
Abstract
Background:
While knees with meniscal tears are associated with a heightened risk of developing osteoarthritis (OA), it is difficult to predict which patients are at the greatest risk for OA. Gene signatures in menisci that are resected during arthroscopic partial meniscectomy (APM) may provide insight into the risk of OA progression.
Hypothesis:
Meniscal gene signatures at the time of APM will predict radiographic OA progression.
Study Design:
Case series; Level of evidence, 4.
Methods:
Meniscal fragments were collected from 38 patients without OA during clinically indicated APM of the medial meniscus. The expression of 28 candidate genes with known roles in cartilage homeostasis, OA, extracellular matrix degradation, and obesity was assessed by quantitative real-time polymerase chain reaction. Weightbearing radiographs obtained before surgery and at final follow-up were graded by a musculoskeletal radiologist using the Kellgren-Lawrence classification of OA. The association of meniscal gene expression at baseline with the progression of radiographic OA was determined.
Results:
Gene expression and baseline and follow-up radiographic data were available from 31 patients (81.6%) at a mean follow-up of 6.2 ± 1.3 years. Patients without OA progression had significantly higher expression of 7 genes: MMP9 (5.1-fold; P = .002), IL8 (2.9-fold; P = .016), CCL3 (3.7-fold; P = .032), CCL3L1 (4.5-fold; P = .008), CXCL6 (6.2-fold; P = .010), LEP (5.2-fold; P = .004), and RETN (46-fold; P = .008).
Conclusion:
Gene expression in the meniscus at the time of APM may be associated with the risk for progression of OA after surgery. Elevated expression of the aforementioned genes may reflect a chondroprotective response. Stratifying the risk for OA progression after APM could facilitate targeted interventions to delay or prevent the development of OA. Further studies in a larger cohort with an extended follow-up, and inclusion of additional genes, are warranted to better characterize this association.
Osteoarthritis (OA) is the most common degenerative joint disorder, resulting in disability and financial burden in the United States and around the world. 40 One reason for its high prevalence may be a lack of information regarding the early molecular events that initiate the disease process. Currently, knee OA is diagnosed in its late stages by radiographs reflecting significant articular cartilage loss, at which time little can be done to delay, halt, or reverse its progression. Oftentimes, total knee arthroplasty (TKA) is the only effective treatment. Interventions at earlier stages may be able to delay or even prevent OA progression such that joint replacement could be delayed or avoided. Meniscal degeneration is highly prevalent in patients with OA. 14,37 However, it is not currently possible to predict which patients with meniscal tears are at the highest risk for developing OA that may require joint replacement, nor is it possible to predict the timeline for OA progression in these patients. While meniscal tears are known to lead to OA in 30% to 75% of patients, 8,19,21,25 few studies have explored how the biology of the injured meniscus relates to OA pathogenesis, 2,3,30,31,35,37 making it difficult to stratify the risk of progression.
Arthroscopic partial meniscectomy (APM) is an effective treatment for symptomatic meniscal tears, but it does not slow OA progression. 6,8,10,19,21 After surgery, patients often recover within several months. Other than some physical therapy, patients often receive little or no additional interventions unless the knee continues to be symptomatic or develops new symptoms. However, many of these patients still develop OA, as the meniscal injury itself may initiate a cascade of changes within the knee or reflects pre-existing changes in the joint that lead to OA. 2,8,19,21,37 Injured meniscal tissue that is debrided at the time of surgery is generally disposed of, but it is possible that this readily available tissue contains information that may provide insight into each individual patient’s risk of OA progression. Developing more sensitive and specific means to determine a patient’s risk for OA progression could facilitate targeted interventions to slow or stop the progression of OA. This could shift the paradigm of treatment for knee OA after a meniscal injury from end-stage reactive treatment with injections and TKA to earlier proactive efforts to slow or stop the disease process using known and yet-to-be discovered interventions.
Previous studies have suggested that OA development is associated with gene expression levels of cytokines, chemokines, matrix metalloproteinases, aggrecanases, and other inflammation-related genes within the meniscus of noninjured knees, 26,41 at the time of APM in the setting of meniscal injuries, 2,3,27,28,30,31 and at the time of TKA in knees with end-stage OA. 35,37 However, no study has investigated the association of gene expression in the injured medial meniscus at the time of APM with the progression of OA. The objective of this study was to investigate the radiographic outcomes of a cohort of patients who previously underwent arthroscopic partial medial meniscectomy and their association with gene expression data available from meniscal samples collected at the time of surgery. 2,3 The study hypothesis was that differential expression of OA-related genes will be associated with the progression of knee OA in patients with medial meniscal injuries treated with APM.
Methods
The study site’s institutional review board approved this protocol. Meniscal fragments were collected at the time of clinically indicated APM for isolated medial meniscal tears from 38 consenting patients meeting inclusion criteria, and gene expression was characterized by quantitative real-time polymerase chain reaction as previously described. 2,3,30 Custom-designed primers 2,3,30 were obtained from Invitrogen for a panel of 28 candidate genes based on their known role in cartilage homeostasis, OA, and extracellular matrix degradation 2,30 as well as selected markers for obesity 28,29 including adiponectin (ADIPOQ), apelin (APLN), leptin (LEP), 11 and resistin (RETN). 24 Briefly, we evaluated the expression of proinflammatory cytokines IL-1α, IL-1β, IL-6, and TNFα 2 as well as chemokines IL-8, CCL3, CCL3L1, CXCL1, CXCL6, and CCL20. The expression of matrix-degrading enzymes ADAMTS4, ADAMTS5, MMP-1, MMP-3, MMP-9, and MMP-13 was assessed. Matrix molecules BMP-2, COL1A1, COL2A1, and ACAN as well as transcription factors NFκB2, NFκBIA, and IκBA were also evaluated.
All patients underwent a single series of knee radiographs (standing anteroposterior, Rosenberg, lateral, and Merchant views) at the time of the initial preoperative clinic visit and at final follow-up. Baseline age, sex, and body mass index (BMI) were collected and recorded. A single academic musculoskeletal radiologist who was blinded to gene expression data (M.V.F.) graded the preoperative and final follow-up radiographs according to the Kellgren-Lawrence classification of OA. 7,17 The modified Kellgren-Lawrence classification allows for patients to be dichotomized as having “incident OA,” defined as joint space narrowing and an osteophyte, with at least 1 of these being new or “no incident OA.” 7 Radiographic progression was quantified as an increase by at least 1 Kellgren-Lawrence grade within a compartment. Patients with rapid progression were those who had incident OA as defined above. 7,17
We compared patients without OA progression in any compartment of the knee to those with progression in any compartment of the knee, patients without any progression in the medial compartment to those with progression in the medial compartment, and patients without rapid progression in the medial compartment to those with rapid progression in the medial compartment. Finally, we compared the entire cohort between those with no progression in the knee, those with progression but not in the medial compartment, those with some progression but not rapid progression in the medial compartment, and those with rapid progression in the medial compartment. No patients had rapid progression in the lateral and/or patellofemoral compartments without also having rapid progression in the medial compartment.
Statistical Analysis
Based on previous studies reporting that approximately 36% of patients are expected to demonstrate radiographic progression of OA at 5 years after APM, 22,33 an a priori power calculation with an effect size of 0.5, alpha of .05, and power of 0.8 was performed and demonstrated a required minimum sample size of 26 patients. Quantitative real-time polymerase chain reaction data were analyzed using the 2 –ΔΔCT method. 36 For each gene in the analysis, normalized fold changes (2–(target gene C T – housekeeping gene C T )) in patients showing no radiographic progression of OA were averaged and treated as controls. The normalized fold changes of patients with progression of OA were averaged and compared with controls using a t test, setting the level of significance to .05. Fold change was calculated by dividing the OA average by the control average. When patients with OA were separated into groups by severity, analysis of variance, followed by a Tukey post hoc pairwise comparison, was performed. Analyses were performed in SPSS (Version 25; IBM).
Results
Follow-up radiographs were obtained on 31 of the initial 38 patients (81.6%) at a mean follow-up of 6.2 ± 1.3 years (Table 1). At the time of APM, the cohort had a mean age of 48.5 ± 9.2 years and a mean BMI of 28.1 ± 5.1 kg/m2, with 45.2% being female.
Characteristics of Study Patients a
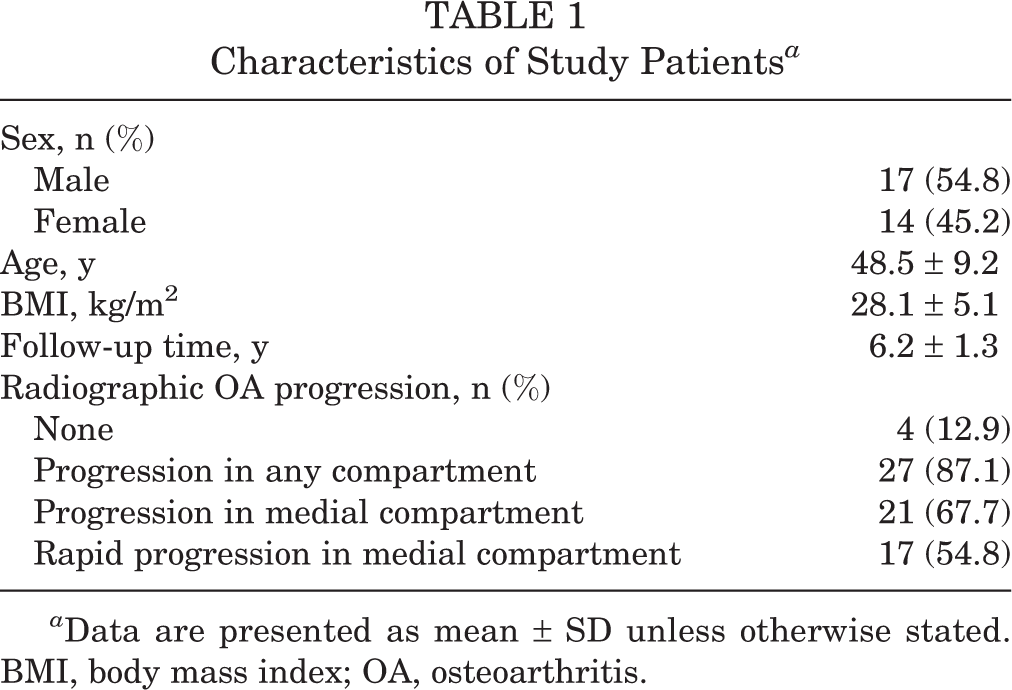
a Data are presented as mean ± SD unless otherwise stated. BMI, body mass index; OA, osteoarthritis.
Patients with a progression of radiographic OA had significantly lower expression of 7 genes (Figure 1). Specifically, there was a 5.1-fold decrease in MMP9 (P = .002), 2.9-fold decrease in IL8 (P = .016), 3.7-fold decrease in CCL3 (P = .032), 4.5-fold decrease in CCL3L1 (P = .008), 6.2-fold decrease in CXCL6 (P = .010), 5.2-fold decrease in LEP (P = .004), and 46-fold decrease in RETN (P = .008). None of the other candidate genes tested reached formal significance (Table 2).

Gene transcripts differentially expressed between patients who showed radiographic osteoarthritis (OA) progression at follow-up (“Some”) and those who did not (“No”).
Normalized Expression of All Candidate Genes Tested a

a Data are presented as mean ± SEM. P values in bold represent statistically significant differences, OA, osteoarthritis.
When segregating patients based on the severity of OA progression, there was significantly increased expression of 3 genes among patients without any radiographic OA progression (Figure 2). Specifically, there was increased expression of MMP9 among patients without progression compared to those with progression in the lateral and/or patellofemoral compartments (7.2-fold; P = .038) and compared to those with rapid progression in the medial compartment (5.0-fold; P = .023). There was increased expression of CXCL6 (9.5-fold; P = .042) and LEP (4.3-fold; P = .047) among those without any radiographic OA progression compared to those with rapid progression in the medial compartment.
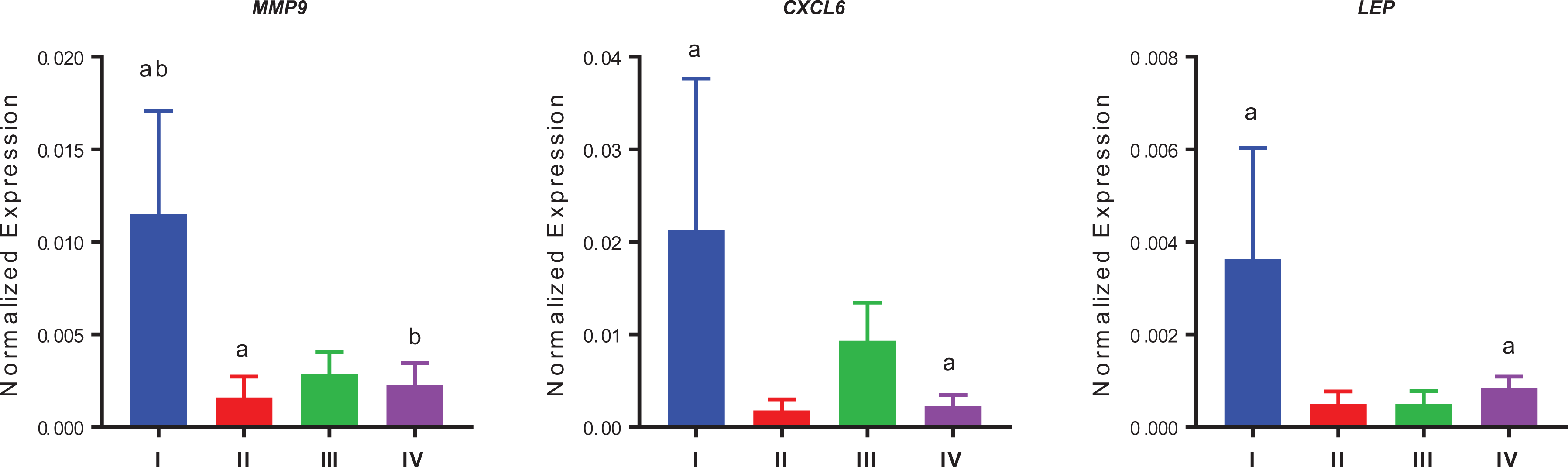
Gene transcripts differentially expressed across patients with different categories of radiographic osteoarthritis (OA) progression (Kellgren-Lawrence grades: I [minimal], II [mild], III [moderate], IV [severe]) at follow-up based on knee compartment and rate of progression. Label a indicates a significant difference between 2 groups (P < .05). Similarly, label b indicates a significant difference between 2 groups (P < .05).
Post hoc analysis was performed to assess the effect of patient age and BMI as well as tear pattern. Adjusting for patient age and BMI did not change the results.
In patients without any radiographic OA progression, a tear characterized as “degenerative” was found in 75% of patients and “traumatic” in 25% of patients. Analysis of patients with a progression of radiographic OA demonstrated “degenerative” tears in 83% and “traumatic” tears in 17%.
Discussion
The association of gene expression in the injured meniscus at the time of APM with progression of radiographic OA within 6 years of surgery is a novel finding with potentially important implications for predicting and preventing the development of OA after this common injury. Previous studies have investigated gene expression of the meniscus one snapshot at a time (ie, at the time of TKA or APM) 2,3,27,28,30,31,34,35,37 but not how it may be associated with the progression of radiographic OA. This study provides the first evidence that gene expression signatures at the time of partial meniscectomy can predict the progression of OA at medium-term follow-up. Patients without any radiographic OA progression had increased expression of several OA- and obesity-related genes in the meniscus at the time of APM. As these genes have been implicated in the pathogenesis of OA or obesity, 2,3,12,13,16,26,41,42 the reason for their elevated expression in the meniscus of nonprogressors at the time of surgery is not immediately clear. One possible explanation is that the expression of these genes represents a repair response in the metabolic activity of the meniscus after an injury, which may be chondroprotective, as these patients had no radiographic OA at baseline or final follow-up.
Much of the available research on the pathogenesis of OA has focused on biological activity within articular cartilage. 39 However, recent studies have investigated how differing biological activities within the meniscus and articular cartilage relate to OA. Brophy et al 5 recently reported clustering of meniscal transcripts among patients undergoing APM without OA compared to those with end-stage OA undergoing TKA. Patients with non-OA menisci exhibited a “repair” phenotype compared with a more inflammatory phenotype in the menisci of patients undergoing TKA. 5 In a similar study, the authors characterized the gene expression profile of articular cartilage in patients with meniscal tears undergoing APM and in patients with end-stage OA undergoing TKA. 32 The authors reported distinct sets of OA transcripts between these 2 groups of patients, with APM cartilage exhibiting molecular signatures reflective of OA but in an earlier stage. 31,32 Interestingly, when looking at specific transcripts that were overexpressed among patients undergoing APM in these studies, there were no common transcripts overexpressed in both meniscal and articular cartilage tissue. Similarly, there were very few transcripts overexpressed in both menisci and cartilage in patients undergoing TKA. These findings suggest that the gene expression profiles within the meniscus and articular cartilage differ, particularly in the setting of a meniscal injury.
It has been estimated that 30% to 75% of patients develop subsequent knee OA within 10 to 20 years of APM. 8,19,21 While it has been suggested that degenerative tears may be associated with radiographic OA after meniscectomy, 9 few studies have investigated the biological differences between traumatic and degenerative tears. Brophy et al 4 recently analyzed gene expression within the menisci of patients with degenerative and traumatic tears, demonstrating that gene expression varied by tear pattern. Patients with traumatic tears had increased expression of certain chemokines (IL8 and CXCL6) and matrix metalloproteinases (MMP1 and MMP3). In the present study, we demonstrated that nonprogressors had significantly increased expression of the chemokines IL8 and CXCL6, among other genes, compared with progressors. In the present study, we initially chose not to consider tear type (degenerative vs traumatic), as it is often difficult to ascertain, particularly in a middle-aged patient cohort, whether the cause was truly degenerative, traumatic, a combination of both, or something else. After our data analysis revealed common genes overexpressed in nonprogressors and in patients with traumatic tears, as described in a previous study, 4 we performed a post hoc analysis comparing tear type (degenerative vs traumatic) between nonprogressors and progressors. This analysis demonstrated no difference in tear type among nonprogressors and progressors. While further analysis was not performed, it is unlikely that tear type alone is responsible for the gene expression profile as it relates to the progression of OA after APM.
Several previous studies have investigated gene expression of the meniscus in noninjured knees, 26,38,41 at the time of surgery in the setting of a meniscal injury, 2,3,27,28,30,31 and at the time of TKA in knees with end-stage OA. 35,37 Using gene expression analysis of meniscal tissue obtained from the same cohort of patients undergoing APM as in the present study, Brophy et al 2 demonstrated significant differences in meniscal gene expression based on age, sex, and injury pattern, which may be clinically relevant. Elevated expression of OA-related genes was seen in association with age and injury pattern. Among other genes, the expression of MMP9 was significantly higher in patients younger than 40 years, and the expression of CCL3 and CCL3L1 was significantly higher in patients with combined meniscal and anterior cruciate ligament tears compared with a meniscal tear alone. 2 Younger patients and patients with a combined injury mechanism may be more likely to mount a more robust biological response to an injury compared with older patients and compared to those with an isolated meniscal injury, respectively. In the present study, we demonstrated overexpression of some of these same genes (CCL3, CCL3L1, MMP9) among nonprogressors. While further research is necessary, it is possible that elevated expression of these and other genes within the meniscus may indicate a more robust biological response after a meniscal injury that may be chondroprotective. Even though several of these genes have been implicated in the pathogenesis of OA, 2,30 these nonprogressors had no radiographic OA at the time of surgery or at final follow-up. The role of these genes specifically within the injured meniscus remains to be defined and deserves further study.
There are several limitations to the current study. First, as discussed earlier, we only investigated the meniscal expression of OA- and obesity-related genes, which were selected based on their known role in cartilage homeostasis, OA, extracellular matrix degradation, and obesity. 2,3,30 We did not investigate non-OA genes, or genes that may protect from OA, such as IL4 and IL10, 15 IGF1, 20 and IL1RA, 23 among others. As mentioned earlier, we did not consider tear type (degenerative vs traumatic), as it is often difficult to ascertain, particularly in a middle-aged patient cohort, whether the cause was truly degenerative, traumatic, a combination of both, or something else. Post hoc analysis of the data set suggests that this would likely not have affected the results of the study. We did not characterize the configuration and location of the tear within the medial meniscus for each patient and understand that this is a limitation of the study. However, all patients did undergo isolated partial medial meniscectomy. As this was a relatively small cohort of patients, it would have been impossible to adequately control for tear configuration, tear location, and amount of meniscal resection.
The meniscus was selected for this study in part because its tissue is typically disposed of at the time of partial meniscectomy, minimizing the potential impact on the patient compared with performing a biopsy of articular cartilage, for example. Furthermore, OA is a disease of the entire knee joint, involving not only articular cartilage but also the menisci and synovium. 18 As such, we feel that it was reasonable to explore the association of meniscal gene expression and the development of OA. Future prospective studies could investigate gene expression of menisci and other tissue such as articular cartilage, synovial fluid, and the synovium collected from the same patients. The study results may not be generalizable, as it was performed at a single academic center in a cohort that may be slightly heavier and older than the average population undergoing APM, although the did not change when adjusted for age and BMI. It is not possible to discern whether these genes were altered at the time of injury or before injury, although that distinction is less important from a clinical perspective, as patients typically present to the clinic after a meniscal tear occurs, and this information has the greatest potential utility in patients undergoing APM.
The study only looked at patients undergoing medial APM, and the results may not be the same for the lateral compartment. In addition, these results are for an intermediate follow-up at a mean 6.2 years after surgery, and they may differ at longer follow-up. At the time of initial enrollment, patients consented to allow us to contact them for follow-up studies in the future, but because we did not initially intend to collect medium-term clinical and radiographic follow-up data, we cannot consider this a prospective study. The small number of nonprogressors is a limitation of the study, which is subject to type II (beta) errors. Finally, we were only able to determine an association of gene expression with OA progression, not causation. By demonstrating an association of gene expression with OA, we are not suggesting that differential gene expression is solely responsible for OA progression. We recognize the biomechanical consequences of meniscectomy and their contribution to subsequent OA. 1
Conclusion
Increased expression of certain genes in the meniscus at the time of APM may be associated with a lower likelihood of OA progression at intermediate follow-up after surgery. Future investigations should look at a larger panel of target genes, including those with known protective roles against OA progression. Additionally, larger and longer longitudinal investigations are needed with respect to how gene expression in the meniscus is associated with the risk for the initiation and progression of knee OA. Ultimately, this line of investigation could facilitate a more precise determination of the risk for OA progression among patients with meniscal injuries and may be able to identify possible approaches, including targets for novel pharmacotherapies, to delay or prevent OA.
Footnotes
Accepted for presentation at the annual meeting of the AOSSM, July 2020.
Final revision submitted December 17, 2019; accepted December 23, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study received support from an OREF Resident Clinician Scientist Training Grant (award 18-014 to J.D.L.). J.D.L. has received educational support from Elite Orthopaedics. R.H.B. has received educational support from Arthrex and Elite Orthopaedics, speaking fees from Smith & Nephew, and consulting fees from ISTO Technologies and Sanofi. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Washington University in St Louis Institutional Review Board (No. 201509165).