
Abstract
Background:
Success rates for surgical management of chronic exertional compartment syndrome (CECS) are historically lower with release of the deep posterior compartment compared with isolated anterolateral releases. At our institution, when a deep posterior compartment release is performed, we routinely examine for a separate posterior tibial muscle osseofascial sheath and release it if present.
Purpose:
Within the context of this surgical approach, the aim of the current study was to compare long-term patient satisfaction and activity levels in patients who underwent 2-compartment fasciotomy versus a modified 4-compartment fasciotomy for CECS.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients treated with fasciotomy for lower extremity CECS from 2007 to 2017 were retrospectively identified. In all patients in whom a 4-compartment fasciotomy was indicated, the tibialis posterior muscle was examined for a separate osseofascial sheath, which was released when present. Patients completed a series of validated patient-reported outcome (PRO) surveys, including the Marx activity score, Tegner activity score, 12-Item Short Form Health Survey, and Likert score for patient satisfaction.
Results:
Of the 48 patients who were included in this study, 34 (71%) patients with a total of 52 operative limbs responded and completed PRO surveys. The mean follow-up for the entire cohort was 5.5 ± 2.6 years. Of the 34 patients, 23 (68%) underwent 2-compartment fasciotomy and 11 (32%) underwent 4-compartment fasciotomy. Among the patients in the 4-compartment fasciotomy group, 7 (64%) were found to have a fifth compartment. No significant difference was found in any of the validated PRO measures between patients who had a 2- versus 4-compartment fasciotomy or those who underwent 4-compartment fasciotomy with or without a present fifth compartment. At a mean 5.5-year follow-up, 74% of patients who underwent a 2-compartment release reported good or excellent outcomes compared with 82% of patients who underwent our modified 4-compartment release.
Conclusion:
The current study, which included the longest follow-up on CECS patients in the literature, demonstrated that the addition of a release of the posterior tibial muscle fascia led to no significant difference in PRO measures between patients who underwent a 2- versus 4-compartment fasciotomy, when historically the 2-compartment fasciotomy group has had higher success rates.
Chronic exertional compartment syndrome (CECS) of the lower leg is an overuse injury that carries significant morbidity in the athletic population. 3 CECS has long been treated with surgical decompression through open fasciotomy of the symptomatic compartments. 16 –18 The deep posterior compartment is the second-most common site of involvement, with the anterior compartment being the most frequent. 1,3,14,24 Compartment involvement has been shown to be a prognostic factor in successful treatment of CECS, and higher failure rates are associated with release of the deep posterior compartment. 4,5,11,15,20,22,25,26
Failure rates associated with release of the deep posterior compartment have been reported to be as high as 60%. 11 Some studies have suggested that the significantly higher failure rate associated with release of the deep posterior compartment may be related to variable anatomic features, whereby some patients possess a “fifth compartment” of the lower leg formed by a fibular attachment of the flexor digitorum longus (FDL) muscle. 9,10,19 This osseofascial sheath has the ability to compress segments of the tibialis posterior muscle (TPM), thereby raising pressures and producing the symptoms of exertional compartment syndrome. Figure 1A demonstrates a cross-sectional view of the lower leg to highlight the relationships between these structures. Several authors have stressed the importance of releasing this osseofascial sheath. 6,7,16,18,20

(A) Axial cross section of lower leg demonstrating the surgical approach used for the described fasciotomies. EDL, extensor digitorum longus; EHL, extensor hallucis longus; FDL, flexor digitorum longus; FHL, flexor hallucis longus; G(LH), lateral head of gastrocnemius; G(MH), medial head of gastrocnemius; PB, peroneus brevis; PL, peroneus longus; S, soleus; TA, tibialis anterior; TPM, tibialis posterior muscle. (B) Posterior view of cadaveric dissection with gastrocnemius and soleus retracted, demonstrating relationship of deep compartment musculature with the path of dissection in our modified 4-compartment release. The white indicator demonstrates a path anterior to the FDL along the posterior tibia. This specimen did not have a fifth compartment. (C) Posterior view of cadaveric dissection with FDL retracted to demonstrate how dissection anterior to the FDL in our modified 4-compartment release allows visualization of the TPM to examine for and potentially release the fifth compartment.
Davey et al 6 demonstrated the presence of this fifth compartment using contrast studies as well as the occurrence of isolated exertional compartment syndrome in the TPM by using intracompartmental pressure monitoring in live patients. Those authors also showed that traditional fasciotomy techniques were not effective in decompressing the TPM in their cadaveric analyses, an observation similarly made by Rorabeck et al 18 in 1988, who reported a significantly decreased success rate for deep posterior compartment release and attributed it to inadequate decompression of the TPM.
At our institution, when a deep posterior compartment release is performed, we routinely examine for an osseofascial sheath overlying the TPM and release it when present. We use a modification of the medial incision technique in dissecting anterior, rather than posterior, to the FDL muscle to reach the TPM. 12,20 Within the context of this surgical approach, the aim of the current study was to compare long-term patient-reported outcomes (PROs) in patients who underwent 2- versus 4-compartment fasciotomy for CECS. Our primary hypothesis was that there would be no significant difference in outcomes between patients who underwent 2-compartment versus modified 4-compartment release.
Methods
Patient Selection
This retrospective observational study reports on a consecutive series of patients with lower extremity CECS who underwent surgical management by the senior author (S.A.L.) at a single academic medical center between January 1, 2007, and January 1, 2017. After institutional review board approval was obtained, medical records were queried by use of International Classification of Diseases, 9th Revision code 820 and Current Procedural Terminology codes 27600, 27601, and 27602. After these parameters were applied, 76 limbs from 48 patients were available for review. The mean age of the patients at the time of surgery was 25.6 ± 8.5 years (range, 15-42 years).
Operative Data Collection
All patients underwent lower limb fasciotomy by the senior author at a single surgical center. All patients were symptomatic and had CECS confirmed by intracompartmental pressure testing before surgery according to the Pedowitz criteria. 13 Intracompartmental pressure testing was completed by an independent nonoperative partner according to standard procedure. The posterior compartment measurements were made medial and posterior to the tibia. No attempt was made to isolate the TPM, and the needle was most likely in the FDL muscle belly. Patients underwent either 2-compartment release involving the anterior and lateral compartments or a 4-compartment release involving the anterior, lateral, superficial posterior, and deep posterior compartments. For the 2-compartment release cohort, both anterior and lateral compartments were released even if only 1 compartment was symptomatic.
As part of our surgical technique, the presence of a separate TPM osseofascial sheath (fifth compartment) is routinely sought during 4-compartment release, and the presence or absence of this sheath is recorded in the operative note for every case. All patient operative reports were reviewed, and the location and total number of compartments released were recorded. The presence or absence of a fifth compartment was always recorded.
PRO Collection
All patients were contacted via telephone to obtain informed consent for participation in the current study between July 2017 and December 2019. Overall, 38 patients were successfully contacted to discuss participation in the study. We were unable to contact 10 patients because no working telephone numbers or email addresses were available. After consent was obtained, patients were asked to complete a series of validated PRO surveys, including the Marx activity score, Tegner activity score, 12-Item Short Form Health Survey (SF-12), and Likert score for satisfaction. All patients who were successfully contacted agreed to participate in the study; however, 2 patients in each group did not complete surveys despite multiple contact attempts. Similar to Schepsis et al, 20 we used a Likert scoring system that asked patients to rate their overall outcome as excellent, good, fair, or poor. Finally, patients were asked to report whether they had undergone any additional surgery on the limb of interest. A chart review was conducted for all patients included in the study to assess the incidence of complications associated with surgery as well as revision surgery rates.
Surgical Technique
All surgeries were performed with the patient under general anesthesia with thigh tourniquet control. Figure 1 provides an axial cross section demonstrating the surgical approach used for the subsequently described fasciotomy technique as well as a posterior view of a cadaveric dissection to better visualize the fascial planes relevant to the described path of dissection. The senior author used a 2-incision technique as described by Rorabeck et al 17 for the release of the anterior and lateral compartments. Two 4-cm longitudinal incisions were made, 1 proximal and 1 distal, midway between the anterior border of the tibia and fibula (Figure 2).

Demonstration of the 2-incision technique for release of the anterior and lateral compartments. Two 4-cm incisions are made, 1 proximal and 1 distal, midway between the anterior border of the tibia and fibula.
The distal incision was centered 10 to 12 cm proximal from the distal tip of the fibula, while the proximal incision was made in the proximal one-third of the leg. Careful dissection was carried down to identify the superficial peroneal nerve, where neuroplasty was completed in all cases. The anterior and lateral compartment fasciae were incised transversely at the midpoint of each incision. The anterior and lateral compartments were then longitudinally released with a long Metzenbaum scissor from their proximal origin to beyond the distal musculotendinous junction (Figure 3). The longitudinal releases were completed from the tibial tuberosity level to a point 4 to 6 cm proximal to the ankle joint line to preserve the superior extensor retinaculum.

Anterior compartment fascia divided in both a transverse and a longitudinal fashion.
For the release of posterior compartments, the senior author used a modification of the technique described by Mubarak and Owen. 12 A separate 10-cm longitudinal medial incision was made over the middle one-third of the leg 1 cm medial to the medial border of the tibia (Figure 4), and the greater saphenous vein was protected. The superficial posterior compartment was exposed and released proximally from the muscle origin to a point distal to the musculotendinous junction (Figure 5). The soleus origin along the tibia was also released under direct vision.

Demonstration of incision for access to superficial and deep posterior compartments. A separate 10-cm longitudinal medial incision is made over the middle one-third of the calf parallel to the medial border of the tibia.
(A) Exposure and (B) release of the superficial posterior compartment.
The posterior tibial vessels and nerve were visualized and protected posterior to the FDL muscle belly. Next, the senior author used a modification of the traditional technique and carried the dissection posterior to the tibia and anterior to the FDL muscle belly. The FDL was visualized (Figure 6A) and then mobilized posteriorly off its origin along the tibia to protect the posterior tibial vessels and better visualize the TPM and complete the deep posterior release (Figure 6B). The surgeon looked for a separate fifth compartment in every case that was performed (Figure 7A), and, when present, the fifth compartment was released (Figure 7B). Similar to other authors, 20,27 we did not seek to release the flexor hallucis longus fascia as a separate step. This modification is further illustrated in Figure 1.

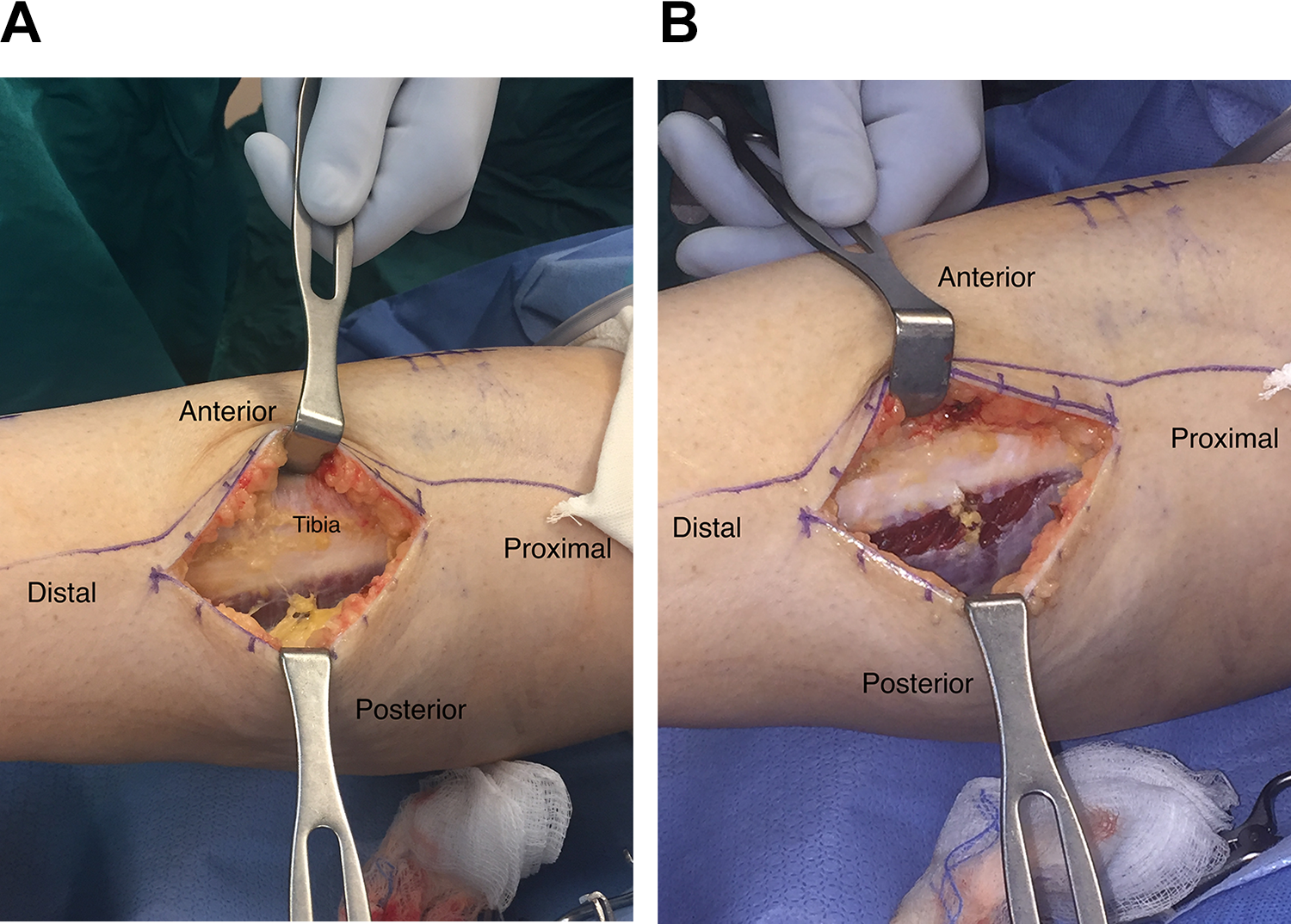
(A) Exposure of the deep posterior compartment revealing the flexor digitorum longus (FDL). (B) Release of the deep posterior compartment, dissecting anterior to the FDL and elevating it off the posterior tibia.

(A) Retraction of the flexor digitorum longus (FDL) and identification of a fifth compartment around the tibialis posterior muscle (TPM). (B) Demonstration of released fifth compartment revealing TPM, with FDL retracted.
We routinely deflated the thigh tourniquet and performed an adequate hemostasis. All patients received a Hemovac suction drain (Zimmer Hemovac; Zimmer), which was removed the following day in clinic.
Postoperative Rehabilitation
All patients were placed in a soft compressive dressing and allowed weightbearing as tolerated with crutches. Skin sutures were removed 2 weeks after surgery, and patients were weaned off crutches. We allowed full weightbearing and gradual return to activities by 6 to 8 weeks after surgery.
Statistical Analysis
For patients with bilateral operative limbs, only 1 PRO survey was used in our analysis. The distribution of continuous numerical data including all PRO scores was examined in descriptive histograms and box plots, and a Kolmogorov-Smirnov test was used to confirm a normal distribution. For descriptive analysis, absolute mean values for PRO scores were reported with standard deviations. An independent-samples t test was used to compare continuous variable PRO outcomes between patients who underwent a 2-compartment fasciotomy versus our modified 4-compartment fasciotomy. A separate independent-samples t test was used to compare continuous variable PRO outcomes between patients who underwent a 4-compartment fasciotomy with and without a present fifth compartment. Chi-square analysis was used to compare Likert scores and revision rates between the 2-compartment and 4-compartment fasciotomy groups. For all analyses, a P value less than .05 was considered significant. All statistical analyses were performed with Stata statistical software (Stata Statistical Software Release 14; StataCorp).
Results
Of the 48 patients who were included in this study, 10 patients could not be contacted, and they were considered lost to follow-up. Of these 10 patients, 7 had undergone 2-compartment fasciotomy and 3 had undergone modified 4-compartment fasciotomy. Further, 2 patients each in the 2-compartment and modified 4-compartment groups failed to complete the PRO surveys. Overall, 34 patients (71%) with a total of 52 operative limbs responded and completed the PRO surveys. The response rate for the 2-compartment fasciotomy group was 72%, and the response rate for the modified 4-compartment fasciotomy group was 69%. The final analysis included 14 (41%) male patients and 20 (59%) female patients. The mean follow-up time for the entire cohort was 5.5 ± 2.6 years (range, 1.4-12.2 years). Preoperative compartment pressures were measured only for symptomatic compartments and are shown in Table 1. In bilateral cases, preoperative compartment pressures were assessed in only 1 limb and thus were not recorded in 10 cases.
Preoperative Compartment Pressure Measurements a

a Values are expressed as mm Hg. Posterior compartment measurements were made medial and posterior to the tibia. No attempt was made to isolate the tibialis posterior, and the needle was most likely in the flexor digitorum longus muscle belly. Dashes represent intracompartmental pressure values not measured during testing. L, left; R, right.
Of the 34 patients, 23 (68%) underwent 2-compartment fasciotomy and 11 (32%) underwent 4-compartment fasciotomy. Among the patients in the 4-compartment fasciotomy group, 7 (64%) were found to have a fifth compartment (Table 2).
Individual Patient Characteristics and Patient-Reported Outcome Results a

a F, female; L, left; M, male; R, right; SF-12, 12-Item Short Form Health Survey.
We found no significant difference in any of the validated PRO measures between patients who had a 2-compartment versus 4-compartment fasciotomy (Table 3). The mean Marx activity score was 9.6 for the 2-compartment group and 10.6 for the modified 4-compartment group (P = .59). In total, 10 patients (29.4%) reported a Marx score of 15 or 16, indicating full return to high-impact athletics. The mean Tegner activity score was 5.6 for the 2-compartment group and 5.7 for the modified 4-compartment group (P = .87) indicating recreational athletics. The mean SF-12 physical component score was 51.1 for the 2-compartment group and 50.5 for the modified 4-compartment group (P = .83), and the mean SF-12 mental component score was 53.1 for the 2-compartment group and 52.4 for the modified 4-compartment group (P = .82).
Patient Characteristics and Patient-Reported Outcome Results for 2-Compartment vs 4-Compartment Fasciotomy a

a Values are reported as mean ± SD unless otherwise noted. SF-12, 12-Item Short Form Health Survey.
b Determined by 2-sample t test.
We noted no significant difference in any of the PRO measures between patients with and without a fifth compartment in the modified 4-compartment fasciotomy group (Table 4). The mean Marx activity score was 9.9 for patients with a fifth compartment and 12.0 for those without a fifth compartment (P = .51). The mean Tegner activity score was 5.7 for patients who had a fifth compartment and 5.8 for those without an identifiable fifth compartment (P = .98). The mean SF-12 physical component score was 51.5 for patients who had a fifth compartment and 48.9 for those who did not (P = .55). The mean SF-12 mental component score was 51.4 for the patients who had a fifth compartment group and 54.2 for those who did not (P = .59).
Patient Characteristics and Patient-Reported Outcome Results for 4-Compartment Fasciotomy With and Without a Fifth Compartment a

a Values are reported as mean ± SD unless otherwise noted. SF-12, 12-Item Short Form Health Survey.
b Determined by 2-sample t test.
At a mean follow-up of 5.5 years, 74% of patients who underwent 2-compartment release reported good or excellent outcomes compared with 82% of patients who underwent our modified 4-compartment release. The overall success rate among both groups was 76%. No significant difference was seen in patient satisfaction as reported by Likert scale between those who had 2-compartment versus the modified 4-compartment releases (P = .44).
Complications of surgery were documented in 5 limbs (14.7%). Of these, 2 limbs developed wound dehiscence. Both of these limbs underwent modified 4-compartment fasciotomy; 1 limb was found to have a fifth compartment whereas the other did not. Both cases resolved with local wound care. Seroma formation occurred in 1 patient undergoing isolated anterolateral release and led to delayed wound healing. This resolved after local aspiration and initiation of antibiotics. None of the 3 limbs experienced any long-term effects due to these complications. Superficial peroneal nerve dysesthesias developed in 1 patient who underwent modified 4-compartment fasciotomy and 1 patient who underwent 2-compartment fasciotomy. The symptoms in the patient who underwent modified 4-compartment fasciotomy resolved spontaneously over 12 months, whereas the symptoms in the patient who underwent 2-compartment fasciotomy have remained persistent. No patients in the modified 4-compartment group reported foot or toe deformity related to FDL release. We noted that 2 (5.9%) patients reported poor outcomes according to the Likert scale rating, both of whom had undergone 2-compartment fasciotomy. No patients in the 2-compartment or modified 4-compartment fasciotomy group underwent any additional surgical procedures in any limb; the revision rate was 0% for the entire cohort.
Among the 14 patients who were lost to follow-up, the chart review revealed no recurrence of symptoms after surgical fascial release and no occurrence of complications associated with surgery.
Discussion
The current study, which included the longest follow-up in the literature on CECS patients treated surgically, demonstrated that patients with deep posterior compartment involvement who underwent modified 4-compartment fasciotomy had no significant difference in outcomes compared with patients who underwent 2-compartment fasciotomy, when historically the 2-compartment fasciotomy group has had higher success rates. 4,20,22,25 We found that a separate osseofascial sheath existed around the TPM in the majority of our cases.
Scully and Benavides 21 recently published an article detailing their technique for fasciotomies in the treatment of CECS. Their technique was similar to that described in the current study except they elected to release the fascia of the deep posterior compartment posterior to the FDL muscle belly as opposed to dissecting anterior to the FDL and releasing it off the posterior tibia. No mention was made of examining for and releasing the posterior tibial fascia. Schepsis et al 20 reported on 46 patients with CECS. Similar to Mubarak and Owen, 12 Schepsis et al used 1 lateral incision and 1 medial incision for 4-compartment release. Schepsis et al always released both the anterior and lateral compartments, they performed deep posterior release posterior to the FDL (in contrast to our technique of anterior release), and they released posterior tibial fascia when they found it. Schepsis et al did not state the frequency of posterior tibial release. Winkes et al 27 published a prospective study detailing their surgical technique for releasing the deep posterior compartment. They dissected posterior to the FDL, released its fascia, and confirmed that the TPM osseofascial sheath was often present and released it. Similar to our experience, they did not seek to release the flexor hallucis longus fascia.
Our modified dissection was always anterior to the FDL, as the senior author believed that would protect the posterior tibial vessels and allow better visualization of the TPM. We believe that our modification may explain the improved results compared with historic literature. Previously, the success rate of 4-compartment fasciotomy in the treatment of CECS involving the deep posterior compartment has been reported as low as 40% to 48%, 11,26 although Winkes et al 27 reported a 71% beneficial outcome for isolated deep posterior compartment fasciotomy. This is compared with an 82% success rate in the current study, with 27.2% of patients participating in competitive athletics at long-term follow-up. Given the prevalence of a fifth compartment in the majority of patients undergoing a 4-compartment release, our improved long-term results suggest that our modified technique and the routine examination for and release of the fifth compartment may help surgeons achieve higher success rates in the treatment of CECS involving the deep posterior compartment.
Notably, our analysis between those patients who did and did not have a present fifth compartment within the modified 4-compartment fasciotomy group did not detect a statistically significant difference in outcome measures. We believe this is likely attributable to our small sample size. Future studies with larger cohorts could provide helpful data to evaluate our modified 4-compartment fasciotomy technique compared with more traditional techniques.
The current study found a 74% success rate with 2-compartment release involving the anterior and lateral compartments, which is lower than the reported average in the literature. A recent systematic review found the success rate of anterior compartment release to be 86% and the success rate of lateral compartment release to be 90%. 5 Despite this, it must be noted that the current study used more rigorous and validated PRO measures and reported results from the longest mean postoperative follow-up, at 66 months compared with 49 months among the studies included in the review by Campano et al. 5 It is possible that the higher reported success rates in previous studies analyzing anterior and lateral compartment release are related to shorter term follow-up and a variable definition of a successful outcome. 18
In our study, complications from surgery were documented in 5 limbs (14.7%). These included 2 cases of wound dehiscence, 1 case of seroma formation, and 2 cases of superficial peroneal nerve neuritis. All resolved over time, except for 1 case of superficial peroneal nerve neuritis, which has persisted at 7.5 years from surgery. This compares with a 13% complication rate in multiple studies summarized by Campano et al, 5 with more complications reported in long-term studies.
Previous studies have demonstrated an 8% rate of all-cause reoperation 5 compared with a 0% reoperation rate in the current study. Our findings again suggest that the use of this modified technique can decrease the need for reoperation owing to recalcitrant symptoms, especially in patients experiencing CECS symptoms of the deep posterior compartment.
As we compared outcomes with other studies in the literature, the lack of uniform and validated outcome measures across the CECS literature was evident. Therefore, there exists no clear consensus on the definition of a successful treatment. Schepsis et al 20 used a subjective questionnaire not previously validated to report their results. Other studies included in the systematic review by Campano et al 5 used a combination of Likert scale measures of outcome, patient satisfaction with the surgery, and rate of return to previous activity. The majority of these studies included a Likert scale in their outcome measures, and outcomes graded as excellent or good were considered a success. We used similar methods in the current study in order to attain comparable results with the historical literature. However, we believe that a strength of the current study is our use of additional validated patient outcome measures such as the Marx activity score, Tegner activity score, and SF-12. More recent studies have done the same and have included measures such as the Tegner activity scale, SF-12, and the EuroQol-5D index score. 2,8,23 Future studies looking at the operative treatment of CECS may continue to include these additional outcome measures to more accurately compare results of treatment techniques and develop a more standardized definition of success in the treatment of CECS.
Based on the outcome data from this retrospective study, a power analysis for a future prospective study (2-group design) was performed to better delineate the sample size required to reach a clinically significant conclusion when using these validated patient outcome measures. We chose to perform statistical power calculations on the SF-12 physical component score and assume a 5-point difference between study groups as clinically important. A sample size of 64 patients in each study group will achieve 80% power to reject the null hypothesis of equal SF-12 physical component score means when the population mean difference is μ1 – μ2 = 50 – 45 = 5, with a standard deviation for both groups of 9 points and with a significance level (alpha) of .05 when using a 2-sided 2-sample equal-variance t test.
We recognize that limitations exist in such a retrospective study. Our small study population limited our ability to detect statistically significant differences. We have provided a power analysis in an effort to highlight the numbers needed in future studies that use these validated outcome measures. Our preoperative intracompartmental pressure measures for the deep posterior compartment were not explicitly measured within the TPM belly. The needle was most likely in the FDL muscle belly during measurement. Future studies could attempt to obtain this measurement within the TPM to better assess for the effects of a fifth compartment if present. Patients were required to recall their progress over the past 10 years while completing the outcome measures. We were unable to contact 10 patients identified in the initial review; despite this, their charts were still reviewed and we found no recorded evidence of symptom recurrence after their release for the treatment of CECS. We used Tegner and Marx activity scales because they are validated measures for return to athletic activity, although they were not designed specifically for patients with CECS.
Conclusion
We found that the routine examination for and release of the TPM osseofascial sheath using our modified 4-compartment fasciotomy technique for treatment of CECS demonstrated no significant difference in PRO measures compared with 2-compartment release; further, the modified technique yielded a notable improvement in the success rates compared with the historic literature. Therefore, we recommend the use of this surgical technique in all 4-compartment fasciotomies for CECS.
Footnotes
Acknowledgment
The authors thank Brian Brockway for his assistance with creating illustrations for the manuscript. Additionally, they thank Yunyun Chen and Kirk Easley for their assistance with the statistical analysis.
Final revision submitted March 10, 2020; accepted March 20, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.A.L. has received speaking fees from Arthrex and Arthrosurface; consulting fees from Arthrosurface, Heron Therapeutics, and Stryker; and hospitality payments from Exactech. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Emory University Institutional Review Board (IRB00088598).