
Abstract
Cyclops lesion is a known complication of anterior cruciate ligament reconstruction (ACLR). Although the incidence of cyclops lesion appears to be decreasing, it remains an important cause of restriction of extension after ACLR. We reviewed the available literature regarding the cyclops lesion and syndrome and cyclops-like lesions to analyze available evidence on cyclops lesions and variants of cyclops lesions. A keyword search in PubMed, Scopus, Web of Science, and EMBASE, Ovid Medline, and Ovid journals provided 47 relevant articles in the English literature, which were used to create this review. We classified cyclops lesions based on clinical presentation, pathology, and location. Risk factors, management options, tips to reduce the condition, and controversies related to the condition have been discussed. Female sex, greater graft volume, bony avulsion injuries, excessively anterior tibial tunnel, double-bundle ACLR, and bicruciate-retaining arthroplasty appear to predispose patients to cyclops lesions. Cyclops syndrome is a cyclops lesion that causes a loss of terminal extension. Arthroscopic debridement is an effective treatment for cyclops syndrome, whereas cyclops lesions are usually managed conservatively. It is important to distinguish between cyclops lesion and cyclops syndrome, as management differs based on symptoms. Cyclops lesion is diagnosed using magnetic resonance imaging. The management of choice for symptomatic lesions is surgical excision. Outcomes after excision are very good, and recurrence is rare.
Keywords
Cyclops lesion, also known as localized anterior arthrofibrosis, was first described by Jackson and Schaefer in 1990. 14 It is a fibrous nodule of granulation tissue that is located anteriorly along the graft after an anterior cruciate ligament reconstruction (ACLR). A cyclops lesion with loss of extension of the knee with or without an audible or palpable clunk in terminal extension constitutes the cyclops syndrome. 14 The incidence of cyclops syndrome has been reported to be between 1% and 10% of all ACLRs, 3,14,20 whereas magnetic resonance imaging (MRI) studies have reported an incidence of 25% to 47% for cyclops lesions. 9 The incidence of all types of cyclops progressively increases with time: One study 9 reported that the incidence increased from 25% at 6 months after ACLR to 33% by the end of 1 to 2 years, whereas another study 11 reported a 46.8% incidence by 1 year of which only 10.6% of cases were symptomatic.
The purpose of this review was to analyze the available evidence on cyclops lesions and variants of cyclops lesions.
Methods
The first keyword search was performed on March 10, 2019, using the keywords ((cyclops OR “anterior arthrofibrosis” OR cyclopoid) AND (knee)) to identify articles on cyclops lesion. Before publication of this manuscript, an updated search using the same keywords was performed on December 25, 2019. Databases searched were PubMed, Scopus, Web of Science, EMBASE, and Ovid Medline. All references from the search were screened, and relevant articles were selected. Duplicates from different databases were removed. Search and selection were performed by 2 authors (S.B.S.K. and S.S.).
There were 133 references from PubMed; 123 from Scopus, 9 from Web of Science; and 494 from EMBASE, Ovid Medline, and Ovid journals. Of these, 87 appeared relevant for this study on the preliminary survey. After further analysis and exclusions, 47 articles from the English-language literature were used to prepare this review. The available literature consisted mostly of case reports and case series.
Results
Pathology of the Cyclops Lesion
The cyclops lesion is a pedunculated or nonpedunculated nodule of fibrovascular tissue. The arthroscopic appearance with its overlying blood vessels gives the appearance of a “cyclops.” 14 The most common site is the anterolateral aspect of the tibial insertion site of the ACL graft 14 (Figure 1). The nodule ranges in size from 3 × 5 mm to 8 × 12 mm. 21 Microscopically, the cyclops lesion has demonstrated peripheral fibrous tissue with a central region of granulation tissue in all specimens. Some specimens also have contained bone or cartilaginous tissue. 14 Muellner et al 22 noted that symptomatic cyclops lesions were hard in consistency and, on microscopy, revealed fibrocartilaginous tissue with active bone formation in the center. However, asymptomatic lesions were soft and only had fibrocartilaginous islands surrounded by granulation tissue on microscopy. The investigators termed the latter as “cyclopoid” lesions.

Sites of occurrence of cyclops lesion and its variants: classic cyclops lesion at the tibial attachment of the anterior cruciate ligament (ACL) graft (A), inverted cyclops lesion at the femoral side (B), and atypical cyclops lesion in the midsubstance of the ACL graft (C).
Atypical lesions may be covered with a layer of synoviocytes. 38 When the lesion occurs after grafting using a ligament augmentation device, histological analysis shows chronic inflammation with multinucleated giant cells 17 similar to foreign body reaction.
In atypical cyclops lesions after partial ACL tears, the nodule will be found adherent to the anterolateral part of the ACL, 38 presumably the tear site (Figure 1).
Variants of Cyclops Lesions
Inverted Cyclops Lesion
Inverted cyclops lesion has been described as a fibrous nodule arising from the femoral notch instead of the tibia. Only 5 reports of this lesion have been published, and it has been associated with T-shaped intercondylar fracture of the femur, 12 autologous ACLR using bone–patellar tendon–bone (BPTB) graft, 30 4-strand hamstring grafts, 16 or has occurred after supracondylar nailing of the femur. 15 The lesion may have a stalk leading to the femoral tunnel 30 or may occur without any connection to the femoral tunnel. 16
Cyclopoid Lesions
Cyclopoid lesions were first described by Muellner et al 22 as fibroproliferative nodules without cartilage or bone and hence softer than the classic cyclops lesion. Because cyclopoid lesions are soft, they do not restrict terminal extension, may be asymptomatic, and are detected only as incidental findings on MRI scans or during arthroscopy. If flexion is also restricted in patients, the cyclopoid lesion probably represents a general tendency toward fibrotic healing and is not due to evolution into a true cyclops. 22
Pseudocyclops Lesions
Pseudocyclops lesions mimic cyclops lesions clinically and sometimes on imaging but do not have pathological features of cyclops. These are very rare lesions.
Other Causes of Cyclops-like Presentation
Cyclops-like presentation has other causes. Gouty tophus has been reported as a cause of loss of extension and cyclops-like appearance during arthroscopy. 8 Histologically, gouty tophus consists of monosodium urate crystals and inflammatory cells. Gouty deposits are typically multiple and rarely single, 8 and the most common location is the infrapatellar fat pad region. Another cause of cyclops-like presentation reported was partial tear of an ACL graft. 33 The torn fibers distally clumped up to form a nodule resembling cyclops lesion. Other potential causes include space-occupying lesions, such as ganglia and pigmented villonodular synovitis, but these have not been reported in the setting of trauma to the knee or ACLR and hence may be incidental occurrences. They can be differentiated according to their typical histological features.
With a high incidence of ACL tears (250,000 per year in the United States 19 ), an incidence of 1% to 10% for cyclops lesions after ACLR can mean a huge burden to health care. However, no large series of cyclops lesions have been reported in the literature. It may be assumed that a large number of cyclops or cyclopoid lesions are asymptomatic and undiagnosed or that the incidence is declining because of improvements in ACLR techniques.
Classification
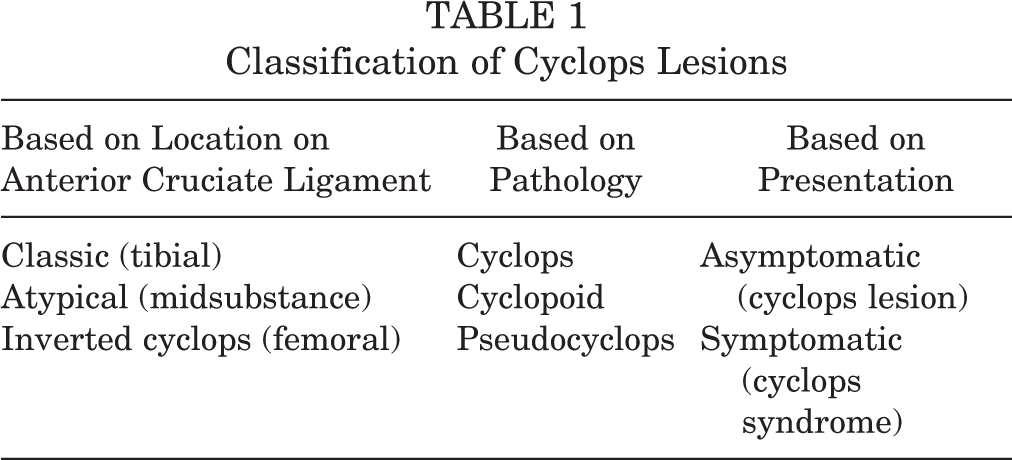
We have summarized the classification of cyclops lesions based on their location, pathological process, and clinical presentation in Table 1.
Classification of Cyclops Lesions
Etiological Factors
Cyclops lesion is a nodule or hypertrophied graft tissue and is commonly associated with a more anteriorly placed tibial tunnel or a disorganized mass of scar tissue in the anterior compartment. 6 It is the second most common cause of restricted knee extension after graft impingement. 29
Cyclops lesion has been reported with both complete tear and partial tears of the native ACL. The cause of the nodule in ACL ruptures was thought to be avulsion of pieces of bone from the tibial attachment site of the ACL. 23 Cyclops lesion has also been reported after partial avulsion of small bone pieces from proximal attachment on the femur. 35 Persistent loss of knee extension for more than 2 months even after aggressive rehabilitation after ACL rupture should raise suspicion of a cyclops lesion. 21 Microtrauma was thought to lead to granulation tissue, which leads to formation of the nodule creating the cyclops. 5 No difference has been noted in the location, histologic features, or amount of loss of extension between cyclops lesion after rupture of the native ACL and that after ACLR. 21 There is also no difference in the incidence of cyclops lesions between remnant-preserving ACLR and remnant-resecting ACLR. 35
In a study of 1012 cases of ACL injuries that entailed arthroscopies or reconstructions in China, Wang and Ao 41 found the incidence of ACL remnants was 24 (2.4%), and 19 (1.9%) of these caused extension loss. Age, acuteness of reconstruction, duration of partial weightbearing, addition of meniscal surgery, or concomitant collateral ligament injury treated conservatively did not influence results. Proportionately, more male patients had extension loss.
Cyclops lesion has been reported with different types of ACL grafts and repair and reconstruction methods, including BPTB grafts, 4-strand hamstrings and fascia lata grafts, single- and double-bundle ACLR, 34 Leeds-Keio (Dacron) scaffold, 5 Kennedy ligament augmentation device, 17 and dynamic intraligamentary stabilization device for primary repair of the ACL. 25 Most cases of cyclops lesion reported in the early literature occurred after BPTB ACLR, although no difference has been reported in the incidence of the lesion after hamstring and BPTB grafts. 27,40 However, cyclops lesion has been reported to be more common in double-bundle and quadriceps graft ACLR than in single-bundle and hamstring graft ACLR. 34 The incidence in double-bundle ACLR is 3.6%, and the cause in this case is thought to be a higher volume of the graft that impinges on the posterior cruciate ligament synovium posteriorly, with the lesion arising from the synovium of the posterior cruciate ligament rather than the graft. 34 The incidence of cyclops lesion after single anteromedial bundle biological augmentation ACLR technique (a type of remnant-preserving technique) was found to be 3.7% (5/135 cases). 26
A greater incidence of cyclops lesion in female patients, as high as 4 times greater than that in their male counterparts, has been reported by various studies. 24,27 A greater incidence has also been reported after bicruciate-retaining total knee arthroplasty 18,42 even without injury to the ACL. The cause has been proposed to be injury to the ACL during implantation of the prostheses and sharp edges of the tibial bone island. The challenge in arthroplasty is to diagnose the condition because standard MRI is not useful in the presence of metal prostheses. Ultrasonography or metal artifact reduction sequences or arthroscopy have been recommended to diagnose these cases.
A prospective study of 113 patients undergoing ACLR followed using sequential MRIs found no correlation between size of the cyclops lesion and pain or other symptoms. However, the study found a significantly higher incidence of the lesion in women and a significantly smaller notch in those with cyclops lesions. 9 von Essen et al 39 found no difference in the incidence of the lesion in patients undergoing ACLR within 8 days versus 6 weeks after injury.
Gohil et al, 11 in their MRI-based study comparing standard and stump preservation ACLR techniques, reported no difference in the incidence of cyclops lesions. In another study, anterior placement of the tibia doubled the risk of developing cyclops lesion. 37 In a review, Noailles et al 24 reported knee inflammation and/or motion restriction at the time of ACLR, narrow intercondylar notch, excessively anterior tibial tunnel, and persistent hamstring muscle spasm to be risk factors for cyclops syndrome. However, tibial and femoral tunnel sizes have not been correlated with occurrence of the lesion. 10
Although the traditional belief has been that cyclops lesion was responsible for restriction of knee extension, Pinto et al 28 identified a higher incidence of hamstring contracture–related extension deficit in patients with cyclops lesions. Whether hamstring contracture is a cause or an effect of the cyclops lesion is yet to be ascertained. Table 2 lists the risk factors for cyclops lesion.
Risk Factors for Cyclops Lesion

Diagnosis
Most cyclops lesions are asymptomatic and are found incidentally on postoperative MRI scans. Only 2% to 10% of all cyclops lesions are symptomatic. 3,8,20,24 These patients often present with loss of terminal extension of the knee, discomfort on walking or running or when lying supine, 38 and an audible or palpable clunk during terminal extension. 14 The incidence of cyclops lesion in patients with extension loss after ACLR is 1-9.8%. 29 This loss of extension of around 20° becomes symptomatic progressively over 4 months after the surgery. 20,38 Other reported causes for loss of terminal extension were suprapatellar, intercondylar, or capsular adhesions; fibrosis; and entrapment of the patella. 29
Clinical symptoms and signs have included pain at terminal extension, crepitus, painful cracking, 2 rubbery endpoint to extension with a palpable pop, 3 stiffness, residual laxity, 6 grinding with attempted extension beyond a patient’s limit, 20 joint line pain and tenderness, locking of the knee, and discomfort with climbing stairs.
The diagnosis of cyclops lesion is made in about 93% of cases within 6 months of surgery, 34 and 78% of them have extension loss within 6 weeks 43 after surgery. Cyclops lesions have been reported as late as 10 years after ACLR 17 and 23 years after chronic partial rupture without surgery. 13 If the knee appears irritated more than 4 weeks after ACLR, the likelihood of arthrofibrosis, a significant proportion of which is due to cyclops lesion, 22 should be considered.
The bounce test was described by Marzo et al 20 and consists of a rubbery feel at full extension of the knee along with a bouncing back into flexion after full extension is attained. Cyclops lesions may alter a patient’s gait by altering the sagittal and frontal plane knee movements and are associated with medial knee joint cartilage degenerative changes at 1 year after ACLR. 31
Radiographs do not show any obvious abnormalities, although they may be useful in assessing the accuracy of the position of the tunnels. MRI has sensitivity, specificity, and accuracy of 85.0%, 84.6%, and 84.8%, respectively, for diagnosing cyclops lesions. 3 When the size of the lesion increases to more than 10 mm, the specificity and accuracy increase to 100% and 91%, respectively. 3 Proton density images and T2-weighted images show intermediate signal intensity in a majority of lesions. 3 The term “MRI cyclops” is used to denote all cyclops lesions on MRI scans whether they are symptomatic or not, 11 and the incidence of these lesions has been found to be 46.8% of all ACLRs. Loss of extension was present in 23% of all patients with MRI cyclops lesion. 11 No evidence is available regarding differences in MRI appearance (eg, size, signal intensity, location) between symptomatic and asymptomatic lesions. In some cases, the ACL graft showed posterior bowing because of impingement of the cyclops lesion. 3 Persistent impingement of the ACL graft also led to high signal changes in the distal two-thirds of the graft. 3 Ultrasound examination has been used by some authors, who have described a well-defined, hypoechoic nodule attached to the tibial cortex along with hyperemia and neovascularity in the periphery. 4
Intraoperative Findings and Management
Loss of extension due to isolated full or partial rupture of the ACL may disappear under anesthesia, 32 whereas loss of extension due to cyclops syndrome will persist. 21 McMahon et al 21 found a difference in the amount of loss of extension without anesthesia and after anesthesia, with less loss of extension after anesthesia indicating that pain on impingement may have been a factor in the additional loss of extension. Cyclops lesion derived its name from its appearance during arthroscopy. The fibrous nodule appears like a head with an area of reddish-blue discoloration of venous channels giving the appearance of the eye of a cyclops. 7 On second-look arthroscopy of the knee after ACLR, the incidence of cyclops lesion has been variably reported as 21% 1 and 35%. 6 The incidence according to location of the cyclops lesion during arthroscopy 1 has been categorized as 44% near the tibial tunnel area, 27% just anterior to the reconstructed graft, 18% in front of the notch, and 20% in the area between the tunnel and the graft; 80% of these cases did not have any symptoms, and only 20% of these contributed to limitation of extension, leaving the incidence of symptomatic lesion in the overall group at less than 5%. Most limitation of extensions occurred with lesions that were larger and located in front of the graft and at the tibial tunnel. 1 The general consensus is to leave asymptomatic cyclops lesions undisturbed, whereas cyclops syndrome requires intervention to recover the normal biomechanics of the knee, although no comparative evidence is available so far.
Tonin et al 36 reported good results after excision of the lesion if done within 12 weeks of presentation and did not report any recurrence after successful surgical excision, although recurrence is common for the other causes of loss of knee extension.
The margins of the lesions should be carefully defined. Excision is done by using a shaver or bur to shave off the fibrous nodule. Intraoperatively, the knee should be taken through full range of motion (ROM) to check any impingement of the ACL graft with the roof at full extension. If impingement occurs, notchplasty is performed.
Outcomes and Prognosis
The prognosis is good with these lesions after excision. The symptoms completely resolve within a few weeks after excision of the lesion, and patients regain full ROM. 37 Recurrence has been reported only once so far, in an MRI-based study that reported 1 recurrence among 33 cases. 3
Prevention
Recommended strategies to prevent cyclops lesions include the following
2,6
: Delaying ACLR until after recovery of ROM Minimally invasive surgery compared with open ACLR Creating less debris by use of a sequential reamer and thorough removal of debris Correct tunnel positioning Debridement in and around the bone tunnel
23
Trial extension with the reamer or drill placed through the tibial tunnel to check whether it impinges with the notch Notchplasty if associated with impingement of the ACL graft If possible, drawing the graft from the femoral tunnel first into the tibial tunnel to draw debris into the tibial tunnel Early postoperative mobilization For cyclops lesion associated with bicruciate-retaining arthroplasty, selective fiber releases of the ACL, rounding of the edges of the tibial bone island, and notchplasty
18
Limitations
Most studies that we identified were case reports or small case series. Hence, a systematic review could not be performed. Quality assessment of the literature was not conducted because of the narrative nature of the review. No comparison could be made among the various treatment options. Although various preventive strategies have been proposed, there is no evidence to suggest that such strategies really work. Further, there is no evidence to suggest that the presence of cyclops lesion positively or negatively influences outcomes after ACLR.
Conclusion
Cyclops lesion is a common complication after ACLR. It is important to distinguish between a cyclops lesion and cyclops syndrome because management is needed only for the symptomatic lesion. Confirmatory diagnosis is made using MRI, and surgical excision is the management of choice for symptomatic lesions. Outcomes after excision are very good, and lesions almost never recur after excision.
Footnotes
Final revision submitted March 18, 2020; accepted April 3, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.