
Abstract

Athletes who play throwing sports, such as baseball, can experience vascular injuries at any level of the arm from the thoracic outlet to the fingertips. 1 Digital ischemia can occur in the throwing hand of baseball pitchers who perform repetitive, high-stress, high-velocity movements. Arterial injuries around the shoulder on the throwing side and in the catching hand are well-known conditions resulting in hand ischemia in baseball players 3,5,9,12,14 –16 ; however, arterial injuries of the throwing hand are not fully understood. Itoh et al 8 reported 3 cases of baseball pitchers with this condition in which release of the Cleland ligaments (on both sides of the fingers) or the lumbrical canal was successful in treating their injuries. The authors also reported that hyperextension of the proximal interphalangeal (PIP) joint in the throwing hand caused a digital arterial injury. 8
Recently, we treated 2 cases of high-level (professional or draft candidate) baseball pitchers with complete occlusion of the digital artery of the index or middle finger without any local compression, and both athletes were able to return to their original level of performance after surgical intervention. We present these cases along with a review of the literature. This study was approved by the ethical committee at our hospital, and we obtained written approval from the patients for publication of the details of their case.
Case 1
A 21-year-old right-handed professional baseball pitcher had experienced coldness, numbness, and pain during pitching for 2 months without any particular cause. He could not continue to pitch and consulted our clinic. He had been a baseball pitcher for 12 years. At the initial visit, his right index and middle fingers appeared pale, and the skin temperature was clearly low during palpation. He had a long-standing blood blister on the ulnar side of his index fingertip, and refill of the involved fingertip was quite slow. His right thumb, ring, and little fingers showed a normal appearance and temperature. He experienced no motor disturbance, and the digital Allen test revealed arterial obstruction in the middle radial and index ulnar arteries. Ultrasonography revealed complete occlusion of the index ulnar digital artery at the level of the midproximal phalanx (Figure 1A) and poor arterial flow in the index radial and middle radial digital arteries as well as in both fingertips (Figure 1B). Digital subtraction angiography showed the same condition (Figure 2). Additionally, no proximal occlusion was detected. He did not have a history of any systemic disease or smoking.

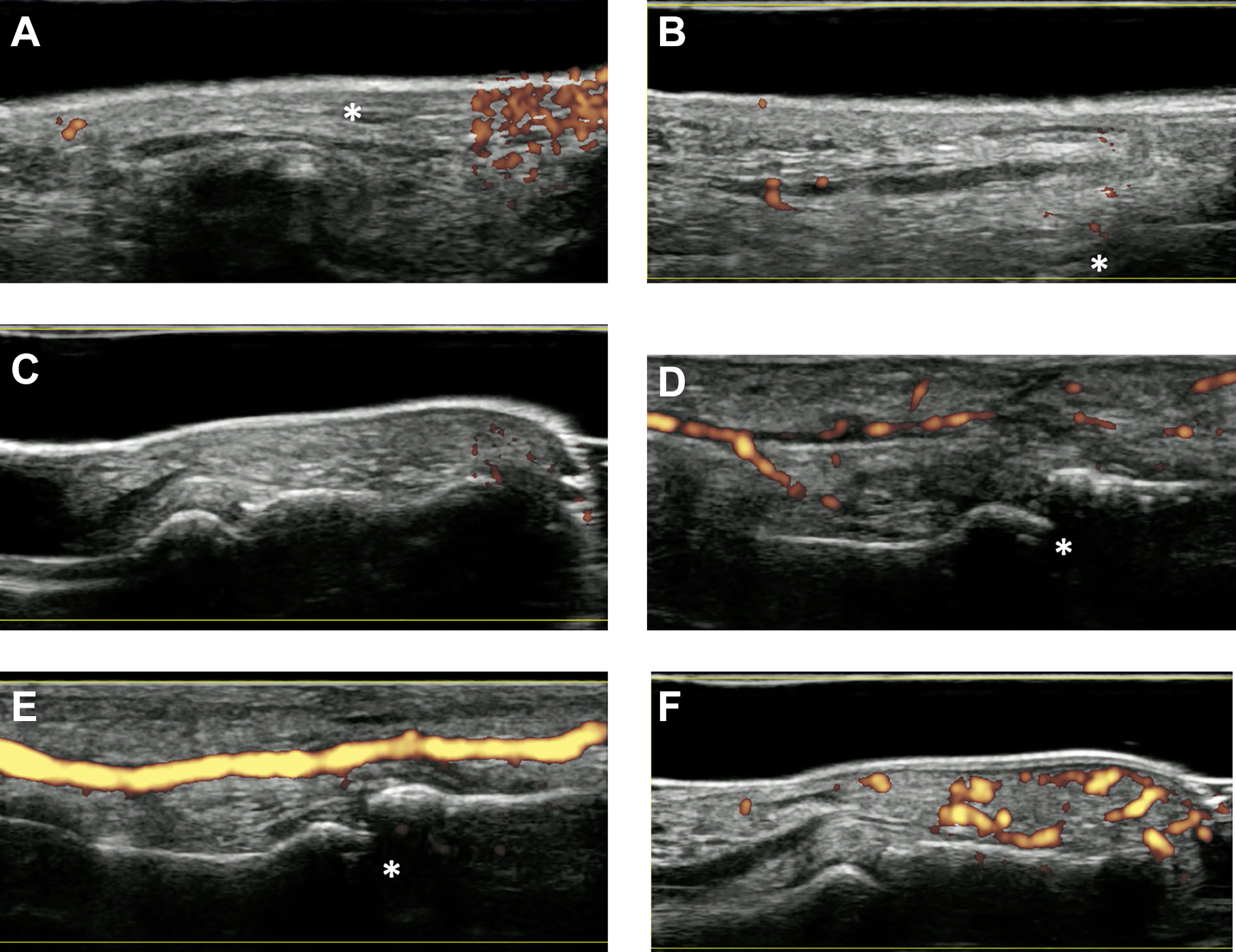
Ultrasonogram of case 1 (left: proximal). (A) Preoperative ulnar digital artery of the right index finger at the midproximal phalanx. Flow is spotty and insufficient. (B) Preoperative fingertip of the index finger. No flow is detected. (C) Postoperative 6-month fingertip of the index finger. Flow is sufficient. *The artery is occluded proximal to the proximal interphalangeal joint.

Digital subtraction angiogram of case 1. Flow in the ulnar digital artery of the right index finger is interrupted proximal to the proximal interphalangeal joint (arrow).
Nonoperative treatment with oral antithrombotic agents (200 mg aspirin and 15 μg prostaglandin E1 per day for 2 weeks) did not work, and a surgical intervention was selected. A zigzag incision was applied on the volar surface of the index finger under tourniquet control, and both digital arteries were exposed under the operating microscope from the common digital arterial level to the distal part of the distal interphalangeal (DIP) joint. Local compression was not seen at any level, including the lumbrical canal and around the PIP and DIP joints, indicating that neither the Grayson nor the Cleland ligaments were the cause. After tourniquet release, arterial flow in the index ulnar digital artery was not detected from the midproximal phalanx level to just proximal to the DIP joint (Figure 3). In addition, the artery at this portion was harder and felt like a stick rather than a tube. Transection of the artery revealed complete occlusion with fibrous tissue inside (Figure 4). After total resection of this occluded artery (from the midproximal phalanx level to just proximal to the DIP joint), arterial flow from the proximal stump was still poor. Adventitial stripping from the distal portion of the common digital artery to the proximal stump was performed microscopically, and flow was better but pulseless. A vein graft harvested from the volar side of the distal forearm was used. The patency test showed flow within the graft; however, it was still pulseless and lacked normal tension. After the addition of complete adventitial stripping from the distal portion of the common digital artery to the distal portion of the DIP joint of the radial digital artery, the artery was expanded and showed normal pulsation. The color of the fingertip of the index finger returned to pink. The color of the middle fingertip was still pale, and adventitial stripping using the same method as for the radial digital artery worked well, with the color of the middle fingertip returning to pink. After surgery, the patient took oral 20 mg aspirin and 15 μg prostaglandin E1 for 1 month.

Intraoperative findings of case 1. Flow in the ulnar digital artery of the right index finger is interrupted proximal to the proximal interphalangeal (PIP) joint (arrow). *PIP joint.
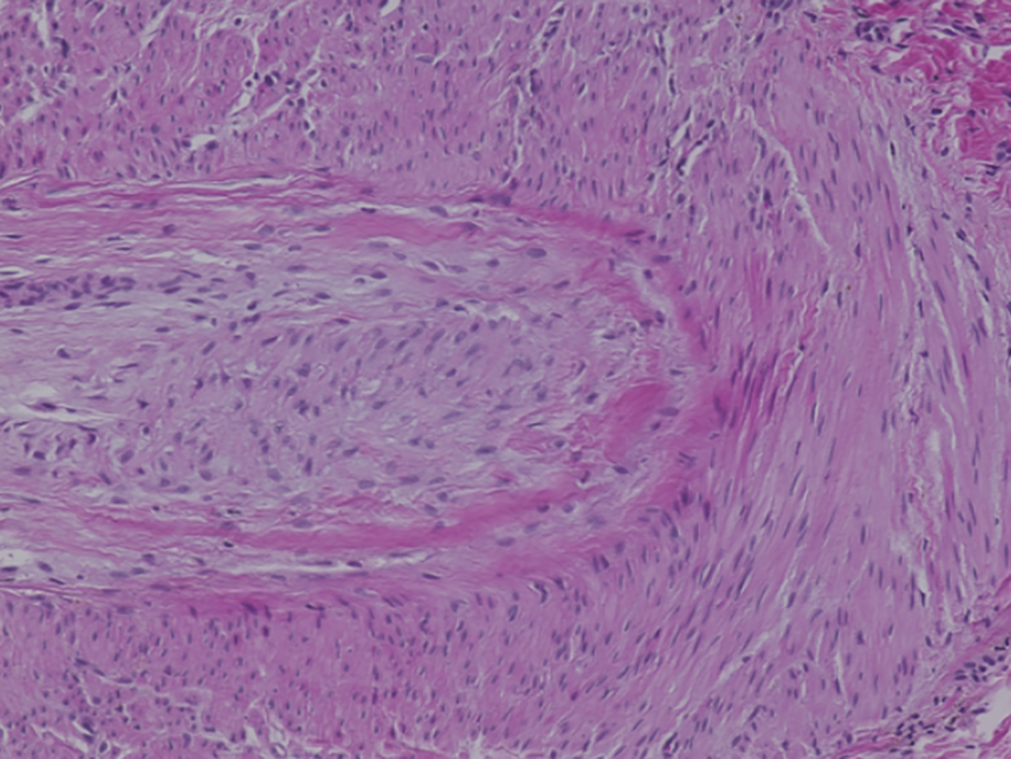
Pathological findings of case 1. The artery is completely filled with fibrous tissue.
For 2 weeks after surgery, a volar splint from the forearm to the fingertip of the index and middle fingers was applied to facilitate healing of the vein graft, and the patient started to move the involved fingers without any limit and to throw a ball gently at 1 month postoperatively. At 6 months after surgery, he was able to pitch in the national major league without any complaints, and an ultrasonographic examination revealed enough blood flow in the index radial digital artery and fingertip (Figure 1C). He has been the closer of the baseball team for 5 years after surgery.
Case 2
A 20-year-old left-handed high-level amateur pitcher (draft candidate) complained of sudden coldness and pain in his left middle finger, and he had been unable to pitch 2 weeks before the initial visit to our clinic. He had been a baseball pitcher for 10 years. At the first visit, his middle finger appeared completely pale and cold during palpation. He had a long-standing blood blister on the radial side of the middle fingertip (Figure 5), and refill of the fingertip was quite slow. Thermography revealed coldness of the finger (Figure 6A). An ultrasonographic examination of the middle finger showed no flow in the radial digital artery from the level of the metacarpophalangeal joint (Figure 7A) as well as spotty and poor flow in the ulnar digital artery (Figure 7B). In addition, flow was not detected in the fingertip (Figure 7C). Computed tomography angiography revealed no arterial lesion from the level of the subclavian to the wrist. We suspected the same condition as seen in case 1, and a surgical intervention was selected. The patient did not have a history of any systemic disease or smoking.

Photograph of case 2 at the initial visit. The fingertip of the left middle finger is pale, and there is a long-standing blood blister on the radial side.

Thermogram of case 2. (A) The preoperative skin temperature of the middle finger is quite low. (B) The postoperative 8-week skin temperature is normal.
Ultrasonogram of case 2 (left: proximal). (A-C) The left middle finger before surgery and (D-F) 8 weeks after surgery. (A) Arterial flow in the radial digital artery around the proximal interphalangeal (PIP) joint is not detected preoperatively, (D) but it is confirmed after thrombectomy and adventitial stripping. (B) Arterial flow in the ulnar digital artery is spotty and insufficient preoperatively, (E) but it is adequate after adventitial stripping. (C) No flow in the fingertip is detected preoperatively, (F) but flow is sufficient postoperatively. *PIP joint.
The digital arteries of the middle finger were exposed in the same fashion as case 1 under the operating microscope. Flow in the radial digital artery was not detected, and a mobile mass in the artery at the proximal level of the PIP joint and softening of the digital artery were seen during palpitation at the level of the PIP joint (Figure 8A). The mobile mass was resected after partial transection of the artery (Figure 8B), and a pathological examination revealed a red (distal) and white (proximal) thrombus (Figure 9). Arterial flow was still poor just after resection of the mass, and after total adventitial stripping similar to case 1, blood flow in the involved artery recovered sufficiently, and closure of the transection site was performed microsurgically. Additionally, complete adventitial stripping of the ulnar digital artery was performed, and the color of the middle fingertip returned to pink. After surgery, similar to case 1, the patient took oral aspirin and prostaglandin E1 for 1 month.

Intraoperative findings of case 2. (A) There is a mobile mass (arrow) in the radial digital artery of the left middle finger just proximal to the proximal interphalangeal joint, and flow is interrupted just proximal to this mass. (B) The mass is a thrombus (arrow) and is resected.

Pathological findings of case 2 (top: distal). The mass consists of red cells (top) and fibrous tissue (bottom).
At 1 month after surgery, the skin temperature remained normal (Figure 6B), and the patient started throwing a ball. Ultrasonography revealed sufficient arterial flow in the involved digital arteries and fingertip (Figure 7, D-F). He was able to return to the game at 3 months postoperatively. At 1 year after surgery, he had no symptoms in the involved digit.
Discussion
In both cases presented, we found a digital arterial lesion around the PIP joint in the index or middle finger without any compressive abnormality, and we were able to successfully treat them surgically with thrombus resection and total adventitial stripping around the involved artery. Although ultrasonography showed spotty and insufficient blood flow in the artery treated with a vein graft after surgery, these patients were able to return to playing baseball as pitchers at the same competitive level.
This kind of digital arterial lesion has not been reported previously in the English-language literature. The only report about digital arterial injuries in the hands of baseball pitchers was described by Itoh et al. 8 Those authors were able to successfully treat their cases with release of the Cleland ligament around the PIP joint on both sides of the fingers or the lumbrical canal. However, in our 2 cases, we could not find any local compressive lesions along the digital arteries from the lumbrical canal to the distal portion of the DIP joint. We found complete occlusion of the digital arteries around the PIP joint with a thrombus or occlusive fibrous tissue.
The results of a kinematic study 17 revealed that the metacarpophalangeal and PIP joints of the middle and index fingers flex and then extend rapidly until ball release during the acceleration phase of the pitching motion. Kinoshita et al 10 demonstrated 2 peaks of resultant forces in the index and middle fingers, before (1) maximum rotation of the shoulder joint and (2) ball release. In other words, baseball pitchers grip the ball and force strong finger extension repeatedly within a short time. Anatomically, the digital artery is fixed between the Cleland ligament and Grayson ligament. The high-speed repetition of the pitching motion and the anatomic location of the digital artery may cause pathological changes in the digital arteries and irreversible circulatory disturbances around the PIP joint. In fact, softening of the artery around the PIP joint, which may represent traumatic changes in the inner and middle layers leading to thrombus formation, was palpable in case 2.
The diagnosis for this condition is as follows. Patients usually present with cool, pale, and painful index or middle fingers. They sometimes have a long-standing blood blister without normal healing on the involved digit. For the assessment of distal arterial patency, the digital Allen test should be performed. Digital subtraction angiography may be the gold standard for the assessment of vascular disorders in the area of the hand as well as the regions proximal to the hand. However, it is an invasive procedure, and we only performed it in case 1.
Although an ultrasonographic examination is technically demanding, it is very useful for the assessment of limited areas. In our 2 cases, it revealed digital arterial occlusion and poor circulation of the involved fingertips. Additionally, ultrasound can be used for the assessment of arterial flow postoperatively. However, in our cases, it did not identify the thrombus in the digital artery.
Because of the rarity of the condition, uniform treatment options have not yet been established. Similarly, effective nonoperative treatment for this condition has not been described, and from our minimal experience, medications such as antithrombin agents, heparin, and prostaglandins are not effective in these advanced cases. However, if presymptomatic patients can be detected by an ultrasonographic examination, these medications may have the potential to prevent the progression of this lesion. The other option is intra-arterial thrombolysis; however, its benefits are limited and unclear, 7 and it might not be indicated for a white thrombus and complete occlusion with fibrous tissue, as seen in our cases.
Surgical treatment options include thrombectomy, revascularization with or without a vein graft, and digital sympathectomy, meaning adventitial stripping. In case 1, we reconstructed the occlusive artery with a vein graft, but it did not work sufficiently because of poor outflow from the proximal stump. In case 2, we were able to successfully resect the thrombus, but arterial flow was still poor. Thus, we performed periarterial sympathectomy, including complete circumferential stripping of the adventitia from the distal common digital artery to the distal portion of the DIP joint under the operating microscope. After the procedure, arterial flow recovered, and the fingertip color returned to pink.
Periarterial sympathectomy for the treatment of digital ischemia was initially described by Flatt 4 and subsequently modified by Wilgis 18 and Koman et al, 11 and it has become standardized in patients with primary vasospastic disease involving a single digit. 6 Adventitial stripping is usually performed for the prevention or treatment of vasospasm and for vasodilation in the microvascular surgery setting. From an ex vivo study using the radial artery harvested during cardiovascular reconstruction, it was proven that the adventitial dissected radial artery was less susceptible to vasoconstriction and more prone to vasorelaxation and showed increased free blood flow. 13 Adventitial stripping should be performed under a surgical microscope to prevent perforation of the digital artery and to improve the quality of sympathectomy while preserving important small arterial branches. Although we could not ascertain the optimal length of stripping, total stripping from the distal common digital artery to the distal portion of the DIP joint was sufficient to re-establish flow in our cases. Although the follow-up period of one of our cases was only 1 year, midterm results were promising in the literature. 4,18 The complications of this procedure reported in the literature are hypoesthesia of the fingertip and delayed healing of the surgical wound, but all of them can be treated nonoperatively. 2
Competitive baseball pitchers are at risk for hematogenous disorders of the fingers. These disorders may be asymptomatic at first but then may lead to pathological changes including digital arterial occlusion with a thrombus, progressing to complete fibrous occlusion. Physicians should be aware of this clinical condition, and when faced with hand ischemia in baseball players, an arterial evaluation from the shoulder to the finger should be considered. An ultrasonographic examination is recommended for the evaluation of distal-level arterial flow. If complete occlusion is revealed, a revascularization procedure including thrombectomy or vein grafting should be performed, and when flow is not sufficient, adventitial stripping may be indicated.
Footnotes
Final revision submitted February 16, 2020; accepted March 13, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.