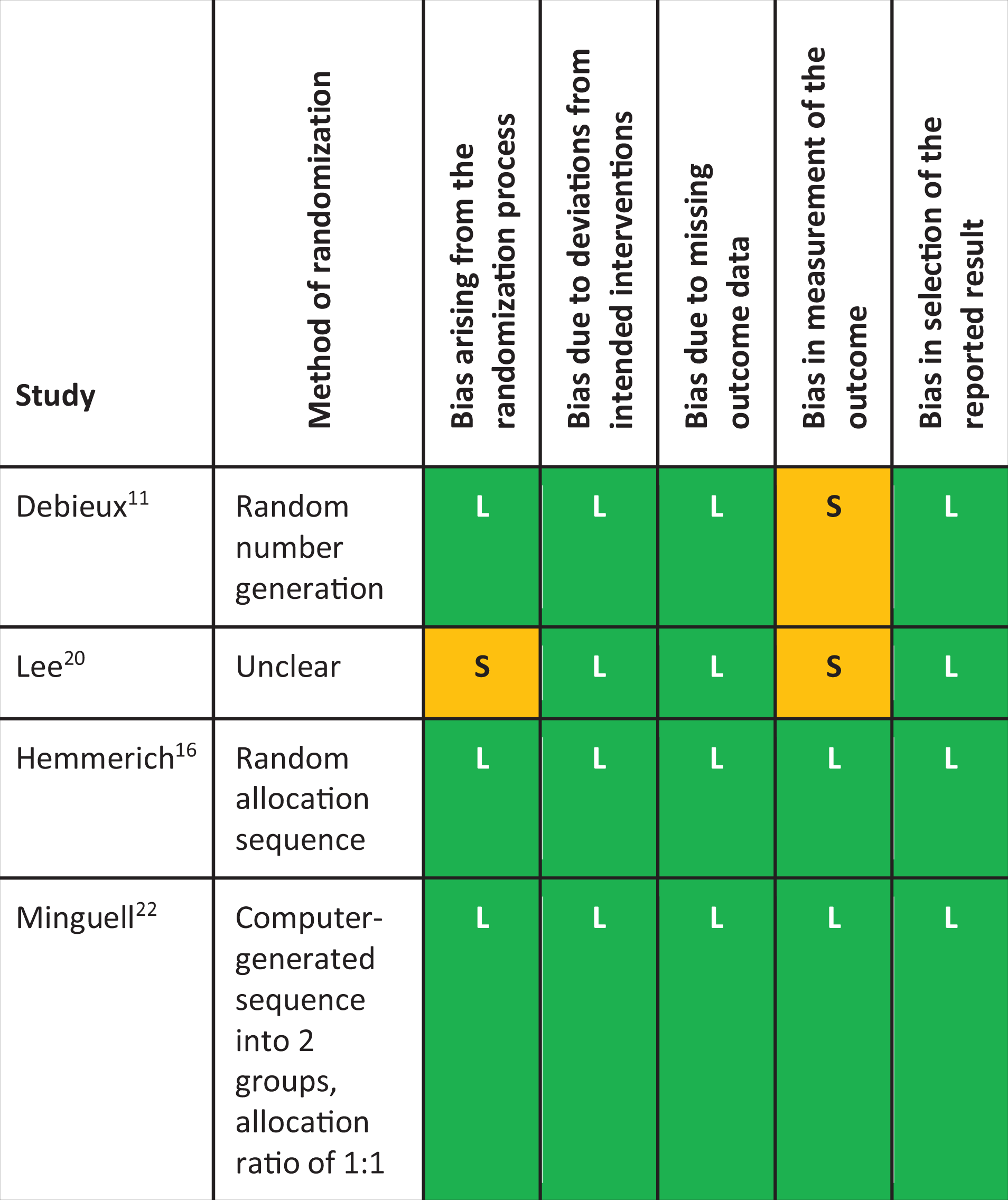
Quality assessment according to the RoB 2.0 (revised tool for Risk of Bias in randomized trials) tool of the included randomized controlled trials. L, low risk of bias; S, serious risk of bias.
Minguell et al 22 performed the only study that randomized between an anteromedial portal technique (AMP) and a transtibial drilling technique (TT) to create the femoral tunnel. The AMP group showed a more anatomic positioning of the graft in both sagittal and coronal planes. Preoperatively, no difference in range of tibial rotation was seen between the groups. Postoperatively, the AMP group showed a significant difference regarding the improvement of absolute values of internal rotation (AMP, 4.9°; TT, 3.8°; P = .016). However, in terms of range of tibial rotation, no difference was observed. Both techniques reduced the amount of total tibial rotation by 19% 22 (Tables 1 and 2).
Other Measuring Methods
We retrieved 3 more studies that examined tibial rotation after ACLR. 16,18,26 Hemmerich et al 16 used MRI to evaluate tibial rotation, whereas Nordt et al 26 used CT scans. Both applied a 5-N·m torque. Kidera et al 18 acquired 3D CT and biplanar fluoroscopy while patients were in a squatting position to evaluate tibial rotation after double-bundle ACLR. This is the same technique as used by Miyaji et al 23 to study patients who had ACL deficiency. A decrease in range of tibial rotation of 13.5% after ACLR was shown by Kidera et al, although this did not reach statistical significance. In that study, no significant difference between the injured and contralateral intact leg was reported (14.9° and 14.5°, respectively). The studies by Nordt et al and Kidera et al were graded as having a serious risk of selection and confounding bias (Figure 2).
Overall Rating of Quality of Evidence
The majority of included studies were observational studies. Only 4 randomized controlled trials were included. According to the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) classification, 14 the overall quality was rated as low to very low, based on inconsistencies, imprecisions, and risk of bias. The evidence statements according to the GRADE classification were as follows: Very low evidence for ACL rupture leading to an increase in range of tibial rotation, and low evidence for ACLR leading to a decrease in range of tibial rotation in relation to the injured state. An overview of the quality assessments of the included trials is provided in Figures 2 and 3.
Discussion
The studies regarding patients with ACL deficiency differed too much in study protocols to compare results in a proper manner. Therefore, no general conclusion could be drawn on the amount of range of tibial rotation in patients with ACL deficiency.
According to the studies reviewed, ACLR resulted in an average reduction of 17% to 32% of tibial rotation when pre- and postoperative states were compared. This finding seems to be consistent over different flexion angles. A study comparing the postoperative state with a preinjury state is yet to be designed, so whether the ACL returns to preinjury levels remains unclear.
Studies using the pivot-shift test without an objective, external measurement technique for rotational measurement were excluded. Previous work by Musahl et al 24 showed a wide variation in pivot-shift technique as well as clinical grading between examiners. Therefore, the use of pivot shift as a sole measurement technique was regarded as too subjective.
Several techniques for measuring tibial rotation have been used: MRI, biplanar fluoroscopy, CAS, motion capture systems, and several newly developed devices. For the purpose of this review, studies using motion capture systems were excluded. The numerous possibilities in cutting maneuvers made comparison between studies very difficult. Newly developed devices to measure tibial rotation were excluded when no reference method (eg, CAS) was used as a comparison. A remarkable outlier was the study performed by Hemmerich et al 16 (see Table 1). Hemmerich et al used MRI scans before and after ACLR to compare the range of tibial rotation. Reported values were out of range when compared with the results of the other studies reported in Table 1. Most likely this is the result of the different measuring technique. Because the Hemmerich et al investigation was the only study using the MRI technique in subjects after ACLR, we cannot validate the outcome.
Each measuring method has its own limitations. 21 When CAS is used, sensors are placed on the tibia and femur that can be detected by infrared cameras. Measuring intraoperative rotation during CAS has shown high reliability and is easily applied and very reproducible. Skin and soft tissue movements are eliminated, and pure bony movements are measured. Although there were differences between the patients studied (see Table 4), it can be concluded, based on the included studies, that in both single- and double-bundle ACLR, the range of tibial rotation after ACLR is diminished directly after the reconstruction.
A disadvantage of this technique is that CAS is used intraoperatively, which eliminates the influence of muscle tone, as in cadaveric research, and it is essentially performed in an unloaded situation. As a consequence, a reduced intraoperative range of tibial rotation cannot be related to the clinical situation. Because measuring with CAS instruments is an invasive procedure, preferably performed during surgery, it is difficult to reevaluate patients over time. Further, a comparison with the normal preinjury state is difficult. Using intraoperative measurements may also be incomparable to the clinical situation: First, after reconstruction, lengthening of the graft occurs after 2000 cycles of knee flexion-extension under moderate loading. 8 Due to creep of the ACL graft, lengthening of up to 20 mm has been reported, 8 which may lead to residual, or perhaps renewed, laxity. Second, when hamstring tendons have been harvested to be used as a graft, one of the active stabilizing structures counteracting external rotation of the tibia is weakened.
CAS, however, is a very accurate and reproducible tool to measure tibial rotation. Single-examiner reproducibility of rotatory laxity has been shown to be as low as 1.6°. 21 Although motion capture systems show promising results with respect to accuracy, 31 and skin motion artifact reduction tools have become more precise, 3 the current literature regarding the use of motion capture systems in ACLR is too diverse to advise on a standard protocol. MRI, CT, and biplanar fluoroscopy are of limited use in studying a dynamic situation such as tibial rotation.
Another issue is the difference in patient characteristics and the integrity of the other stabilizing structures around the knee joint. In clinical studies, Haughom et al 15 and Christino et al 10 reported a higher range of tibial rotation in female patients, which was not supported by Hemmerich et al. 16 Also, adolescents have been shown to have a higher range of tibial rotation compared with adults. 10
The menisci, the capsule, the anterolateral ligament, and the iliotibial band restrain the amount of internal rotation. 19 Concomitant injury to these structures may lead to an increased range of tibial rotation. None of the included studies reported whether any meniscal injury was present, even though the influence of an intact meniscus on stability is well known. 2,25,27
Study Limitations and Future Research
The range of tibial rotation in the context of ACL deficiency and reconstruction is a challenge that has not yet been resolved. Internal and external rotation can be measured only in relation to a neutral position, which can be challenging to determine, especially when repeated measurements are used over time. Moreover, the knee demonstrates an internal as well as an external rotational moment during movement. For that reason, we included in this review only articles reporting the total range of tibial rotation. Total range of tibial rotation is of key importance in relating excessive tibial rotation to clinical giving way, an increased internal rotation may not lead to increased laxity when external rotation is reduced.
All of the included studies lacked proper description of the included participants and previous history of the patients’ knees. We noted that 3 studies used randomization between single-bundle and double-bundle reconstruction. 11,16,20 None of these studies used a blinded observer. Due to the lack of uniformity in measuring techniques and study protocols, only descriptive statistics were provided in this review. Meta-analysis or even the providing of means or averages was not statistically justified.
This review focused on the role of the ACL in restraining rotational laxity. Other stabilizing structures (ie, iliotibial band, anterolateral ligament) were not taken into account. No further analysis was performed to evaluate the influence of the type of graft or surgical technique. Given the presence of many confounding variables, case matching may be critical in future research to isolate the influence of the ACL on tibial rotation.
Clinical Recommendations
We recommend that when CAS is used to evaluate tibial rotation, a uniform measuring protocol be followed. Based on findings in Tables 1 and 2, this protocol should contain measurements at 0°, 30°, and 60° of flexion and a maximum of 5 N·m of rotational force. With more than 60° of knee flexion, no further increase in range of tibial rotation is seen, and it would be of less clinical importance given that the stance phase in most activities will not include a knee flexed to more than 90°.
Conclusion
No gold standard is available for measuring tibial rotation in the current literature. Compared with the preoperative state, an ACLR seems to achieve a reduction of 17% to 32% of range of tibial rotation, as measured with CAS. Whether range of tibial rotation returns to preinjury levels remains unclear.
Based on the reviewed literature, the use of CAS in studying patients with ACL deficiency and those who undergo ACLR shows reproducible results. However, many varying protocols are being used. This review showed that when CAS is used, a maximum force of 5 N·m and flexion angles of 0°, 30°, and 60° are sufficient to detect relevant differences between the ACL-deficient and ACL-reconstructed state.
Normal values for the range of tibial rotation in patients with ACL deficiency and those who undergo ACLR could be provided based on the available literature owing to lack of uniform measuring techniques and protocols. We advocate uniformity in measuring tibial rotation, as described above. When future research is focused on a uniform research protocol, a meta-analysis might become within reach.
Footnotes
Acknowledgement
The authors thank Truus van Ittersum for her contribution in retrieving and organizing the search results.
Final revision submitted March 10, 2020; accepted April 3, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.G.Z. has received educational support from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.