
Abstract
Background:
Arthroscopic Bankart repair (ABR) and the Latarjet procedure are surgical techniques commonly used to treat anterior shoulder instability. There is no consensus among shoulder surgeons regarding the indications for choosing one over the other.
Purpose:
To compare the results of the Latarjet procedure with those of ABR for the treatment of anterior shoulder instability.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data on all patients who were treated surgically for recurrent anterior shoulder instability between 2006 and 2011 were retrospectively collected at 4 medical centers. The minimum follow-up was 5 years. Data were retrieved from medical charts, and patients were interviewed to assess their level of satisfaction (range, 0-100), functional outcomes (using the American Shoulder and Elbow Surgeons shoulder score; the Subjective Shoulder Value; and the Disabilities of the Arm, Shoulder and Hand score), and quality of life (using the 12-Item Short Form Health Survey [SF-12]). Information on return to sports activities and postoperative level of activity compared with that of the preinjury state, complications, reoperations, and recurrent instability were recorded and evaluated.
Results:
A total of 242 patients were included. The Latarjet procedure was performed in 27 shoulders, and ABR was performed in 215 shoulders. Patients in the ABR group had significantly higher rates of redislocation (18.5%; P = .05) and subluxation (21.4%; P = .43) but a lower rate of self-reported apprehension (43.0%; P = .05) compared with patients in the Latarjet group (3.7%, 14.8%, and 63.0%, respectively). There were 5 patients in the ABR group who underwent reoperation with the Latarjet procedure because of recurrent instability. The functional scores in the Latarjet group were better than those in the ABR group. The SF-12 physical score was significantly better in the Latarjet group than in the ABR group (98.1 vs 93.9, respectively; P = .01). Patient satisfaction and subjective scores were similar in both groups.
Conclusion:
These results support recently published data on the Latarjet procedure that showed its superiority over ABR in midterm stability (dislocations or subluxations). The contribution of self-reported apprehension to the broad definition of stability is not clear, and apprehension rates were not correlated with satisfaction scores or the recurrence of dislocation or subluxation.
Glenohumeral joint (GHJ) instability mostly affects young adults and has a variety of presentations. 10 Shoulder instability has traditionally been divided into multidirectional nontraumatic and unidirectional traumatic, with the former often treated nonoperatively and the latter, surgically. 4,6,14 Patients who present with anterior shoulder instability report recurrent dislocation or subluxation, limited function, reduced athletic performance, and decreased quality of life. 4,6,14 Surgical treatment for GHJ instability falls into 2 main categories. The first, anatomic repair, includes labral repair, capsular shift, and remplissage to treat large Hill-Sachs lesions. The second, the Latarjet procedure, was originally intended to address large bony defects of the glenoid fossa, and it has gained popularity for that and other indications as well. 13
The results of surgical treatment for anterior shoulder instability are satisfactory on the whole, 4,14 with recurrence rates reported between 0% and 40%, 4 although many of those studies reported only a short-term follow-up (ie, 2 years) 11,14 and were either not controlled or examined different surgical techniques. 7,20 The factors affecting the results of surgical treatment are numerous, and they include the patient’s age, type and level of physical activity, size and severity of bony and soft tissue lesions, surgical technique, and laxity. 1,4
There is no consensus among shoulder surgeons regarding the indications for the Latarjet procedure in preference to other techniques in patients without significant bone loss. Only a few studies have compared its long-term results with those of arthroscopic Bankart repair (ABR). 12,14 Zimmermann et al 22 recently evaluated their results with at least 6 years of follow-up and reported significant advantage of the Latarjet procedure compared with ABR. The overall instability rates, including dislocation, subluxation, and self-reported apprehension, were dramatically in favor of the Latarjet procedure. These authors concluded that the Latarjet procedure is superior to ABR and that the results tend to further differ in favor of the former as follow-up time increases. Nevertheless, the Latarjet procedure was reported to have a high complication rate. 19
The aim of this multicenter study was to compare the results of the Latarjet procedure with those of ABR for the treatment of anterior shoulder instability. Our hypothesis was that there would be no differences in terms of recurrence or functional outcomes.
Methods
After approval from the institutional ethics committee, a retrospective data search was conducted at 4 medical centers. Inclusion criteria were primary surgical treatment (ABR or Latarjet) for anterior GHJ instability between 2006 and 2011, age younger than 40 years at the time of surgery, and a minimum follow-up of 5 years. Patients who had undergone previous shoulder surgery or had sustained other injuries in the affected shoulder (eg, a superior labral anterior-posterior lesion, rotator cuff tear, cartilage defect, humeral avulsion of the glenohumeral ligament, voluntary dislocation, and multidirectional instability) were excluded.
Data were collected by orthopaedic residents from medical charts, and the study patients were interviewed to assess their level of satisfaction (range, 0-100), functional outcomes (using the American Shoulder and Elbow Surgeons [ASES] shoulder score; the Subjective Shoulder Value [SSV]; and the Disabilities of the Arm, Shoulder and Hand [DASH] score), and quality of life (using the 12-Item Short Form Health Survey [SF-12]). Their responses to questions on return to sports activities and postoperative levels of sports activities compared with preinjury functioning, complications associated with the surgical procedure, reoperations, and recurrent level of instability were evaluated by independent reviewers.
Recurrent instability was defined by the same criteria as those of Zimmermann et al 22 : “redislocation” referred to a dislocation that required reduction by a medical professional; “subluxation” referred to a subjective sensation of slipping or shifting of the GHJ, followed by spontaneous reduction or manual resetting by the patient; and “functional apprehension” referred to the patient’s concern that the humeral head would come out of the joint when the arm was in the throwing position (abduction-external rotation).
All operative procedures were performed by fellowship-trained shoulder specialists. The Latarjet procedure was performed according to the original technique as described in detail elsewhere. 13,21 ABR was performed arthroscopically with the patient in either a beach-chair or lateral decubitus position, similar to the technique described by Zimmermann et al 22 or as previously described by Maman et al 14 and Chechik et al, 8 with or without arthroscopic rotator interval closure. The decision to perform the Latarjet procedure was made according to a preoperative assessment of glenoid bone loss or the size of the Hill-Sachs lesion as measured using computerized tomography or magnetic resonance arthrography. The Latarjet procedure was also performed if glenoid loss was ≥15% or humeral bone loss was ≥30% to 40%. 3,6
Statistical Analysis
Comparisons of the demographic and clinical variables were made using the Student t test and Mann-Whitney nonparametric test for continuous parameters and the chi-square test or Fisher exact test for categorical parameters. Statistical analysis was carried out using SPSS for Windows software (version 22.0; IBM Corp), and significance was set at P ≤ .05.
Results
Of the 538 patients who underwent surgical treatment for anterior shoulder instability, 296 were lost to follow-up, did not meet the inclusion criteria, or declined to participate in this study, leaving 242 (45.0%) patients in the cohort, of whom 27 underwent the Latarjet procedure and 215 underwent ABR. Specific details on mean age at surgery, sex, involved arm, dominant arm, type of surgery, age at first dislocation, and dislocation of the contralateral shoulder are presented in Table 1. Patients in the ABR group were significantly younger than those in the Latarjet group (24.9 vs 29.2 years, respectively; P = .0008). The mean follow-up was 7.8 years, with a range of 5.0 to 12.8 years. A bony Bankart lesion was the main recorded indication for performing a primary Latarjet procedure, and it was recorded in 76% of the 27 patients.
Patient Characteristics a
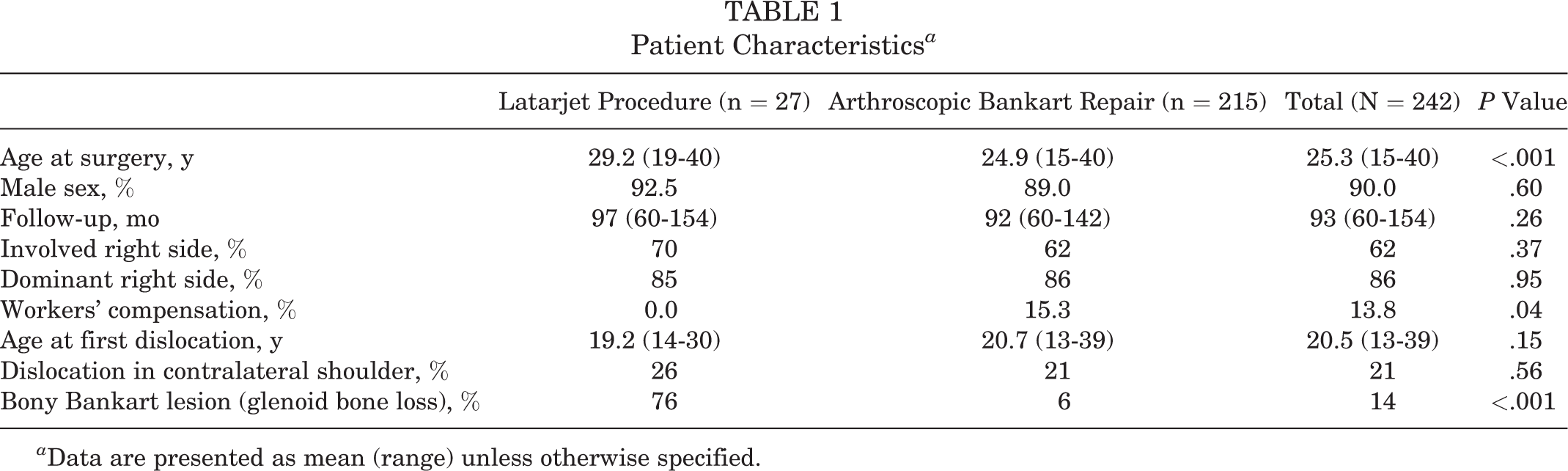
a Data are presented as mean (range) unless otherwise specified.
Patients in the ABR group had a significantly higher redislocation rate (18.5%) and higher rate of reported subluxation (21.4%) but had a lower rate of apprehension (43.0%) compared with rates in patients in the Latarjet group (3.7%, 14.8%, and 63.0%, respectively) (P = .05, P = .43, and P = .05, respectively) (Figure 1). There were 5 patients in the ABR group who underwent reoperation with the Latarjet procedure because of recurrent instability.

Residual instability and return to sports at final follow-up (range, 5.0-12.8 years). ABR, arthroscopic Bankart repair. Asterisk indicates statistically significant differences (P < .05).
Functional scores in the Latarjet group were better than those in the ABR group; the Latarjet group showed a nearly significant advantage in the mean ASES score (91.2 vs 86.0, respectively; P = .051) and significant differences in factors, such as lifting weights, throwing a ball, and sports activity (P = .004, .007, and .01, respectively) (Figure 2). Pain levels were similar in both the ABR and the Latarjet groups (1.8 vs 1.3, respectively; P = .18).

Functional results at final follow-up (range, 5.0-12.8 years). ABR, arthroscopic Bankart repair; ASES, American Shoulder and Elbow Surgeons; SF12, 12-Item Short Form Health Survey; SSV, Subjective Shoulder Value. Asterisk indicates statistically significant differences (P < .05).
The mean SF-12 physical score was significantly better in the Latarjet group compared with the ABR group (98.1 vs 93.9, respectively; P = .01). The mean DASH score was better in the Latarjet group as well (4.5 vs 6.2, respectively; P = .31). Patient satisfaction and other subjective scores were similar in both groups (Figure 3). The mean satisfaction score for the Latarjet group was 8.4 of 10: overall, 17 of 27 (63.0%) patients ranked their satisfaction as ≥8, and only 3 of 27 (11.1%) scored their satisfaction as ≤5. The ABR group’s mean satisfaction score was 7.7 of 10: overall, 131 of 215 (60.9%) had a score of ≥8, and 9 of 215 (4.2%) had a score of ≤5. The mean SSV score was 81.5 (range, 40-100) in the Latarjet group compared with 84.8 (range, 20-100) in the ABR group (Figure 2).

Patient satisfaction and functional results at final follow-up (range, 5.0-12.8 years). ABR, arthroscopic Bankart repair; DASH, Disabilities of the Arm, Shoulder and Hand.
Subgroup analysis was performed for patients aged <25 years and patients aged ≥25 years. In the case of patients aged <25 years, no statistically significant differences were found between groups in terms of age (mean, 21.5 years [range, 19-24 years] for Latarjet vs 20.5 years [range, 15-24 years] for ABR), sex, and dominant arm. Patients in the Latarjet group scored lower than the ABR group for the SF-12 mental score (mean, 87 [range, 57-100] vs 88 [range, 53-100], respectively) but had similar functional scores: SSV, 83 (range, 60-100) versus 86 (range, 30-100), respectively; ASES, 89 (range, 60-95) versus 87 (range, 50-100), respectively; and DASH, 5.8 (range, 0-28) versus 6.0 (range, 0-39), respectively. The instability rates in the Latarjet group were 0% for dislocation, 13% for subluxation, and 63% for apprehension (self-reported) compared with 22% for dislocation, 26% for subluxation, and 46% for apprehension in the ABR group.
In patients aged ≥25 years, the Latarjet group was still older than the ABR group (mean age, 32 years [range, 25-40 years] vs 30 years [range, 25-40 years], respectively), with no differences in other demographic variables (sex, dominant arm). Patients in the Latarjet group had a higher SF-12 mental score compared with that of the ABR group (mean, 93 [range, 79-100] vs 85 [range, 18-100], respectively) but had similar functional scores: SSV, 81 (range, 40-100) versus 84 (range, 20-100), respectively; ASES, 92 (range, 57-100) versus 84 (range, 32-100), respectively; and DASH, 4.0 (range, 0-19) versus 6.5 (range, 0-65), respectively. The instability rates in the Latarjet group were 5% for dislocation, 16% for subluxation, and 63% for apprehension (self-reported) compared with 14% for dislocation, 16% for subluxation, and 39% for apprehension in the ABR group.
There were 7 major complications in the ABR group, including 2 neurological injuries, 2 infections, 2 cases of chronic pain, and 1 case of a postoperative tendon tear that required rotator cuff repair. No major complications were recorded for the patients in the Latarjet group; 1 patient required screw removal, which did not affect his final SSV score of 95 and satisfaction score of 10 of 10.
Discussion
The aim of this study was to compare the results of the primary Latarjet procedure and ABR for the treatment of anterior shoulder instability. The Latarjet procedure has often been performed in cases of significant bone loss or failed labral repair, and it proved to provide excellent results in terms of shoulder stability and function. 9,12 Therefore, a primary Latarjet procedure is currently considered even in cases without significant bone loss. Better understanding of the factors that influence the results (eg, young age, large Hill-Sachs lesion, hyperlaxity, and engagement in contact sports) led to the use of the instability severity index score 1 as a predicting tool 16 and a means to broaden the indications for this procedure.
Previous publications 8,14 have examined the results of ABR and revealed a recurrent instability rate of 15% to 20%. However, the minimum follow-up was only 2 years (range, 2-5.6 years), and the definition of instability included only dislocation or subluxation. A recent study by Zimmermann et al 22 reported significantly inferior long-term outcomes of ABR compared with those of the Latarjet procedure. The current multicenter study was designed to compare the results of the Latarjet procedure with those of ABR for the treatment of anterior shoulder instability. Furthermore, because the parameter of self-reported apprehension had such a significant effect on their results, we evaluated its significance. We chose essentially the same inclusion and exclusion criteria as those used by Zimmermann et al, and both studies are similar for the definitions of “instability” and types of procedures (ABR and Latarjet).
The Latarjet procedure showed favorable stability (dislocation and subluxation) compared with that of ABR for redislocation (3.7% vs 18.5%, respectively; P = .05) and subluxation (14.8% vs 21.4%, respectively; P = .43), similar to the findings of Zimmermann et al 22 (1% vs 13%, respectively, for redislocation and 2% vs 15%, respectively, for subluxation) and those of Bessiere et al 2 (minimum follow-up of 4 years; recurrent instability of 10% [9/93] in the Latarjet group compared with 22% [20/93] in the ABR group).
The main differences between the study groups were younger age in the ABR group (24.9 vs 29.2 years, respectively) and a higher rate of significant glenoid bone loss in the Latarjet group (6% vs 76%, respectively). Both factors were previously found to be related to high failure and recurrence rates. 22 It had been shown before by Boileau et al 4 that significant glenoid bone loss is an indication for the Latarjet procedure. The results of this study support this notion, as the recurrent instability rates after the Latarjet procedure were low, despite bone loss. Young age alone is not considered an indication for the Latarjet procedure, and the results of this study do not allow a conclusion regarding this matter.
However, the rates of self-reported apprehension in this study are significantly higher (63.0% for Latarjet and 43.0% for ABR) than those previously reported by Zimmermann et al 22 (9% for Latarjet and 29% for ABR). Because all other outcomes besides apprehension are comparable with those in previous studies, we speculate that apprehension reported by patients was often not necessarily a sign of instability. Patients may feel discomfort in the throwing position because of adhesion and anterior capsule tightness and thus report positive apprehension.
Traditionally, an apprehension test is used to assess anterior instability. The real value of the patient’s level of apprehension as a predictive sign for instability is not clear. Safran et al 18 concluded that it can categorize patients into groups at a higher and lower risk for recurrent dislocation after a first traumatic shoulder dislocation, with a sensitivity and specificity of 41.7% and 85.7%, respectively. The value of a positive apprehension test result after instability repair is even more obscure. The findings of Zimmermann et al 22 suggest that the presence of postoperative apprehension may be indicative of surgical failure. According to these authors, the apprehension rate was 29% in the ABR group compared with 9% in the Latarjet group (P < .001), which was correlated with a higher percentage of dissatisfied patients in the former group compared with the latter group (13.2% vs 3.2%, respectively; P = .007). They stated that most studies did not use this broad definition and that the transition from apprehension to subluxation may not always be perfectly clear.
The current study showed no correlation between positive apprehension (63.0% for Latarjet vs 43.0% for ABR) and satisfaction scores (8.4 vs 7.7, respectively; P = .18). Bessiere et al 2 also could not find any correlation between positive apprehension (23% in the Latarjet group vs 19% in the ABR group) and the rate of satisfaction with surgery (91% vs 88%, respectively; P = .47). This inconsistency between self-reported apprehension in the operated arm and the patient’s satisfaction with the procedure was further demonstrated by Hovelius et al. 12 After a follow-up of 15 to 17 years, the rate of apprehension was 0% among the patients in the ABR group compared with 27% among the patients in the Latarjet group, and satisfaction rates were 92% and 97%, respectively. We assume that self-reported apprehension may represent a patient’s discomfort (may be caused by the sling effect and tightness of the subscapularis) rather than instability in the throwing position.
Because the Latarjet procedure is a nonanatomic technique, one may assume that there might be a higher complication rate either in the short or long term, as suggested in various reports. 5,15 Bokshan et al 5 found that the Latarjet procedure had a significantly higher 30-day complication rate of 5.5% compared with 1% for open Bankart repair and 0.6% for ABR. The same was shown by Rollick et al 17 for long-term complications, with a 9.4% complication rate for the Latarjet group and 0% for the ABR group. The complication rate in this study was similar for both groups: 3.3% (7/215) in the ABR group and 3.7% (1/27) in the Latarjet group. These values are within the ranges reported in previous publications (5.5%-9.4% for the Latarjet group and 0%-2.96% for the ABR group). 5,15,17,22
The limitations of this study are those inherent to its retrospective design, the significantly younger age of the ABR group, the relatively small number of patients in the Latarjet group, and the higher risk for failure in the Latarjet group because of a deficient glenoid or humerus. While its being a multicenter study enabled us to recruit a large number of patients in the collective cohort, it also combined the operative outcomes of a number of surgeons with different experience, operative techniques, and decision-making considerations. Additional limitations of this study include the following: this study was not randomized, sports activity or return to sports was not recorded, and no follow-up imaging was performed.
Conclusion
The Latarjet procedure as a primary treatment for anterior shoulder instability showed very good results in terms of recurrent instability, functional outcomes, and patient satisfaction. Recurrent instability after the Latarjet procedure was lower compared with that after ABR. However, self-reported apprehension after the Latarjet procedure was very common without compromising functional results or patient satisfaction.
Footnotes
Final revision submitted April 28, 2020; accepted May 12, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Tel Aviv Sourasky Medical Center (protocol No. 0525-15-TLV).