
Abstract
Background:
Thumb ulnar collateral ligament (UCL) tears are common in competitive athletes. These tears often occur as a result of a radially directed force on an extended thumb. To date, no literature exists on the use of suture tape augmentation for repair of the thumb UCL in a competitive athlete cohort.
Hypothesis:
Using suture tape augmentation for the thumb UCL will allow for a safe and expedient return to play in competitive athletes.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective chart review was completed to identify all patients who underwent operative primary thumb UCL repair between 2014 and 2018. All procedures were performed at a single institution by the senior author. Inclusion criteria were acute complete tears of the thumb metacarpophalangeal joint UCL, treated with primary repair via suture tape augmentation in competitive high school, collegiate, or professional athletes. Exclusion criteria included recreational athletes, patients who underwent reconstruction (rather than repair), and patients with insufficient follow-up to establish return to play. Charts of patients identified through the retrospective review were further evaluated to determine patient- and injury-related variables. Return to play was defined as return to game competition and stratified as to whether this was at the same level of competition or any level of competition.
Results:
A total of 18 thumbs in 17 competitive high school, collegiate, and professional athletes were included in this study. One of the professional basketball players sustained injury to both thumbs approximately 10 months apart. The study group comprised 4 collegiate baseball players, 6 professional baseball players, 3 professional basketball players, 1 professional hockey player, 1 amateur-level hockey player, 1 high school basketball player, and 1 high school volleyball player. Mean follow-up was 27.9 months, and no complications were noted. Athletes who sustained an in-season injury (n = 13; 72.2%) returned to play at any level at a mean ± SD of 30.9 ± 10.1 days and at the same level at 36.3 ± 11.2 days. Athletes who sustained an out-of-season injury (n = 5; 27.8%) returned to play at any level at 101.4 ± 86.6 days and at the same level at 114.6 ± 87.0 days.
Conclusion:
The findings presented here offer evidence for return to play in competitive high school, collegiate, and professional athletes with a thumb UCL tear treated with repair and suture tape augmentation. All athletes returned to the same level of play. Those attempting to return in-season returned to the same level of play at a mean of just under 5 weeks. Augmenting the repair with anchored suture may prevent prolonged immobilization, expedite thumb motion, and improve postoperative recovery.
Thumb ulnar collateral ligament (UCL) tears occur commonly in elite athletes. 1,6,15 The mechanism of injury is a radially directed force on an extended thumb, which can occur when an athlete falls onto an abducted thumb, slides into a baseball base, or attempts to catch a ball. 1,5,9,10 In acute cases of complete tears involving high-level athletes, the ligament should be repaired to provide metacarpophalangeal (MCP) joint stability, restore pinch strength, and return athletes to play. 7,11 In-season injuries have traditionally resulted in missed time for elite athletes. 17,18 Missed playing and practicing time may have adverse financial and professional repercussions.
Minimal literature exists on return to play in elite athletes after UCL repair. 2,4,5,20 Few case series exist describing return to play after thumb UCL repair. 6,15,17,18 This article provides data on return to play after UCL repair with suture tape augmentation in competitive high school, collegiate, and professional athletes. The goal of suture tape augmentation of a ligament repair is to add significant strength to the repair at time zero. A recent biomechanical study comparing the strength of a traditional suture anchor repair versus a repair augmented with suture tape found that the augmented repair was at least 5 times stronger than the suture anchor repair. 13 Suture tape augmentation has been used with success in a number of ligament repair techniques throughout the body. 8,12,14,16,19,21 To date, no clinical study exists on the use of suture tape augmentation for repair of the thumb UCL.
Primary ligament repair without suture tape augmentation has often resulted in prolonged immobilization and protection of the thumb postoperatively. Our hypothesis was that using suture tape augmentation for the thumb UCL repair would allow for a safe and expedient return to play in competitive high school, collegiate, and professional athletes. The aim of this study was to evaluate return to play (at any level as well as at the same level of competition) in competitive high school, collegiate, and professional athletes after thumb UCL repair with suture tape augmentation.
Methods
Patients
After institutional review board approval was granted, a retrospective chart review was completed to identify all patients who underwent operative treatment of thumb UCL tears (Current Procedural Terminology codes 26540, 26541, and 26542) between 2014 and 2018. All procedures were performed at a single ambulatory surgical center by the senior author (S.S.S.). Inclusion criteria were complete tears of the thumb MCP joint UCL that were treated with primary repair and suture tape augmentation in competitive high school, collegiate, or professional athletes. Exclusion criteria included recreational athletes, patients who underwent reconstruction (rather than repair), and patients with insufficient follow-up to establish their return to play. A minimum 1-year follow-up was required.
Preoperative Evaluation
All patients presented to the senior author for evaluation of their thumb injury. The diagnosis of a thumb MCP UCL tear was made based on history and physical examination. Patients were diagnosed with a grade III (or full-thickness) tear if they had positive clinical findings (eg, tenderness at the ulnar aspect of the thumb MCP joint and laxity or soft endpoint with passive radial stress testing of the joint) and magnetic resonance imaging findings consistent with an acute complete tear of the thumb MCP UCL. Stener lesions, which occur when the adductor aponeurosis is interposed between the ligament and its distal insertion, thereby preventing normal healing of the ligament, were noted if present. Acute tears were defined as tears that resulted from an injury with an appropriate mechanism. Chronic tears were defined as tears that resulted from repetitive stress or where no appropriate injury or mechanism could be elucidated.
Surgical Technique
The surgical technique used by the senior author was consistent among all included patients. This technique has been previously described. 3 The patient was positioned supine on an operating room table with an attached hand table. A tourniquet was applied to the operative extremity. A longitudinal midaxial incision was made over the ulnar aspect of the MCP joint. The surgeon performed dissection of the subcutaneous tissues, taking care to preserve surrounding neurovascular structures. The distally torn ligament was dissected free from surrounding soft tissues. A 2.5-mm PushLock anchor (Arthrex) loaded with SutureTape (Arthrex) and a No. 3-0 FiberWire suture (Arthrex) was inserted into the volar-ulnar base of the proximal phalanx, the normal anatomic location of distal UCL attachment. The UCL was repaired back to this location by use of the preloaded FiberWire suture. The suture tape tails were then held taut and brought proximally in line with the ligament to the ulnar aspect of the metacarpal head (Figure 1). Holding the MCP joint in approximately 30° of flexion, the surgeon anchored the tails at the normal anatomic location of the proximal UCL attachment using a 3.5-mm DX SwiveLock anchor (Arthrex). It was necessary to maintain this slightly flexed position of the MCP joint in order to preserve full passive flexion of the joint. The thumb MCP joint was then examined to confirm resistance to radial stress and maintenance of full motion. The incision was closed in layers. After deflation of the tourniquet, a plaster thumb spica splint was applied.

Example of suture augmentation of a repair of the thumb ulnar collateral ligament. Arrow indicates to suture augmentation.
Postoperative Management
All patients returned within 1 week for a wound check and were fitted for a custom hand-based thumb spica orthosis. Occupational therapy was initiated with the goal of normalization of the soft tissues and restoring thumb MCP and interphalangeal motion. Sutures were removed at 2 weeks. Several different factors were considered when determining whether a patient could return to sport, including sufficient healing of the incision and soft tissues, ability to tolerate pain associated with the demands of the patient’s sport with or without a splint, and the patient’s overall level of comfort. No strength testing measurements were used in return-to-play determinations.
Return to Play
Charts of patients identified from the retrospective review were further evaluated to determine patient-related and injury-related variables. Return to play was defined as return to game competition at any level. This date was obtained from publicly available sources reporting on athlete participation in sporting competitions. These data were stratified depending on whether the surgery took place in-season or during the off-season. Return to play was also stratified based on the level of play to which the athletes returned, including whether it was the same level or a lower level of play. Professional baseball includes major and minor league levels of play. Professional hockey also includes major and minor league levels of play. Follow-up for each patient was calculated from the time of surgery to the patient’s final communication with the treating physician. A minimum 1-year follow-up was required for a patient to be included in the study. Standard deviations were calculated for all mean values.
Results
A total of 18 thumbs in 17 high-level athletes were included in the study. The study group consisted of 4 collegiate baseball players, 6 professional baseball players, 3 professional basketball players, 1 professional hockey player, 1 amateur-level hockey player, 1 varsity high school basketball player, and 1 varsity high school volleyball player. One of the professional basketball players sustained injury to both thumbs approximately 10 months apart (Table 1). The patients’ ages ranged from 15 to 31 years, with a mean age of 22.9 years at the time of surgery. Of the 18 thumb injuries in 17 athletes, 100% returned to play at the same level. No complications were reported at a mean follow-up of 27.9 ± 10.0 months (range, 14-45 months).
Characteristics of Patients Undergoing Thumb Ulnar Collateral Ligament Repair With Suture Tape Augmentation a
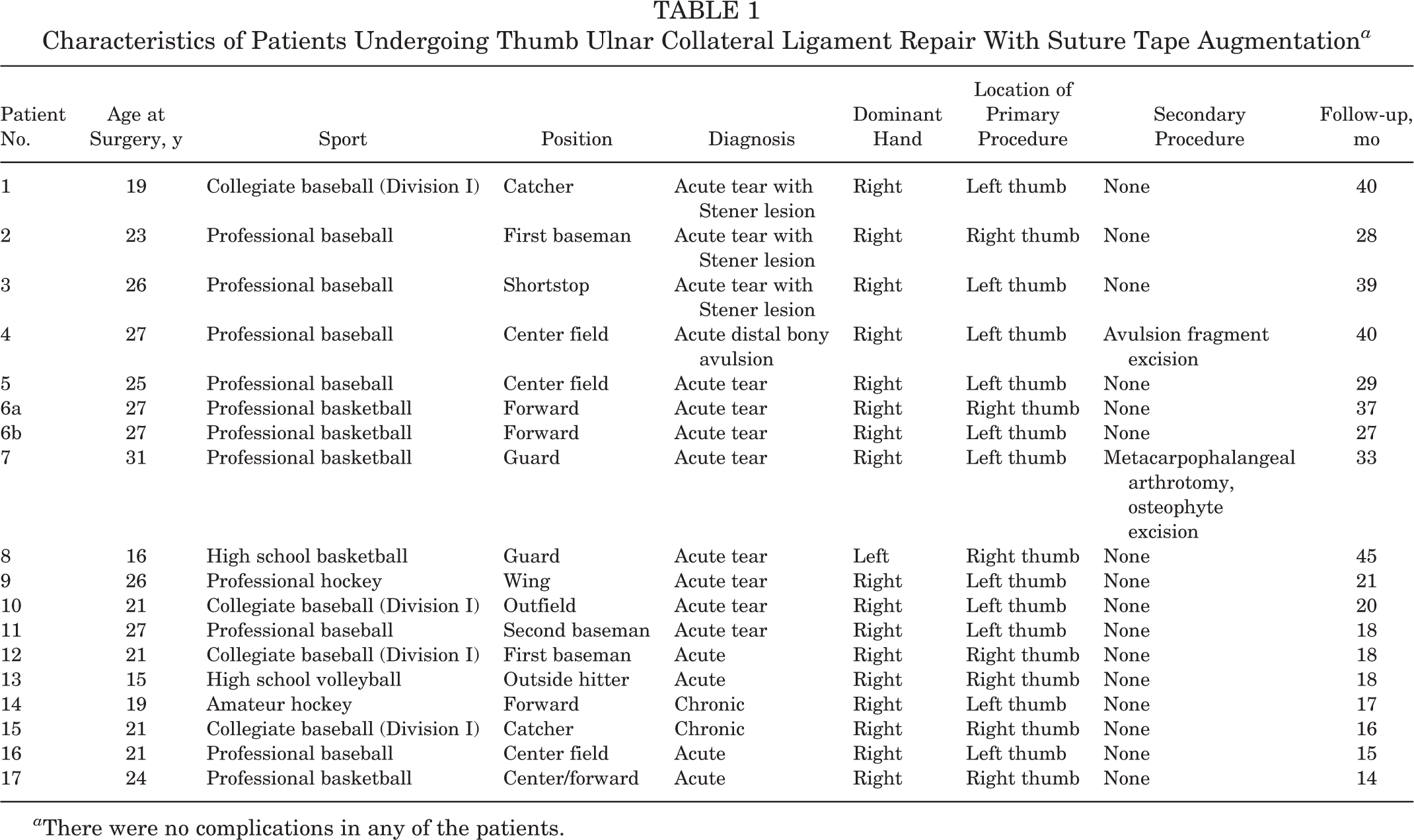
a There were no complications in any of the patients.
Athletes who sustained an in-season injury (13/18 thumbs; 72.2%) returned to play at any level at 30.9 ± 10.06 days (range, 14-48 days) and at the same level at 36.3 ± 11.22 days (range, 15-48 days). Athletes who sustained an out-of-season injury (5/18 thumbs; 27.8%) returned to play at any level at 101.4 ± 86.61 days (range, 23-243 days) and at the same level at 114.6 ± 86.97 days (range, 23-243 days) (Tables 2 and 3).
Return to Play for Patients Undergoing Thumb Ulnar Collateral Ligament Repair With Suture Tape Augmentation

a The time given includes time from the offseason of the athlete’s sport.
Mean Return to Play for Patients Undergoing Thumb Ulnar Collateral Ligament Repair With Suture Tape Augmentation a
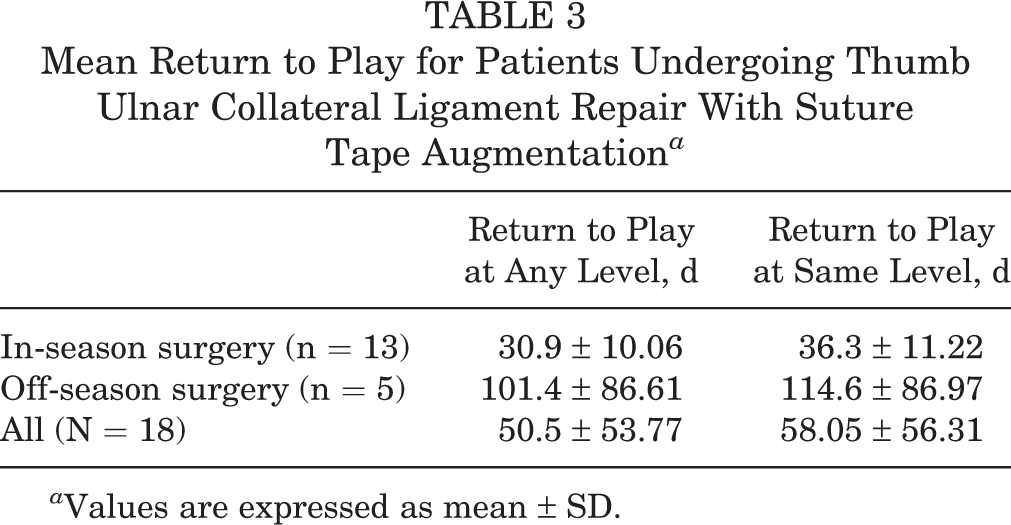
a Values are expressed as mean ± SD.
Discussion
In competitive high school, collegiate, and professional athletes, a complete tear of the thumb UCL requiring repair often results in missed practices and games. Returning athletes to competition both safely and as quickly as possible is the primary goal of surgeons who treat these athletes. Our study confirmed our hypothesis with a 100% return to play at a mean follow-up of 27.9 months and no reported complications in 18 thumbs in 17 competitive high school, collegiate, and professional athletes.
Expert opinion and existing case series on return to play after thumb UCL repair offer a wide range of timeframes. Carlson 2 recommended a 6- to 8-week return to play in basketball athletes. Werner et al, 18 in a case series on collegiate football athletes undergoing UCL repair, found a mean return to play of 7 weeks for skill players. Sochacki et al, 15 using publicly reported data, found a mean return to play of 132.2 days in National Football League players who underwent a thumb UCL repair. For athletes who returned within the same season as their surgery, their return was 34.8 days. 15 Jack et al, 6 also using publicly reported data, found a mean return to sport of 120.0 days for Major League Baseball players who underwent a thumb UCL repair, with an in-season return of 56.2 days.
Dy et al, 4 in a survey of consultant hand surgeons for the National Football League, National Basketball Association, and Major League Baseball, found a large range of return-to-play recommendations. Some surgeons recommended protected return to play immediately, whereas others recommended return to play at 2 weeks, 6 weeks, and even 3 months. Unprotected return to play varied from 6 weeks to 6 months. In our series of 18 suture tape–augmented thumb UCL repairs in 17 athletes, we found a mean in-season return to play of 30.9 days (4 weeks and 2.9 days) for all sports for return to play at any level.
The technique and biomechanical study of suture tape augmentation for thumb UCL repairs have been previously described by the senior author. 3 To our knowledge, this is the first reported series of competitive high school, collegiate, and professional athletes returning to play after undergoing thumb UCL repair with this technique. Suture tape augmentation acts as an internal brace and increases load to failure of the repaired tissue during ligament healing. 13 As noted, the thumb MCP joint is held in 30° of flexion to avoid overconstraining the joint and shielding the repair from normal stresses necessary for healing. 3 In our series, we noted 100% return to play at the same level with no failures and no complications. We believe that the increased strength and stability afforded by suture tape augmentation of the thumb UCL repair expedited return to play in this group of athletes. 13
This case series has obvious limitations. The lack of a control group presents an obvious problem. Sport-specific differences between basketball, hockey, volleyball, and baseball athletes affect return to play. Additionally, some patients elected to undergo operative repair in their respective off-seasons. It was difficult to quantify the time from the injury to the date of surgery. This also made it difficult to quantify the time for their return to play. We attempted to account for this by stratifying our results based on whether the athlete underwent surgery in-season or during the off-season. Surgery during the season affords athletes an opportunity to demonstrate their return to play, using these criteria, in a more expedient manner than those athletes who have surgery in the off-season. Finally, this is a small case series with no documented physical examination at follow-up and no functional or patient-reported outcomes.
Despite these limitations, the findings presented here offer clinical support of a novel technique used in competitive high school, collegiate, and professional athletes with a common injury. All athletes returned to their preinjury level of play. We believe that by decreasing the time of postoperative immobilization and expediting the initiation of thumb motion and strengthening, suture tape augmentation of the thumb UCL repair improves the player’s overall postoperative recovery and allows for a safe and early return to play.
Footnotes
Final revision submitted January 13, 2020; accepted February 24, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.B.G. has received grant support from Arthrex; educational support from Arthrex, DJO, and Smith & Nephew; and hospitality payments from Stryker and Medical Device Business Systems. S.S.S. has received speaking fees, consulting fees, and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Cedars-Sinai Medical Center Institutional Review Board (ID No. Pro00050710).