
Abstract
Background:
Female athletes are more susceptible to sport-related concussions (SRCs) and experience worse outcomes compared with male athletes. Although numerous studies on SRC have compared the outcomes of concussions in male and female athletes after injury, research pertaining to why female athletes have worse outcomes is limited.
Purpose:
To determine the factors that predispose female athletes to more severe concussions than their male counterparts.
Study Design:
Systematic review; Level or evidence, 3.
Methods:
A systematic review was performed according to PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) guidelines. The MEDLINE, EMBASE, CINAHL, PsychINFO, and Cochrane Library databases were systematically searched on July 5 to July 20, 2018. Included were cohort, case-control, and cross-sectional studies that examined the effects of concussive and subconcussive head impacts in only female athletes of all ages, regardless of competition level. These studies were further supplemented with epidemiologic studies. Exclusion criteria included narrative reviews, single case reports, abstracts and letters to the editor, and studies related to chronic traumatic brain injury.
Results:
A total of 25 studies met the inclusion criteria. Female athletes appear to sustain more severe concussions than male athletes, due in part to a lower biomechanical threshold tolerance for head impacts. Additionally, concussions may alter the hypothalamic-pituitary-ovarian axis, resulting in worse symptoms and amenorrhea. Although females are more likely to report concussions than males, underreporting still exists and may result in concussions going untreated.
Conclusion:
This systematic review demonstrates that female athletes may be more susceptible to concussion, have prolonged symptoms after a concussion, and are more likely to report a concussion than their male counterparts. However, underreporting still exists among female athletes. Possible factors that put female athletes at a higher risk for concussions include biomechanical differences and hormonal differences. To effectively prevent, diagnose, and treat concussions in female athletes, more research is required to determine when and how such injuries are sustained. Despite sex-based differences in the clinical incidence, reporting behavior, and outcomes of SRCs, female athletes remain an understudied population, resulting in lack of sex-specific treatment guidelines for female athletes postinjury.
Keywords
Given recent public health concerns related to concussions, there has been an increase in awareness and media coverage surrounding this injury. In the United States, an estimated 1.6 to 3.8 million sports and recreational concussions occur annually. 33 To reduce the impact of sport-related concussions (SRCs), state legislatures and the National Collegiate Athletic Association (NCAA) have implemented guidelines for medical management and return to play (RTP) after this injury. In 2010, the NCAA Executive Committee adopted a new concussion policy mandating annual concussion education for athletes and coaches, immediate removal from play, elimination of same-day return, and a process for medical clearance. 1
Analysis of SRC data collected over the past 20 years demonstrates an upward trend in concussion injury rates at both the high school and collegiate level, which is likely attributable to increased identification and reporting. 61,63 Recent studies demonstrate that SRCs account for nearly 15% of athletic injuries among high school athletes 40 and 6.2% of reported injuries among NCAA athletes. 63 In high school athletics, the incidence of SRC is highest in football, boys’ lacrosse, and girls’ soccer, with 9.21, 6.65, and 6.11 concussions occurring per 10,000 athlete-exposures (AEs), respectively. 43 At the NCAA level, SRC rates per 10,000 AEs are highest in men’s ice hockey (7.91), women’s ice hockey (7.5), football (6.71), and women’s soccer (6.31). 63 Across comparable sports at the high school and NCAA levels, studies have shown that female athletes experience higher rates of concussion than male athletes. 43,62
Sex-based differences regarding the incidence and outcomes of SRC have been reported. Such research has shown that female athletes may be more likely to sustain a concussion while playing sports than their male counterparts. 14,17,57 Women’s soccer, softball, and basketball have higher incidence rates of concussion than male-equivalent sports. 27,43,63 Even with intentional body-checking prohibited in women’s ice hockey and permitted in male ice hockey, female hockey players sustain nearly equivalent rates of concussion relative to male hockey players. 27,43,63 Additionally, female-dominated sports, such as cheerleading, have high rates of concussion. 34 Further, female athletes have demonstrated higher postconcussive symptom (PCS) scores, have slower reaction times compared with baseline, exhibit greater cognitive decline, and take longer to RTP after experiencing SRC in comparison with males playing comparable sports. 7,13,14,50,57 Research also suggests that female athletes have more prolonged concussion-related symptoms than their male counterparts. 7,12,46
Proposed explanations for these sex-based differences include physical and physiologic aspects, hormonal effects of estrogen and progesterone, and gender norms of behavior. 14,49 Several studies have reported that shorter neck dimensions, less head mass, and narrower neck girth result in less neck strength in female than male athletes, which predisposes girls and women to greater head-neck acceleration during impacts. 55,56 Recent research suggests that menstrual cycle phase and serum progesterone concentration at the time of a concussive injury are predictive of outcomes among women. 60 Additionally, female athletes tend to be more forthcoming in reporting their concussion-related symptoms. 14,57 These findings are important, as they may help with the development of a postconcussion management strategy for female athletes.
An abundance of research is available related to concussions in male-dominated sports (eg, football and hockey). However, there is a paucity of literature regarding the specific factors that predispose female athletes to higher incidence rates and worse outcomes after concussions. In 2014, the NCAA and the US Department of Defense Grand Alliance launched the Concussion Assessment, Research and Education (CARE) Consortium to provide the framework for longitudinal research on concussions and repetitive head impact exposure. However, only 35.4% of the eligible 25,000 NCAA student athletes and cadets enrolled by CARE Consortium institutions are female. 5 Furthermore, the 2017 Concussion in Sport Group (CISG) consensus statement was designed to develop a better understanding of SRC and to provide health care providers with guidelines to evaluate and manage SRC. 36 However, the statement did not recognize sex as a modifier for the current management of concussions, reporting a lack of conclusive evidence in published research on the issue. Instead, the consensus statement concluded that sex may be a risk factor and/or increase the severity of concussions.
The aims of this study were to (1) systematically evaluate the literature of concussions in female athletes and assess limitations of the studies, (2) identify potential factors that predispose female athletes to more severe concussions than male athletes, and (3) identify methods to improve future investigations into female athlete concussions.
Methods
This systemic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The review protocol was prospectively registered in the PROSPERO database for systematic reviews (protocol ID: CRD42018104356). For this systematic review, severity is based on outcome (ie, clinical recovery and return to play), risk, and incidence rate. SRC was defined according to the 2017 CISG consensus statement: a traumatic brain injury induced by biomechanical forces. 36
Search Strategy
A comprehensive search of the MEDLINE, EMBASE, CINAHL, PsychINFO, and Cochrane Library databases was performed from July 5 to July 20, 2018. Our search strategy consisted of the following key terms: athletic injuries, brain concussion, postconcussion syndrome, and female athletes, as well as their subject-related synonyms. A detailed list of specific search terms used is available in the Appendix. The terms used in the initial search were based on the National Library of Medicine’s controlled vocabulary thesaurus, also known as Medical Subject Headlines.
Article Selection and Data Extraction
Inclusion criteria were defined with the PICOS approach (population, intervention, control, outcome, study design). 42 Studies were included if they met the following criteria: evaluation of concussive and subconcussive head impacts in female athlete–only populations; head impacts that occurred during AEs (such as practice, training, or competition) regardless of competition level; study participants who were older than 10 years; and studies that were written in English and published from 2005 to 2018. Studies that examined both male and female populations for comparison were excluded. Narrative reviews, single case reports, abstracts, and letters to the editor on the subject were also excluded. Additionally, studies that included chronic traumatic brain injury were excluded. Numerous studies have compared male versus female athletes; however, our systematic review sought to evaluate studies that included female athletes only. By examining studies on female athletes only, the review sought to identify trends and risk factors associated with concussions in female athletes. Furthermore, the review sought to identify gaps in research related to concussions in female athletes, which could be explored in future studies.
A 3-step screening strategy was used to identify studies for inclusion in the review. First, study titles were screened for relevance. The remaining abstracts were subsequently screened for inclusion and exclusion criteria to identify relevant articles. Articles that satisfied title and abstract review underwent an in-depth full-text screen for inclusion and exclusion criteria. Reference lists of each included study were manually reviewed to identify relevant studies. This systematic review did not include a meta-analysis. Despite our attempts to provide uniform cohorts, lack of standardized outcome measures used throughout the literature made it difficult to compare studies and aggregate data into a meta-analysis. We reviewed and extracted data and then organized the data based on categories to provide a qualitative review. We then summarized the results of the studies based on the following categories: (1) biomechanics of impacts, (2) neuropsychological testing, (3) neurometabolic and neurostructural alterations, and (4) reporting behavior. Results of the search are shown in Figure 1.

Diagrammatic representation of search strategy.
Assessment of Risk of Bias and Level of Evidence
For each article that met inclusion criteria, the risk of bias and strength of evidence were independently rated by 2 authors (N.K.M., S.M.B.) using the quality assessment tools for observational cohort and cross-sectional studies and for case-control studies from the National Institutes of Health 54 and the levels of evidence from the Oxford Center for Evidence-Based Medicine 28 (Table 1).
Studies Meeting Criteria for Review a

a NIH, National Institutes of Health; OCEBM, Oxford Center for Evidence-Based Medicine; QAT, quality assessment tool.
Results
General Findings
The initial database search returned 1419 articles. Title screening yielded 245 relevant articles, and 87 abstracts were then screened for inclusion and exclusion criteria. A total of 44 articles underwent full-text review. Review of each included article’s reference list returned 4 additional relevant studies. Ultimately, 25 studies were included for qualitative analysis.
Biomechanics of Impacts: Frequency, Magnitude, and Threshold for Concussion
We identified 9 studies that specifically evaluated the frequency, direction, and magnitude of impacts sustained by female soccer, 26,32,35,37,47 hockey, 48,58 rugby, 31 and lacrosse 8 players. Peak linear acceleration (PLA) and peak rotational acceleration (PRA) associated with head impacts were used to measure impact magnitude variables in the study populations. Only 1 study 58 observed clinically diagnosed concussions. These studies are summarized in Table 2.
Biomechanical Head-Impact Metrics in Female Athletes a

a AE, athlete-exposure; HITS, Head Impact Telemetry System (Simbex); IQR, interquartile range (25th-75th percentile); IR, impact rate; NR, not reported; PLA, peak linear acceleration (g); PRA, peak rotational acceleration (rad/s2); SIM, Smart Impact Monitor (Triax Technologies); xPatch (X2 Biosystems), sensor system fixed over the mastoid process of the athletes; 50th, 50th percentile; 95th, 95th percentile.
b Values are expressed as mean or as mean ± SD.
c Values are expressed as mean ± SD (range) or median [IQR].
d Values of findings for McCuen (2015) 37 are expressed as mean; median.
Wilcox et al 58 examined the biomechanics of head impacts in female collegiate hockey players over the course of 2 seasons. The study reported that the frequency and magnitude of head impacts per player was higher during AEs when a concussion occurred in comparison with AEs without such a diagnosis. Of the 9 reported concussions, 4 were associated with a single impact (mean PLA 43.3g ± 11.5g and PRA 4030 ± 1243 rad/s2). In 2017, Reed et al 48 evaluated head impacts sustained by youth female hockey players over the course of 3 seasons (total of 66 games). Although no players in the study experienced a concussive event, the study identified potential risk factors (higher body mass index [BMI], older age, ice time, and body positioning) associated with increased severity and frequency of impacts. A higher player BMI was the greatest predictor of head impacts per game. The mean PLA and PRA of the head impacts experienced by female youth hockey players in the study by Reed et al were similar to those experienced by the female collegiate hockey players who did not sustain a concussion in the study by Wilcox et al.
In recent studies on female collegiate soccer players, xPatch and Smart Impact Monitor (SIM) accelerometers were used to quantify head impacts during AEs. 32,35,37,47 No participants reported concussions during any of the 4 studies on collegiate soccer players. As shown in Table 1, these studies reported a wide range of head impact magnitudes. However, it is important to note that McCuen et al 37 recorded head impacts with a resultant linear acceleration exceeding 20g. In contrast, studies by Lynall et al 35 and Press and Rowson 47 used a linear acceleration threshold of 10g to initiate data collection. Further, Lynall et al reported that nearly 90% of head impacts sustained by their athletes were less than 20g.
Using video analysis to verify recorded impacts in female collegiate soccer players, Lamond et al 32 and Press and Rowson 47 examined the magnitude of head impacts based on event type. Lamond et al demonstrated that head-to-head impacts generated a greater PLA (51.26g ± 36.61g) than purposeful headers from shots (32.94g ± 12.91g), clears (31.09g ± 13.43g), and passes (26.11g ± 15.48g). Press and Rowson found that unintentional ball-to-head contact produced a greater average PLA (35g) than player-to-player contact (27g) and purposeful headers (20g). In a study on youth female soccer players, Hanlon and Bir 26 demonstrated that video-verified purposeful headers had a PLA of 4.5g to 62.9g and a PRA of 444.8 to 8869 rad/s2.
Caswell et al 8 characterized head impacts sustained in girls’ varsity high school lacrosse games over the course of 2 competitive seasons (28 games total). All game-related impacts greater than 20g recorded by impact sensors were verified with video analysis, which demonstrated that only about half of the measured impacts greater than 20g were associated with impacts to the head. The study reported a mean impact rate of 1.1 per team game and found that athletes sustained fewer than 2 head impacts greater than 20g per season. King et al 31 examined head impact exposure in women’s rugby players over the course of 1 competitive season (9 matches) and reported recorded impacts greater than 10g (range, 10g-91g) with a mean of 184 ± 18 impacts per match, resulting in a mean of 14 ± 12 impacts per player per match.
Neuropsychological Testing After Concussive and Subconcussive Head Impacts in Female Athletes
Our search identified 6 studies that examined neurocognitive function after concussive and subconcussive head impacts in female athletes (Table 3). 19,20,25,29,30,34 Lovell and Solomon 34 used the ImPACT (Immediate Postconcussion Assessment and Cognitive Testing) to evaluate female cheerleaders within 7 days of sustaining a concussion. The authors found that concussed athletes performed significantly worse on ImPACT tests compared with their baseline, including 37% of concussed athletes who reported no clinical symptoms.
Neuropsychologic Testing After Concussive and Subconcussive Head Impacts in Female Athletes a

a ANAM, Automated Neuropsychological Assessment Metrics computer program (simple reaction time, attention and concentration, math processing, visual memory, and working memory); CSC, Concussion Symptom Checklist (scores yield overall symptom score); EXP, players with a diagnosis of concussion (mean number of concussions, 1.3 ± 6); HVLT, Hopkins Verbal Learning Test (verbal memory); ImPACT, Immediate Postconcussion Assessment and Cognitive Testing, an assessment tool that includes a demographic questionnaire, injury evaluation form, 22-item Post-Concussion Symptoms (PCS) scale, and a 25-minute neurocognitive test battery; modified Romberg, indirect measure of postural stability but not part of the ImPACT tool; NA, not applicable; NR, not reported; WDST, Wechsler Digit Span Test (concentration and immediate memory recall).
b The 10-test battery includes the California Verbal Learning Task (total immediate recall and delayed recall), Ruff 2 & 7 Selective Attention Test (speed and accuracy), Digit Span (verbal short-term and working memory), Letter Fluency Test, Brief Test of Attention, Symbol Digits Modalities Test, Tower of London Dx (TOLDX), simple reaction time, and choice reaction time (CRT).
Ellemberg et al 19 used a test battery consisting of 10 paper-and-pencil and computerized tasks to assess different neuropsychological functions after a first-time concussion in female collegiate soccer players 6 to 8 months after injury. This time period was chosen to limit the practice effect and RTP motivation associated with short-term follow-up testing. The control group consisted of age-matched teammates who had never experienced a concussion. The authors found that neuropsychological impairments related to decision making, inhibition, and planning persisted 6 months after injury.
Previous studies on female soccer players have examined the effects of purposeful heading on neuropsychological test performance, 4 of which found no significant correlation between purposeful heading and neuropsychological test results in both the immediate 25 and the postseason 20,29,30 settings. Forbes et al 20 examined whether cumulative subconcussive impacts over 1 season of girls’ high school soccer caused neurocognitive decline in players with or without a history of previous concussion. The authors found no difference in postseason neurocognitive examination performance between groups. Examining the immediate effects of purposeful heading on neurocognitive testing, Gutierrez et al 25 demonstrated that ImPACT performance immediately after a series of 15 directional headers (5 forward, 5 right, 5 left) did not significantly differ from baseline pretest ImPACT scores in a group of female high school athletes. In 2007, Kaminski et al 30 assessed the relationship between headers per season and neuropsychological and postural test performance in female high school and collegiate soccer players. The authors found no correlation between total number of headers and neuropsychological and postural test performance. In 2008, Kaminksi et al 29 again attempted to determine a relationship between purposeful heading and neuropsychological test performance in girls’ high school soccer. The study found no significant correlation between headers per game and postseason neuropsychological assessment metrics.
Neurometabolic and Neurostructural Alterations After Concussion
We identified 6 studies that examined long-term neurometabolic and neurostructural alterations after concussion. 9 –11,22,51,52 Recent neuroimaging studies used magnetic resonance spectroscopy (MRS) and diffusion tensor imaging (DTI) to identify axonal injury or neuronal loss in previously concussed collegiate and professional female athletes (Table 4). 9 –11,51 Studies by Chamard et al 9 –11 found neurometabolic and neurostructural abnormalities present on MRS and DTI neuroimaging at least 6 months after athletes sustained a concussion. However, the authors also found no neurometabolic or structural abnormalities evident on neuroimaging in concussed female athletes 7 to 10 days after injury. 9 These studies found no correlation between neuroimaging abnormalities and clinical concussive symptoms in the concussed female athletes. 9 –11 In female rugby players, Schranz et al 51 found neurometabolic derangements after a concussion and after a season in nonconcussed athletes suggesting that both concussive and repetitive subconcussive impacts may alter oxidative metabolism of the glutamine-glutamate pathway. Although the authors reported changes in white matter metabolite levels and DTI measures (Table 4), no correlation was found between clinical test scores and imaging metrics in concussed athletes.
Neuroimaging Findings in Concussed Female Athletes a
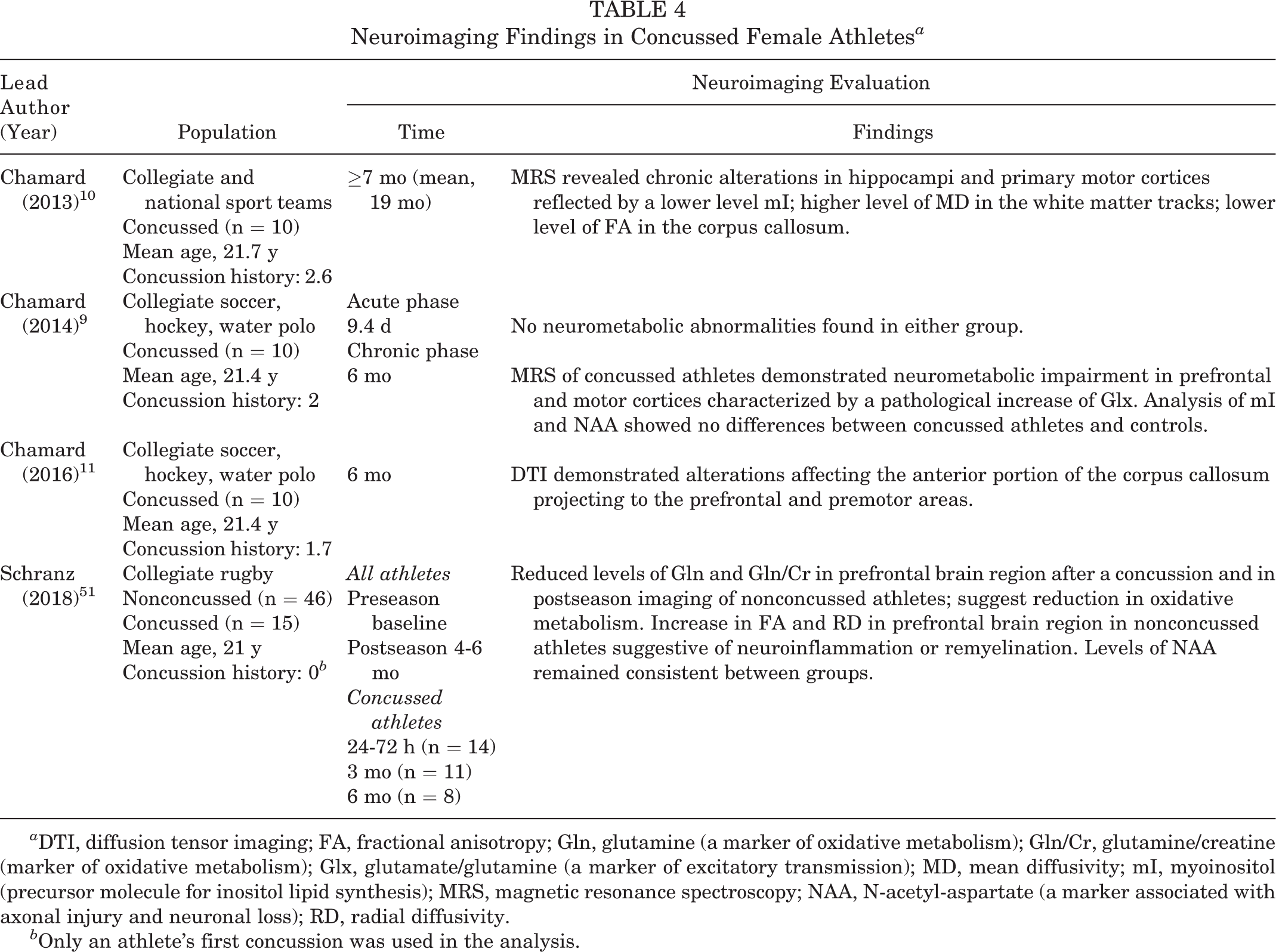
a DTI, diffusion tensor imaging; FA, fractional anisotropy; Gln, glutamine (a marker of oxidative metabolism); Gln/Cr, glutamine/creatine (marker of oxidative metabolism); Glx, glutamate/glutamine (a marker of excitatory transmission); MD, mean diffusivity; mI, myoinositol (precursor molecule for inositol lipid synthesis); MRS, magnetic resonance spectroscopy; NAA, N-acetyl-aspartate (a marker associated with axonal injury and neuronal loss); RD, radial diffusivity.
b Only an athlete’s first concussion was used in the analysis.
Our search identified 2 studies that examined the effects of concussion on the hypothalamic-pituitary-ovarian axis. 22,52 Using a weekly survey, Snook et al 52 prospectively surveyed female athletes ages 12 to 21 years who had experienced either SRC (n = 68) or sports-related orthopaedic injury (n = 61). Despite the groups having similar gynecologic age, BMI, and type of sports played, the risk of 2 or more abnormal menstrual bleeding patterns was significantly higher after concussions than after orthopaedic injuries (5.58; 95% CI, 1.61-21.22). Gallagher et al 22 examined the effects of hormonal contraception (HC) use after concussion in collegiate female athletes. The authors reported that non-HC users (n = 25) demonstrated higher symptom severity scores after concussions compared with HC users (n = 24). No significant differences were found between HC and non-HC females on length of recovery.
Reporting Behavior of Concussion-Like Symptoms
We identified 5 studies that examined concussion-reporting behavior in female athletes. 6,22,38,45,53 Studies showed that a significant percentage of adolescent, 45,53 high school, 38 and collegiate athletes 6,22 failed to report concussion-like symptoms (CLS) and that many of these athletes returned to play with CLS (Table 5). O’Kane et al 45 surveyed adolescent female soccer players over 4 years for the incidence of concussion. The authors found that reasons concussed athletes reported CLS after an impact included concern for making symptoms worse (39.0%) and advice from a parent (35.6%), health care provider (28.8%), or coach (28.8%). McDonald et al 38 surveyed female high school athletes from numerous sports about concussion histories and symptom reporting behavior over a 3-year period. The study found that factors for nondisclosure of CLS after an impact included the athletes’ misconceptions about the severity of injury and their desire to keep playing.
Reporting Behavior of Concussion-Like Symptoms a

a CLS, concussion-like symptoms; NA, not applicable; RTP, return to play; QHS, qualified healthcare provider.
b Sports with diagnosed concussion: soccer (36.4%), softball (33.8%), basketball (19.5%), volleyball (19.5%), cheerleading, dance, and motocross.
c 459 respondents of 1200 athletes who were originally sent the survey: 38.3% participation rate.
At the NCAA level, the prevalence of symptom nondisclosure is even higher. Brook et al 6 anonymously surveyed NCAA women’s ice hockey players to assess concussion history and nondisclosure of CLS. Among participants, the study found significantly high rates (Table 5) of nondisclosure of head impacts associated with CLS during the 2014-2015 hockey season and throughout the participants’ careers. In a retrospective chart review of concussed NCAA female athletes, Gallagher et al 22 found that factors contributing to nondisclosure of head impacts and RTP included delayed symptom onset and failure of the athlete to recognize the symptoms as a concussion.
Discussion
This systematic review describes factors that may predispose female athletes to worse outcomes after concussions in comparison with male athletes. Potential risk factors include female-specific head impact kinematics, sex-specific physiologic parameters that alter recovery, and underreporting of CLS. Furthermore, the systematic review reaffirms previous findings that females may have sex-specific predispositions for concussions and PCS. The same search strategy and inclusion criteria on male athletes yielded 270 PubMed full-text articles on the topic, in comparison with the 25 full-text articles found on female athletes. Thus, the review also highlights the scarcity of research on concussions in female athletes, despite evidence that findings from studies on male athletes cannot always be applied to female athletes.
Biomechanics of Impacts: Frequency, Magnitude, and Threshold for Concussion
Biomechanical studies have correlated head impact kinematics with the risk of brain injury. 18,39 The studies included in our review suggest that head-impact sensors (xPatch, Head Impact Telemetry System [HITS], SIM) do not provide a reliable means of diagnosing concussions; however, the real-time head impact data provide insight into the risk of head impact among female athletes. Additionally, this review suggests that female athletes may have a lower tolerance for linear head impacts than their male counterparts, and therefore guidelines on concussion-producing impact thresholds may need to be sex-specific.
In collegiate football players, a PLA threshold of 100g has been recommended to identify potential concussions. 21 A systematic review on concussions in male high school and collegiate football players reported that concussive impacts produced a mean PLA of 98.68g and PRA of 5776.60 rads/s2. 4 Wilcox et al 58 found that concussive impacts in women’s hockey generated a mean PLA of 43g ± 15g. This is significantly lower than the PLA associated with concussive impacts in male collegiate football players (range, 60.51-168.71g). 24 These findings suggest that female athletes have a lower biomechanical threshold for concussions, and the findings support previous assertions that the diagnosis of concussion is associated with both the magnitude and frequency of head impact exposure. 2
Neuropsychological Testing After Concussion and Subconcussive Head Impacts in Female Athletes
This systematic review demonstrated the clinical value of neuropsychological testing for providing effective postconcussive care, as it increases the capacity to identify female athletes with residual postconcussive neurocognitive deficits. Findings by Lovell and Solomon 34 demonstrated the benefits of neuropsychological testing in addition to self-reported PCS within 7 days of a concussion, because clinical symptoms alone may not be a reliable indicator of ability to RTP in female athletes. Ellemberg et al 19 reported that impairments may last 6 to 8 months postconcussion in female athletes. Previous studies 3 on the cognitive sequelae associated with brain injury have used the same testing metrics as Ellemberg et al. Although we found that concussed female athletes often have neuropsychological impairments, 19,34 we found no correlation between neuropsychological testing and subconcussive impacts associated with heading in female soccer players. 20,25,29,30 In male high school and collegiate football players, repetitive subconcussive injuries have been reported to increase the susceptibility of subsequent concussions 1,2,23 and decrease cognitive function, as demonstrated by neuropsychological testing. 1 This review does not answer whether there is a difference between male and female athletes regarding neuropsychological testing after subconcussive or concussive impacts.
Neurometabolic and Neurostructural Alterations After Concussion
Concussed female athletes showed neurometabolic and neurostructural alterations at least 6 months after the initial injury, as demonstrated by MRS and DTI neuroimaging. 9 –11,51 However, no neurometabolic abnormalities were seen in the acute phase (7-10 days) after concussive injury. 9 Our review found no significant clinical correlation between neuroimaging findings and concussive symptoms 9 –11 or neuropsychological testing. 51 This review cannot comment on sex-based differences in neurometabolic and neurostructural alterations evident on neuroimaging.
Menstrual cycle phase has not been shown to significantly affect clinical measures of concussion in female athletes, including performance on neurocognitive tests, postural stability, or symptoms, regardless of oral contraception use. 41 This systematic review found only 1 study to support these conclusions by reporting that female athletes may experience sex-specific consequences of concussion, namely, altered menstrual patterns. 52 Additionally, although use of HC was shown to have no effect on length of recovery postconcussion, female athletes who did not use HC exhibited greater concussive symptoms after injury. 22 Male and female differences in recovery after concussion thus cannot be attributed to stage in menstrual cycle or use of an oral contraceptive.
Reporting Behavior of CLS
Previous studies have found that women and adolescents experience more concussion-related symptoms and that symptoms in female athletes may last for a longer duration than those of their male counterparts. 16,17,22,57 An investigation of male and female athletes reported that female athletes had worse visual and verbal memory, postural stability testing, and symptom duration outcomes than their male counterparts after experiencing a concussion. 15 One theory suggests that female athletes are more open to reporting head collisions and subsequent concussive symptoms than male athletes because female athletes are more concerned about their future health than are male athletes. 14 However, our review found that despite higher rates of reporting in female compared with male athletes, 57 underreporting still exists and leads to potentially untreated concussions. 6,22,38,45,53
Limitations
There are several limitations to this study. First, the collection of reliable and valid data regarding concussions in female athletes is complicated by diverse diagnostic criteria, discrepancies in symptom reporting, and the potential for cultural and sex-specific factors to influence the diagnosis and management of concussions. Despite our attempts to provide uniform cohorts, lack of standardized outcome measures used throughout the literature made it difficult to compare studies.
Second, studies on the biomechanics of head impact were limited by the validity of the measuring devices (xPatch, HITS, SIM) and the possibility for inherent differences in technology. Caution should be used when generalizing findings for PLA and PRA, as several studies have shown that acceleration events captured by sensors may be susceptible to measurement errors. 44,47,59 Future studies should try to integrate sensor data with verified video analysis of head impacts. Third, studies on neurocognitive testing after concussive and subconcussive head impacts were limited by the discrepancies that exist between the different battery tests. Fourth, in many of the studies on neurometabolic and neurostructural alterations postconcussion, the frequency and magnitude of impacts were not recorded. As a result, such data could not be compared with the neuroradiographic findings and the symptom reporting of the participants. Fifth, the small sample sizes limited the quality and statistical power of the studies in this review. Additionally, many studies relied heavily on the self-reported concussion history and concussion-like symptoms, creating the potential for selection bias and recall bias.
Future research on concussions in female athletes would benefit from sufficiently powered, well-conducted, and high level of evidence prospective investigations to decrease bias in patient cohorts, subsequently allowing for more accurate comparisons across studies.
Conclusion
This systematic review demonstrates that female athletes may be more susceptible to concussion, have prolonged symptoms after a concussion, and are more likely to report a concussion than their male counterparts. However, underreporting still exists among female athletes. Possible factors that put female athletes at a higher risk for concussions include biomechanical differences and hormonal differences. To effectively prevent, diagnose, and treat concussions in female athletes, more research is required to determine when and how such injuries are sustained and whether treatment should be different in female athletes.
Footnotes
Final revision submitted November 13, 2019; accepted November 25, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.K.M. has received educational support from Arthrex, Quest Medical, and Alon Medical Technology; speaking fees from Arthrex; and hospitality payments from Tornier and Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Appendix
PubMed Search Strategy