
Abstract
Background:
The incidence of nontraumatic fatalities in high school (HS) and National Collegiate Athletic Association (NCAA) football players has continued at a constant rate since the 1960s.
Purpose:
To describe the causes of nontraumatic fatalities in HS and NCAA football players and provide prevention strategies.
Study Design:
Descriptive epidemiology study.
Methods:
We reviewed 187 fatalities in HS and NCAA nontraumatic football players catalogued by the National Registry of Catastrophic Sports Injuries during a 20-year period between July 1998 and June 2018.
Results:
The majority (n = 162; 86.6%) of fatalities occurred during a practice or conditioning session. Most fatalities, when timing was known, (n = 126; 70.6%) occurred outside of the regular playing season, with the highest incidence in the August preseason (n = 64; 34.2%). All documented conditioning sessions were supervised by a coach (n = 92) or strength and conditioning coach (n = 40). The exercise regimen at the time of the fatality involved high-intensity aerobic training in 94.7%. Punishment was identified as the intent in 36 fatalities. The average body mass index of the athletes was 32.6 kg/m2. For athletes who died due to exertional heat stroke, the average body mass index was 36.4 kg/m2, and 97.1% were linemen.
Conclusion:
Most nontraumatic fatalities in HS and NCAA football players occurred during coach-supervised conditioning sessions. The primary cause of exertion-related fatalities was high-intensity aerobic workouts that might have been intended as punishment and/or excess repetitions. Exertion-related fatalities are potentially preventable by applying standards in workout design, holding coaches accountable, and ensuring compliance with the athlete’s health and current welfare policies.
Football, one of the most popular team sports in the United States, is also associated with the highest number of fatalities for any high school (HS) or college sport. 6,23 From the 1960s to the 2010s, the incidence of traumatic deaths declined sharply in HS and college football, reflecting the ban on spear tackling, new helmet design, and medical care of brain injuries. 7 During this time, however, there has been less focus on preventing nontraumatic deaths in football players. This may be because of traumatic fatalities occurring mostly during games and being defined as a direct result of the sport, whereas nontraumatic fatalities were erroneously defined as not being directly caused by sport participation. There is a perception that trauma may be mitigated via rules and equipment. In contrast, nontraumatic fatalities imply inherent individual frailty for which neither sport practices nor practitioners are deemed responsible.
An index point in National Collegiate Athletic Association (NCAA) football is circa 2000 when year-round training became common. 2 Since 2000, nontraumatic deaths have exceeded traumatic deaths: 2-fold in HS and 4-fold in college. 7 Therefore, we hypothesized that football conditioning programs have inherent design flaws, leading to fatalities. This is part 2 of a 2-part study; the purpose of part 1 was to compare the incidence of nontraumatic fatalities with that of traumatic fatalities, describe the epidemiology of nontraumatic fatalities in HS and college football players, and determine the effectiveness of NCAA policies to reduce exertional heat stroke (EHS) and exertional sickling (ES) with sickle cell trait (SCT) fatalities. 7 The aim of part 2 was to explore the characteristics of the training programs to determine the causes of nontraumatic deaths in HS and NCAA football players. After the causes of these fatalities are identified, prevention strategies can be developed and implemented. 1
Methods
This study was ruled exempt from institutional review board oversight. The injury definitions, methodology, and number of reports reviewed were described in part 1 of this study. 7 Football fatalities were limited to HS and NCAA athletes between July 1998 and June 2018. In addition to the data collected in part 1, information was obtained on player characteristics (age, weight, height, body mass index [BMI], position played, and game or practice). The month of the fatality was categorized as out-of-season (January through August), preseason (August, a subdivision of out-of-season), and playing season (September through December). Exercise regimens at the time of the fatality were defined as high-intensity aerobic training if the athlete was performing at least 1 of the following tasks: serial sprints, agility drills, fitness tests, exercising at a work-to-rest ratio greater than 1:3, or running for greater than 30 minutes without a break. Low-intensity exercise was categorized as weight lifting, jogging, or games (average work-to-rest ratio, 1:8). 31 Although the intent of punishment may be difficult to establish, we identified cases based on the NCAA description of punishment workouts as a corrective response to poor performance and being inconsistent with the conditioning level of the athlete or team. Punitive workouts are motivated by anger or frustration, are unplanned, and are not based on sound principles of exercise science and physiology; rather, they are employed to make athletes “tougher” or to create a team culture of “accountability.” 39 To augment the definition, we only included cases in which a teammate or independent observer reported that the coach was being abusive (bullying or taunting players who, before their demise, were visibly struggling to finish). Supervision of the conditioning session by a coach or strength and conditioning (S&C) coach was assessed. Weather conditions on the day and at the time of each fatality were obtained from the National Climatic Data Center for EHS and ES with SCT fatalities. 34
Results
During the study period, there were 187 nontraumatic fatalitites in HS and NCAA football players (Table 1). 7 Most (n = 162; 86.6%) fatalities occurred during a practice or conditioning session as compared with a game (n = 25; 13.4%) (Figure 1). All EHS, ES with SCT, and NCAA fatalities occurred during conditioning. Most fatalities, when timing was known, (n = 126; 70.6%) occurred outside of the regular playing season (Figure 1). August (n = 64; 34.2%) was the deadliest month and was when 55.8% of the EHS fatalities occurred. The majority of EHS (n = 40; 93.0%) and ES with SCT deaths (n = 18; 81.8%) occurred during off-season conditioning sessions. The exercise regimen before the death was determined in 113 of the conditioning sessions: 107 (94.7%) consisted of high-intensity aerobic training including all EHS and ES with SCT fatalities (Table 1). Punishment was identified as the intent in a minimum of 36 cases. Case examples and case reports of high-intensity aerobic training sessions and punishment drills are listed in Appendices 1 and 2. A minimum of 6 practices in which a fatality occurred had multiple players who required medical attention, with at least 3 requiring ambulance transportation to the emergency department. All documented conditioning sessions were supervised by a coach (n = 92) or S&C coach (n = 40).
Demographic Data and Playing Conditions a

a Data are presented as n (%) unless otherwise specified. BMI, body mass index; EHS, exertional heat stroke; ES exertional sickling; SCA, sudden cardiac arrest; SCT, sickle cell trait.
b The exercise regimen was known in 113 cases.
c The player’s position was known in 119 cases. All percentages are based on total number of known data points (SCA = 63; EHS = 35; ES with SCT = 12; asthma = 6).
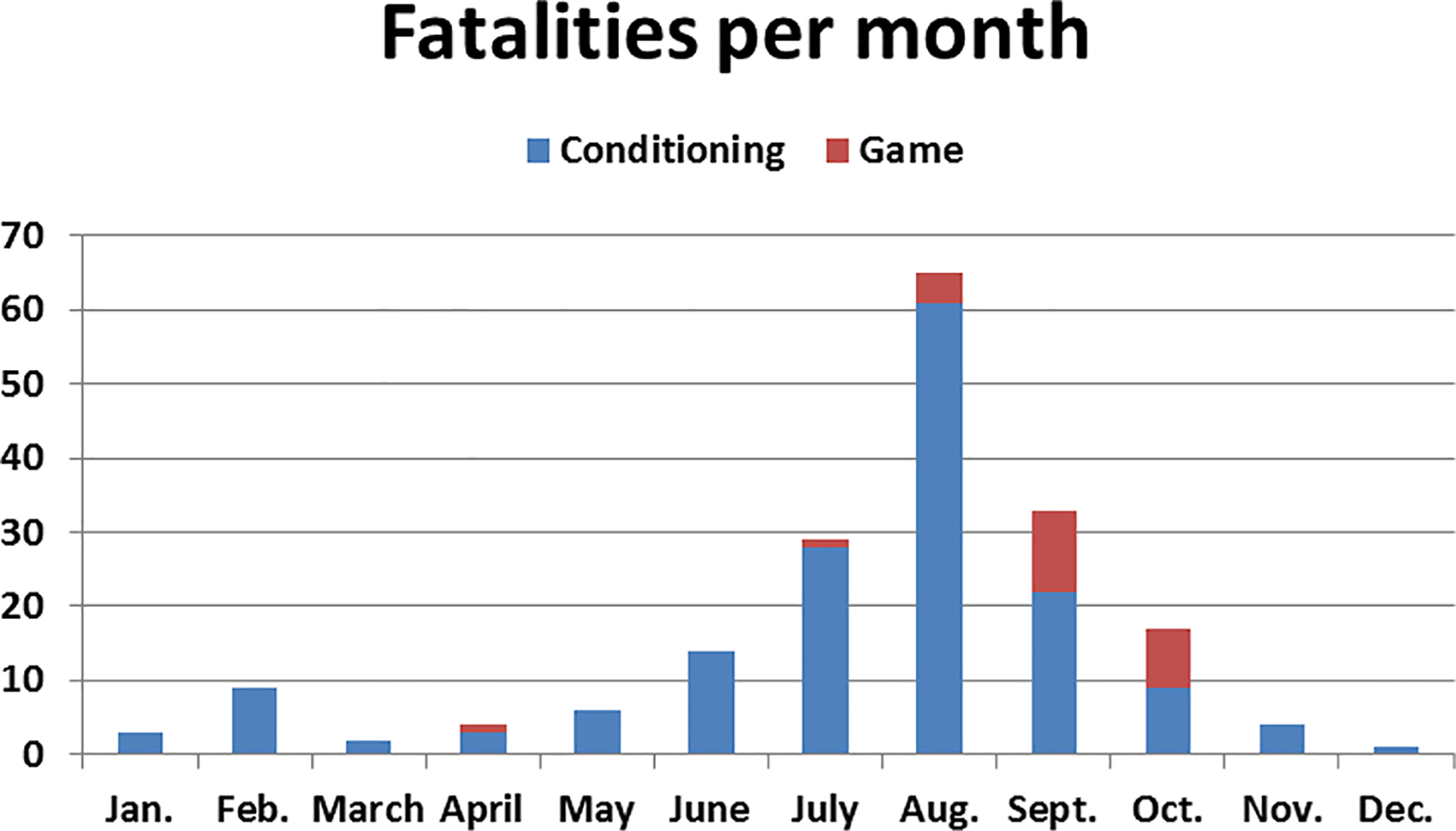
Number of fatalities in football players per month during conditioning/practices versus games.
The average age, height, weight, and BMI were 16.5 years, 72.3 inches (183.54 cm), 242 lb (108.9 kg), and 32.6 kg/m2, respectively (Table 1). Athletes with EHS had the highest average BMI (36.4 kg/m2). The position played by the athlete was determined in 119 cases, with 79 (66.4%) linemen, 11 (9.2%) running backs, 10 (8.4%) linebackers, 7 (5.9%) defensive backs, 5 (4.2%) wide receivers, 4 (3.4%) tight ends, and 3 (2.5%) quarterbacks. Athletes with EHS had the highest percentage (97.1%) playing the lineman position.
Causes
Part 1 of this study reports the number, annual average, and incidence of fatalities for total and specific diagnoses at the HS and NCAA levels (see Table 1) as well as the percentage of each diagnosis (see Figure 3). 7
Sudden Cardiac Arrest (SCA) (n = 105; 57.7%)
The specific diagnoses are provided in the cardiac results section of the companion paper. 7 The majority (n = 82; 78.1%) of SCA fatalities occurred during a conditioning session. All game fatalities occurred in HS athletes. The exercise regimen was determined in 42 fatalities: sprinting in 31, intense agility drills in 6, work-to-rest ratio greater than 1:3 in 1, and low-intensity exercise in 4 cases. Punishment drills were recorded in 14 SCA cases. In 1 case, the athlete died while performing 2 hours of conditioning drills, including repetitive sprints, with full pads as a punishment for poor performance in a scrimmage the day before the incident. There were 11 athletes who had symptoms in a previous practice (n = 7) or abnormality on the preparticipation physical examination (PPE; n = 4) that was not fully investigated by the physician or for which medical instructions were provided but neglected by the parents.
EHS (n = 43; 23.6%)
All of the EHS fatalities (100.0%) occurred while athletes were performing high-intensity aerobic training during a conditioning session. A total of 34 of 35 (97.1%) fatalities from EHS occurred in either offensive or defensive linemen; 1 (2.9%) in a fullback; and 6 in players whose positions were unknown. Overall, 16 EHS cases were reported after punishment drills in response to a player missing an earlier practice, arriving late to a practice, or coach-perceived lack of effort. In 5 cases, water restriction was an identified component of the punishment sessions. In 1 fatality, a 315-lb (141.75-kg) lineman was required to perform 36 sprints with the team from sideline to sideline (Appendix 1). Despite struggling and falling to his knees, the coach encouraged him to continue.
The exact timing of the fatality was determined in 17 cases: 7 (41.1%) on the first day of practice, 8 (47.1%) on days 2 through 5, and 2 (11.8%) on days 6 through 14. The equipment worn was identified in 10 cases: 7 (70.0%) in players wearing no pads with or without a helmet and 3 (30.0%) in athletes wearing full equipment. The region of the heat-related death was identified in 42 cases and unknown in one. Of the known cases, most occurred in the South (n = 29; 69%), followed by the Midwest (n = 8; 18.6%), the Northeast (n = 3; 7.0%), and the West (n = 2; 4.7%); the location was unknown in 1. The states with the most fatalities were Georgia (n = 4) as well as Florida, Indiana, Maryland, and Kentucky, with 3 each.
The average maximum temperature and average maximum wet-bulb globe temperature (WBGT) recorded on the day of the fatality were 90.8°F (range, 76°F-104°F) and 76.7°F (range, 65°F-94°F), respectively (Table 2). The core body temperature at the hospital, identified in 13 cases, averaged 107.8°F (range, 105°F-111°F). The time of death from the onset of EHS symptoms was within 24 hours in 27 (62.8%) athletes, greater than 24 hours but less than 2 weeks in 14 (32.6%) athletes, and greater than 2 weeks in 2 (4.7%) athletes.
Weather Conditions for ES With SCT and EHS on Day of Fatality a
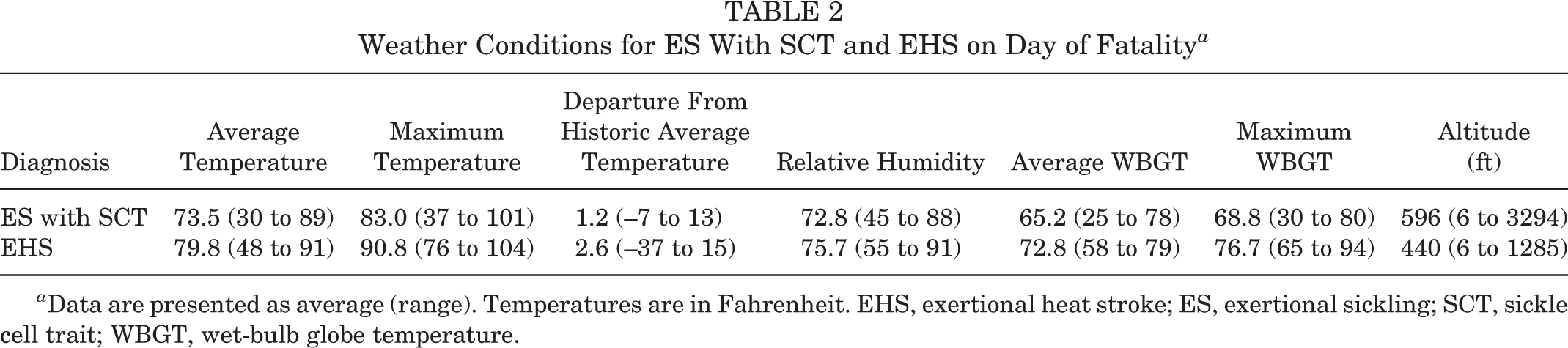
a Data are presented as average (range). Temperatures are in Fahrenheit. EHS, exertional heat stroke; ES, exertional sickling; SCT, sickle cell trait; WBGT, wet-bulb globe temperature.
ES With SCT (n = 22; 12.1%)
All ES with SCT deaths (n = 22; 100.0%) occurred while athletes were performing high-intensity aerobic training during a conditioning session supervised by the coach or S&C coach (Table 1). At least 8 incidents had a component of punishment. In one 2001 ES with SCT fatality, the athletes were performing their annual mat drills, referred to as “10 days of hell” 42 (Appendix 1). Overall, 3 segments, lasting 21 minutes each, of intense conditioning drills were performed with no break between segments. Stations were set up with trash cans for vomiting. According to one report, the assistant coach traditionally addressed the players on the first day of mat drills by stating, “You will pass out before you die. If you pass out, the trainers will take care of you.” 42 The athlete had passed out the previous week while performing similar drills.
A total of 6 ES with SCT deaths occurred during the first day of regular-season (n = 3), off-season (n = 2), or summer (n = 1) practice; 3 of the conditioning sessions were held indoors. For the remaining 19 cases, the average maximum temperature and average maximum WBGT recorded on the day of the fatality were 83.0°F (range, 37°F-101°F) and 68.8°F (range, 30°F-80°F), respectively (Table 2).
Asthma (n = 9; 4.9%)
A total of 8 (88.9%) of the 9 asthma deaths occurred during conditioning sessions. In the lone NCAA case, 1 athlete performing the requisite 28 serial sprints (2160 yd) with a 1:1 work-to-rest ratio developed breathing difficulties and died; 4 other athletes who collapsed during the same intense workout required attention at the emergency department (Appendix 1).
Hyponatremia (n = 3; 1.6%)
A total of 3 deaths resulted from hyponatremia, all during the month of August: 2 during a practice and 1 during a game. Symptoms before death included confusion, headaches, slurred speech, vomiting, and seizures. All 3 athletes died as a result of cerebral edema from excessive hydration. One athlete consumed 4 gallons of water and electrolyte beverages between practice sessions.
Discussion
The most glaring finding in this study is that most (86.6%) nontraumatic fatalities (100.0% of EHS, ES with SCT, and NCAA) in HS and NCAA football athletes did not occur while competing in a game but rather during conditioning sessions supervised by a coach or S&C coach. The risk of nontraumatic exertion-related fatalities in practice sessions was previously identified. 3,6 The causes and preventive strategies become evident in this robust data set and demonstrate a common theme of high-intensity aerobic exercise activity during out-of-season training, with lineman being an at-risk position, especially in EHS fatalities. While these fatalities may appear as isolated events, when assessed together over 20 years, they demonstrate a recurrent problem, indicating that extreme conditioning is unjustifiable.
In football, training is often by tradition, as athletes become coaches and tend to train future generations as they were trained. 13 A common scenario is a coach, angry at a perceived lack of effort, subjecting players to excessive sprints and other conditioning drills. The focus is more on creating toughness and discipline than developing football fitness and skills. 3,24,42 There is no evidence supporting the practice that abuse in conditioning enhances athletic performance or winning. In fact, this report demonstrates predictive adverse consequences from this coaching strategy. Establishing that exertion-related nontraumatic fatalities are directly caused by poorly organized training sessions versus inherent medical conditions is intrinsic to strategies preventing these deaths.
Although this report focused on fatalities, documented nonfatal EHS, ES with SCT, and exertional rhabdomyolysis cases are occurring via similar overexertion methods. 16 –18 The incidence of team outbreaks of exertional rhabdomyolysis due to excessive conditioning drills and a requirement that all athletes exert at the same pace and intensity is equally concerning. 17 The pattern is clear: coaches exposing players to extreme drills and novel exertion. The drills are often designed to intimidate or punish athletes with the intent to inflict pain and push to the limit in the false belief that there is no limit. This pattern of coach-induced overexertion in nonfatal events is similar to the exercise regimens causing nontraumatic fatalities in this study. 17 Regulating this training is overdue.
The findings in this study reveal that the workout leading to death often involved serial sprinting with high work-to-rest ratios. This contrasts with a football game, where most plays last on average 4 to 8 seconds with approximately 35 to 55 seconds of rest between standard plays and 15 to 20 seconds during hurry-up, no-huddle offense. 20,31,40 Football drills should mimic game situations with applicable work-to-rest ratios. Conditioning programs should have a lower work-to-rest ratio early in the season, with a gradual progression over time. 9 Conditioning drills should never be employed as retribution.
In this study, the majority of fatalities, especially EHS cases (average BMI, 36.4 kg/m2), occurred in linemen. Training regimens should be designed to be position specific, with, for example, skill players versus linemen, given differing sport demands and player habitus. This is also critical in at-risk players and settings, such as diminished level of player fitness, athletes returning from extended rehabilitation, transition to off-season and/or preseason, hot and/or humid conditions, and athletes with SCT. All transition periods (preseason, start of off-season, and return from injury) should allow for a minimum 7- to 10-day acclimation in exercise intensity with apt work-to-rest ratios. The S&C coach should work cooperatively with the medical staff in developing exercise science–based workout plans focused on sport-specific conditioning with a priority to improve sport skills. 9 Further research is clearly necessary to determine safe work-to-rest ratios based on sport specificity and individual fitness level. One prevention strategy is to publicly post conditioning programs to foster accountability.
While overexertion is a primary component of a nontraumatic fatality, these fatalities, as evidenced by the case examples and reports (Appendices 1 and 2), may be accompanied by an inadequate medical response, even in the presence of an athletic trainer (AT). Instead of immediate withdrawal of a struggling athlete for assessment and treatment, the ATs often ignored distressed athletes, exhorted athletes to continue through the symptoms and complete the drill, or did not enact immediate proper treatment. This may partially be caused by subjection of ATs to a coach who prioritizes “performance” over medical care, with pressure to conform to a coach’s desire of teaching toughness in which medical care is considered as contributing to weakness of the mind and body. One solution to this problem, which has received consensus support 9,11 and has been adopted by the NCAA as a bylaw, 37 is “to establish an administrative structure that provides independent medical care and affirms the unchallengeable autonomous authority of primary health care providers to determine medical management and return-to-play decisions related to student-athletes.” 38
Sudden Cardiac Arrest
The results of this study also indicate that intense physical activity can trigger covert cardiac conditions. However, compared with EHS, ES with SCT, and asthma fatalities, it is more difficult to directly link overexertion and cardiac deaths, as 23 of the cardiac fatalities, all in HS athletes, occurred during a game. In a report of sudden death due to a cardiovascular cause, there was a noted association with intense physical activity. 28 Although overexertion is surely not the sole cause, it is a predominant component of sport-related cardiac fatalities for football players in training, with 99% of college SCA fatalities occurring during a practice or conditioning session.
Prevention strategies for cardiac fatalities include detecting cardiac abnormalities during the PPE, establishing and rehearsing an emergency action plan (EAP), and immediate on-field treatment of SCA using an automated external defibrillator (AED). 8 Despite the focus on detecting covert cardiovascular conditions during the PPE, effective methods with high detection rates are lacking. 27 –29 Until cost-effective screening tests better identify at-risk athletes, priority should be placed on identifying athletes with previous exertion-related symptoms, noting abnormalities on the PPE, and completing any requested cardiology work-up based on PPE findings. While screening for cardiac conditions in the athlete has had limited effectiveness, athletes who experience SCA during exercise on HS campuses have a high survival rate, with immediate recognition and AED application within 3 minutes. 8,12
Exertional Heat Stroke
We believe that the reason for failure of the 2003 out-of-season NCAA guidelines 7 and the persistent rate of HS EHS fatalities is that current guidelines focus on the environment and uniform as causes of EHS while ignoring body habitus and exertion. 8,10 We recommend a paradigm shift to prevent overexertion, the primary component of EHS fatalities. 41 In this study, athletes were commonly performing bursts of intense exercise, typically sprinting. This supports EHS as predominantly exertional, not environmental. 18,41 A second critical risk factor for heat stroke is body habitus, with 97.1% of the fatalities in this study occurring in linemen who had an average BMI of 36.4 kg/m2. During intense exertion, they have a diminished capacity to shed metabolic heat. Linemen should not be trained the same as skill players. Modifying exercise regimens for linemen and eliminating sustained, intense aerobic training are critical prevention recommendations. The weather conditions in this report did not reveal exceedingly hot environmental conditions, further implicating exertion. The average maximum temperature and average maximum WBGT on the day of the fatalities were only 90.8°F and 76.7°F, respectively, indicating that temperatures were most likely in the high 80s or low 90s during sport participation. However, there was an average 2.6°F elevation of temperature from normal in the EHS fatalities, which argues for the necessity of regional activity modification guidelines based on the change in weather conditions from baseline as opposed to universal WBGT thresholds that do not account for large changes in weather conditions. 19 The football uniform may be overstated as an EHS risk factor. Overall, 70.0% of athletes with EHS fatalities in this report where the equipment worn was known were wearing shorts and a T-shirt, indicating that conditioning football players without pads, with or without a helmet, does not confer “safe” training. Last, hydration does not provide immunity from EHS. Most coaches, apart from the punishment reports, repeatedly avowed that they were providing frequent water breaks. Hydration is important, but dehydration is not the primary contributing factor for EHS.
Unlike SCA in which the athlete collapses and dies within minutes, in EHS deaths, the demise often occurs over several hours. In a minimum of 12 EHS cases, the athlete was found in distress after the practice. These findings support the continuation of monitoring, especially for high-risk athletes, even after completion of the practice sessions.
A renewed focus on acclimation with attention to baseline fitness, position-specific conditioning for linemen, regional acclimatization accounting for changes in baseline weather conditions, recognition of EHS signs and symptoms, a well-rehearsed EAP, and mandatory availability of an ice bath is recommended.
ES With SCT
The primary precipitating factor for all ES with SCT fatalities in this study, and corroborated by others, 14,15 was sustained vigorous bouts of conditioning drills or sprints without adequate rest periods, which triggered sickling and explosive rhabdomyolysis. 16 A minimum of 36% of the episodes were associated with punishment drills. SCT status knowledge is an invaluable clinical determinant. 7 Natal screening tests should be easily accessible by a medical professional. SCT status must be confirmed on the PPE for all sports at all levels. The PPE provides a key opportunity for counseling an athlete with SCT with specific education for the risk of ES before the commencement of strenuous athletic participation. 43 In the lone NCAA Division II ES with SCT fatality, the athlete signed a waiver declining the screening (Appendix 1). The NCAA must eliminate the opt-out waiver and require SCT status knowledge for all athletes.
The NCAA provides a proven model for the prevention of ES with SCT. 7,36 When the status is known, targeted education follows, tailored precautions are implemented, and significant morbidity and mortality due to ES with SCT are prevented. 7 There were 10 Division I football ES with SCT deaths in the 10 years before the NCAA screening and precautions began in 2010 and only 1 Division I death in the 9 years after the bylaw was adopted. 1,7,16 According to the NCAA Sports Medicine Handbook, athletes with SCT should be allowed to train at their own pace; receive adequate hydration; be excused from performance tests, such as serial sprints or timed miles; never be urged to exercise at 100% beyond 2 or 3 minutes without a break; and discontinue activity upon struggling or experiencing symptoms. 35 There were no recorded HS or NCAA ES deaths when the SCT status was known, education ensued, and precautions were heeded.
Unlike athletes with heat stroke, athletes with ES with SCT can collapse after a brief period of intense exercise. In contrast to SCA, athletes with ES with SCT can usually talk after they hit the ground. ES with SCT is a medical emergency. High-flow oxygen of 15 L/min with a non-rebreather mask should be initiated. Vital signs should be monitored, and if obtunded, the EAP should be activated. Emergency department physicians should be notified of the athlete’s SCT status and be warned of the possibility of explosive rhabdomyolysis, engaging a nephrologist and cardiologist to address potentially grave complications.
Asthma
Both our results (88.9%) and those of a comprehensive study (78%) 5 on asthma deaths in athletes demonstrate that the majority of asthma-related deaths in organized sport occurred during a practice session. In the lone fatality in a college athlete, the workout required serial sprints at a 1:1 work-to-rest ratio, evidencing overexertion’s role in these fatalities. 26 Prevention strategies for asthma-related deaths require parents and guardians of athletes with asthma to notify all medical personnel and the coaching staff of their medical condition and treatment plan, listing medications and the person responsible for ensuring that medications are present during practices and competitions. 21
Hyponatremia
Hyponatremia in young athletes participating in team sports is rare and was identified in only 3 athletes in this study. One athlete in this study consumed 4 gallons of water and electrolyte beverages between practice sessions. The treatment of early hyponatremia requires medical referral for observation, restriction of fluids, and ingestion of hypertonic fluids or salty foods. For advanced cases, rapid sodium replacement with a hypertonic saline infusion intravenously is recommended. Prevention is paramount and best accomplished by educating athletes regarding fluid replacement and the potential risks of hyperhydration. 30
Limitations
Our study is limited in that we were not able to document the exercise program in all of the cases. Nonetheless, the high percentage of documented cases in athletes performing high-intensity aerobic conditioning, all non-SCA cases, plus the numerous reports of punishment indicate that this trend likely would have persisted in the remaining cases. Nonetheless, this is the most comprehensive study on nontraumatic fatalities in football players, containing abundant information to substantiate our hypothesis that the primary cause of nontraumatic fatalities is overexertion.
Conclusion
The majority of nontraumatic fatalities in HS and NCAA football athletes did not occur in games but rather during out-of-season, coach-supervised conditioning sessions. The primary cause of exertion-related fatalities was intense aerobic workouts, often associated with punishment drills, with linemen being an at-risk group for EHS fatalities. Exertion-related fatalities are potentially preventable via an organizational structure: applying exercise science in the workout design based on position played and body habitus, holding coaches accountable, and ensuring compliance with the athlete’s health and current welfare policies. Further research is necessary to develop safe conditioning programs.
Footnotes
Final revision submitted April 2, 2020; accepted April 23, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.M.F. has received consulting fees from Flexion Therapeutics. AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the University of Oklahoma.