
Abstract
Background:
The best method for nonsurgical treatment after primary dislocation of the shoulder is not clear. The efficacy of immobilization with the arm in external rotation (ER) compared with internal rotation (IR) remains controversial.
Purpose:
To determine the efficacy of ER immobilization versus IR immobilization on recurrence rate after primary dislocation of the shoulder from the evidence of randomized controlled trials.
Study Design:
Systematic review; Level of evidence, 2.
Methods:
Electronic databases (MEDLINE [Ovid SP], PubMed, Web of Science, EBM reviews, and CINAHL) and available proceedings according to the abstracts of major international meetings related to or including shoulder injuries and trauma were used to search for randomized controlled trials. Two independent investigators determined eligibility and carried out data extraction from the selected studies.
Results:
A total of 9 studies (817 patients) were selected for this meta-analysis. They included 668 male and 149 female patients, with a mean age ranging from 20.3 to 37.5 years. In the 9 pooled studies, the recurrence rate of shoulder dislocation was 21.5% (84/390) in the ER group versus 34.9% (130/373) in the IR group. ER immobilization significantly reduced the recurrence rate compared with IR immobilization (risk ratio, 0.56; P = .007). In the subgroup analysis of those immobilized full-time, ER immobilization was significantly more effective than IR immobilization in reducing the recurrence rate (risk ratio, 0.57; P = .01). In the subgroup analysis of age, ER immobilization was significantly more effective than IR immobilization in those aged 20 to 40 years but not in those younger than 20 years.
Conclusion:
This meta-analysis demonstrates that ER immobilization reduces the recurrence rate after primary shoulder dislocation compared with IR immobilization in patients older than 20 years. When treating a patient with primary shoulder dislocation, the clinician should provide this information to the patient before a treatment method is selected.
Among all the joints of the body, the shoulder is the most common site of traumatic dislocation. 14 Shoulder dislocation has a high recurrence rate, especially in the young. 27,28,35 Since the era of Hippocrates, clinicians have used immobilization in internal rotation (IR) after reduction. 6 However, neither the length nor the rigidity of immobilization has been shown to affect the rate of recurrence. 29 This fact suggests that the Bankart lesion created after the primary dislocation might not be effectively reduced in this position of immobilization. Itoi et al 10 demonstrated that the Bankart lesion was not reduced with the arm in IR but was reduced with the arm in external rotation (ER). Drawing on this observation, those investigators performed a randomized controlled trial (RCT), which showed that the relative risk of recurrence was reduced by 38% with use of immobilization in ER compared with immobilization in IR. 9 After this study, several RCTs were conducted and reported in the literature. Accordingly, several meta-analyses have also been reported, but the conclusions are controversial. Some meta-analyses showed that immobilization in ER was effective in reducing the recurrence rate, 19,24,32 but others reported otherwise. 3,13,17,36,38 Recently, a new RCT was added to the literature. 20 Thus, we sought to update our knowledge about the efficacy of immobilization in ER. The purpose of this study was to determine the efficacy of ER versus IR immobilization on recurrence rate after primary dislocation of the shoulder. We hypothesized that ER immobilization would reduce the recurrence rate after primary shoulder dislocation as compared with IR immobilization.
Methods
Types of Studies
The current analysis included RCTs or quasi-RCTs that evaluated the efficacy of immobilization in ER versus IR in patients with first-time shoulder dislocation. The quasi-RCTs adopted methods that divided the patients into intervention or control groups by quasi-randomization methods such as the patient’s chart number (odd vs even). In this analysis, nonrandomized or case-control studies were excluded.
Outcomes
Recurrence rates at the final follow-up after immobilization treatment were evaluated. We included studies with a minimum of 6 months of follow-up after initial treatment. Recurrence was defined as an obvious dislocation of the glenohumeral joint. The Western Ontario Shoulder Instability Index (WOSI) was also assessed. The WOSI has been used for subjective assessment of quality of life (QOL) for patients with shoulder instability and consists of 4 domains (physical symptoms, sports/recreation/work, lifestyle, and emotion) among 21 items. Each item can be measured using the score from a 100-mm visual analog scale. Therefore, overall WOSI scores obtained from 21 items range from 0 to 2100. For this study, quantitative QOL from WOSI was calculated as [(2100 – WOSI Score) ÷ 2100] × 100 and expressed as a percentage.
Literature Search
Electronic databases (MEDLINE [Ovid SP], PubMed, Web of Science, EBM reviews, and CINAHL) were used for the current analysis. MEDLINE (Ovid SP), EBM reviews, and CINAHL were used to search for articles with the following texts: [shoulder dislocation OR glenohumeral dislocation] AND [primary OR first time] AND [immobilization] AND [external rotation]. PubMed and Web of Science were used to detect articles with the following keywords: primary shoulder dislocation external rotation immobilization. The literature search using these databases was carried out on January 25, 2019. Subsequently, a reference manager (Endnote X8; Clarivate Analytics) was used to identify duplicate articles.
Available proceedings from major international meetings related to or including shoulder injuries and trauma were searched using the keywords shoulder dislocation, immobilization, and external rotation.
In examining the identified literature, 2 independent investigators (E.I., K.S.) determined the data to be eligible for inclusion by reviewing the contents carefully; that is, RCTs comparing recurrence rates after immobilization in ER and IR. In addition, we identified 1 RCT 37 that had been included in the previous meta-analysis. 17 This RCT was not detected through our literature search because it was not written in English; however, we considered it appropriate to include this study in our meta-analysis because the detailed data of this study had been provided in the previous meta-analysis. 17
Data Extraction
Data extraction was carried out by 2 independent reviewers (Y.S., K.S.). Information extracted from the data included the study design, sample size, patient demographics (age and sex), and immobilization details, including immobilized arm positions, duration of immobilization, and the mean follow-up period after immobilization. In addition, we extracted data regarding recurrence including the number of involved patients and their ages. If the data were insufficient, we tried to contact the authors to collect the necessary information.
We analyzed 189 articles that had been extracted with the electronic databases and excluded 110 duplicates using the reference manager, leaving 79 articles. Of these 79 articles, 64 studies were excluded, leaving 15 RCTs. The reasons for exclusion were review articles (n = 13); surgical treatment compared with nonsurgical treatment (n = 11); imaging and arthroscopic examination (n = 10); note, letter, and commentary (n = 10); nonsurgical treatment using brace and physical therapy (n = 7); repeat publications (n = 5); epidemiology, survey, and study design (n = 3); trials without results (n = 3); and case reports (n = 2). The remaining 15 full-text studies were assessed for eligibility. However, 6 studies were excluded because of the study design, imaging examination, or repeat publication. Finally, 9 studies were included in this systematic review and meta-analysis (Figure 1).

Flowchart of articles eligible for inclusion. The flowchart shows how the 9 randomized controlled trials (RCTs) were extracted from the databases. The MEDLINE database included Ovid MEDLINE in-process and other nonindexed citations, Ovid MEDLINE Daily, and Ovid MEDLINE, and Ovid OLDMED LINE 1946 to present. EBM reviews included American College of Physicians Journal Club, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Cochrane Methodology Register, Database of Abstracts of Reviews of Effects, Health Technology Assessment, and National Health Service Economic Evaluation Database. AANA, Arthroscopy Association of North America; AAOS, American Academy of Orthopaedic Surgeons; ASES, American Shoulder and Elbow Surgeons; ICSES, International Congress of Shoulder and Elbow Surgery; ISAKOS, International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine.
We investigated the quality of studies based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement (Table 1). The methodological quality of the trials ranged from low to moderate (total score, 65.08% ± 35.96%).
Risk of Bias a

a Risk of bias was assessed using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. NS, not specified; +, satisfied; −, not satisfied.
Statistical Analysis
This meta-analysis included studies that reported risk ratios and their confidence intervals by comparing IR versus ER immobilization after primary anterior shoulder dislocation. We performed a meta-analysis to calculate risk ratios and 95% CIs using the Mantel-Haenszel statistical method. A random-effects model was used to pool the data, and statistical heterogeneity among studies was evaluated via the I2 statistic (higher values denote greater heterogeneity). Sensitivity analysis was performed by excluding studies with low or unknown compliance 16,21,37 and studies with less than 24 months of follow-up. 21,34,37,39 To evaluate whether the association between treatment and the risk of recurrence was modified by patient characteristics, we also investigated subgroup analysis based on age (<20 years vs 20-40 years) (Figure 2).

Flowchart of articles in the subanalyses. RCT, randomized controlled trial; WOSI, Western Ontario Shoulder Instability Index.
All meta-analyses were performed with Review Manager 5.3 software (Cochrane Collaboration). All tests were 2-tailed, and P < .05 was considered statistically significant.
Results
Literature Search
We included 9 RCTs in our meta-analysis to compare the outcomes of immobilization in ER versus IR for patients with primary anterior shoulder dislocation (Tables 2 and 3).
Patient Demographics a
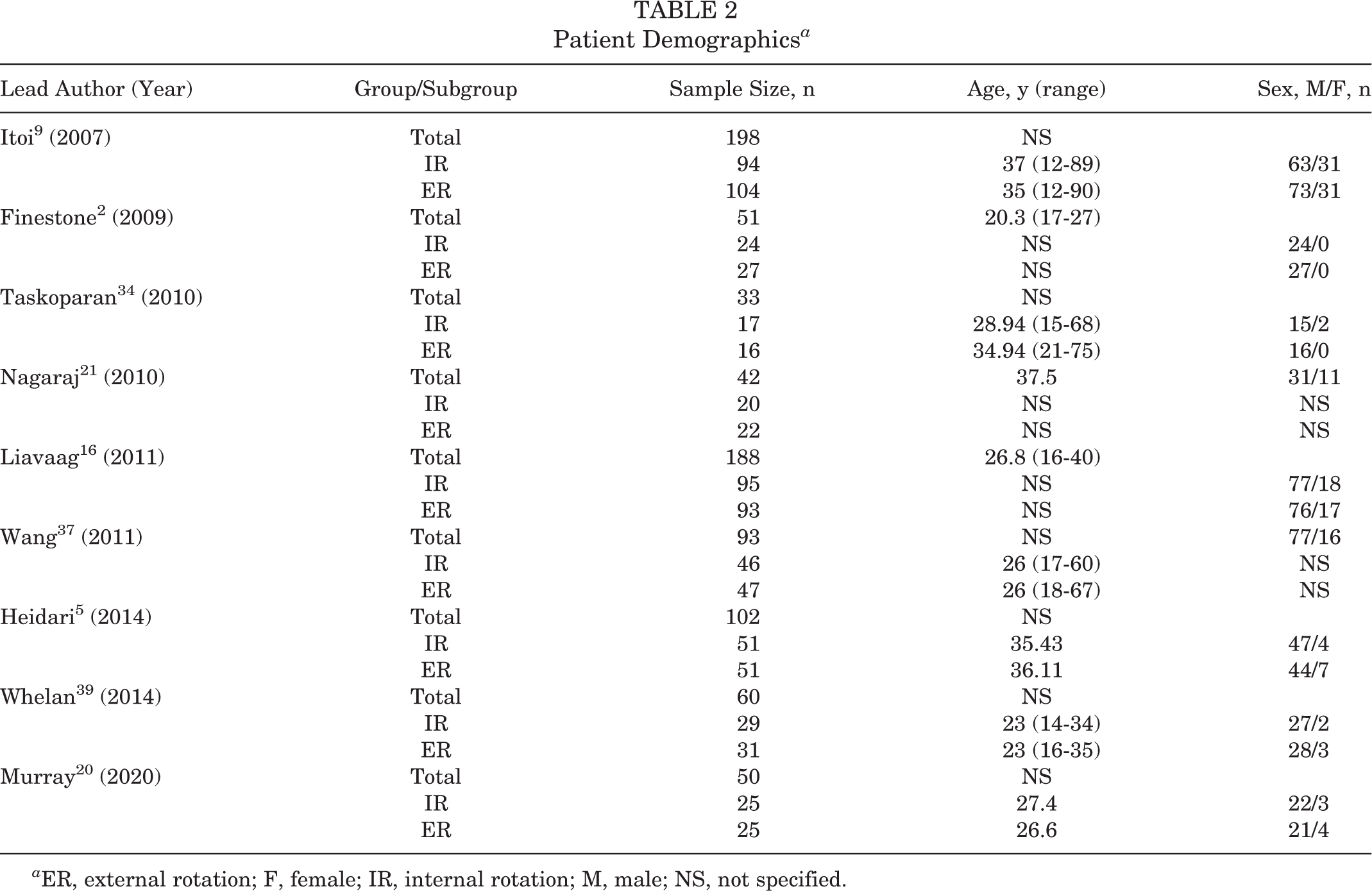
a ER, external rotation; F, female; IR, internal rotation; M, male; NS, not specified.
Characteristics of Included Studies a

a Abd, abduction; ER, external rotation; IR, internal rotation; NA, not available.
Characteristics of Included Studies
The current meta-analysis included 5 RCTs, 5,9,16,20,39 1 quasi-RCT, 34 and 3 studies 2,21,37 that could not be distinguished as RCT or quasi-RCT. Overall, 817 patients were included and divided into 2 groups: 416 patients immobilized in ER and 401 patients immobilized in IR. There were 668 male and 149 female patients, and the mean age of patients ranged from 20.3 to 37.5 years. We noted that 5 studies 2,5,9,16,20 had a minimum 24-month follow-up, 1 study 39 entailed more than 12 months of follow-up, 1 study 34 had more than 6 months of follow-up, and the remaining 2 studies 21,37 were without description. Regarding these 2 studies, Nagaraj et al 21 included 31 male and 11 female patients with a mean age of 37.5 years, and Wang et al 37 included 77 male and 16 female patients with a mean age of 26 years. The duration of immobilization ranged from 3 to 4.5 weeks in all studies. In 6 studies, patients were allowed to remove the brace when showering and changing clothes. One study included patients who used the brace more than 16 hours per day. 16
Outcomes
The overall recurrence rate of the 9 pooled studies was 28.0% (214/763). The recurrence rate was 21.5% (84/390) in the ER group versus 34.9% (130/373) in the IR group. The risk ratio of the ER group relative to the IR group was 0.56, which was statistically significant (P = .007) (Figure 3). This means that the relative risk reduction of recurrent instability with use of ER immobilization was 44% compared with IR immobilization.

Forest plot of the recurrence rate between immobilization in external rotation (ER) versus internal rotation (IR) at all ages. The risk ratio of the ER group relative to the IR group was 0.56, which was statistically significant (P = .007). Each square represents 1 study, and size expresses weight of the study in this meta-analysis. Horizontal lines show the 95% CIs for each study. The vertical line shows no differences between immobilization in ER and IR. The diamond represents the risk ratio, and its width represents the 95% CI. M-H, Mantel-Haenszel.
WOSI scores were reported in 4 studies, and 3 of the studies 5,16,39 showed the mean value and standard deviation, whereas 1 study showed only the mean values 21 (Table 4). Using the former 3 studies, 5,16,39 we analyzed the effect of immobilization position on the WOSI score and found no statistically significant effect (P = .54) (Figure 4).

Forest plot of the Western Ontario Shoulder Instability Index (WOSI) scores between immobilization in external rotation versus internal rotation. Immobilization position had no significant effect on the WOSI score. IV, inverse variance.
Recurrence Rate of Shoulder Dislocation and the WOSI Score a
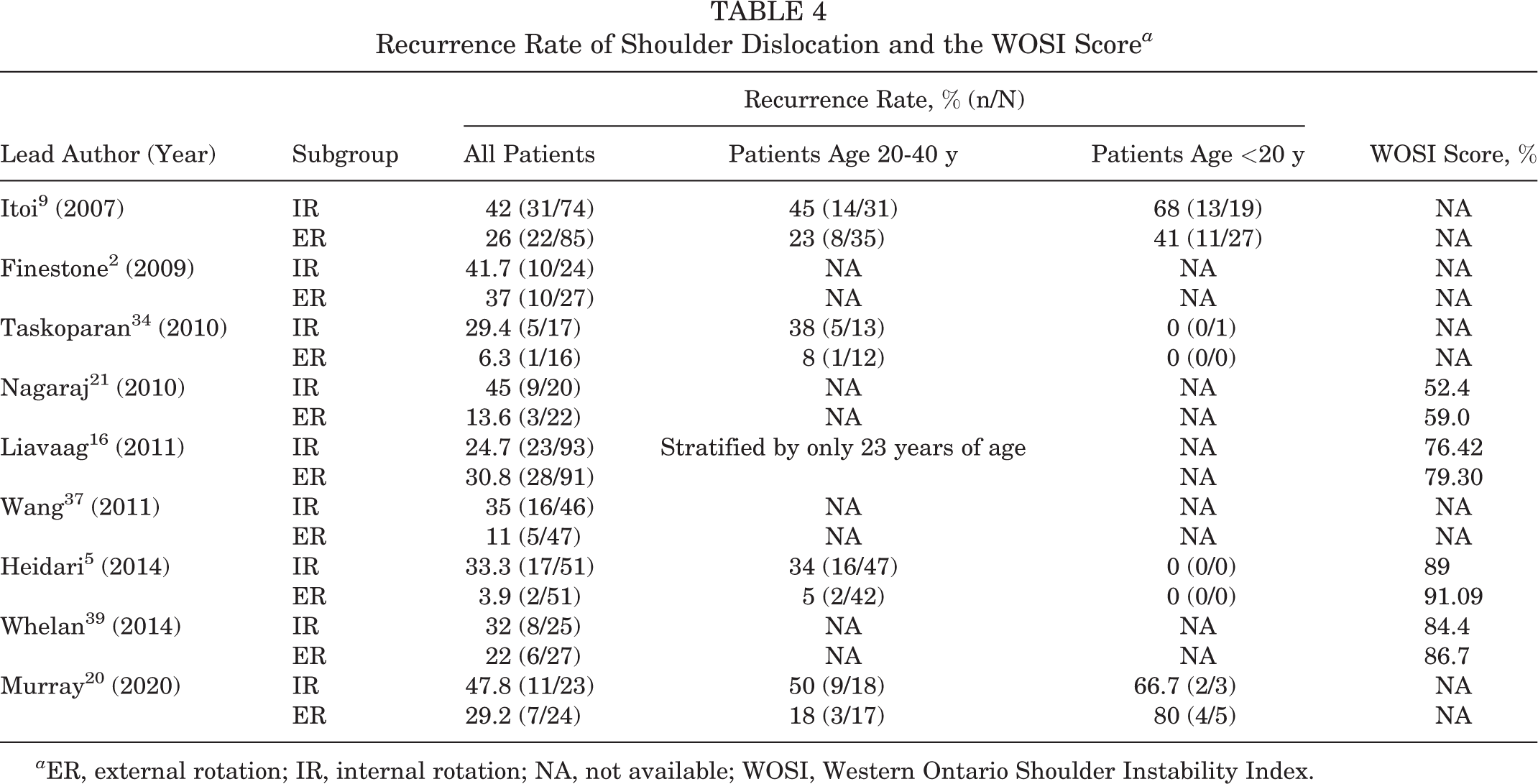
a ER, external rotation; IR, internal rotation; NA, not available; WOSI, Western Ontario Shoulder Instability Index.
Subgroup Analyses: Stratified by Immobilization Period, Age, and Follow-up Duration
In 1 study, patients who wore the brace for more than 16 hours per day were considered compliant. 16 In 2 studies, no information was provided regarding the time of brace application per day. 21,37 After we excluded these low-compliance or unknown-compliance studies, the remaining 6 studies 2,5,9,20,34,39 (in which patients wore the brace full-time except when showering or changing clothes) demonstrated significant differences between ER and IR groups (P = .01) with a 0.57 risk ratio for ER immobilization (Figure 5).

Forest plot of patients with full-time brace application. External rotation immobilization had a significant effect on recurrence rate, with a risk ratio of 0.57 (P = .01). M-H, Mantel-Haenszel.
Further subgroup analyses were performed without the low-compliance or unknown-compliance studies. In 4 studies, 5,9,20,34 outcomes of nonsurgical treatment were described in patients aged 20 to 40 years and those younger than 20 years. In the 20- to 40-year cohort, the recurrence rate was significantly lower in the ER group than the IR group (P < .0001) (Figure 6). The risk ratio of immobilization in ER was 0.32, and the relative risk reduction of ER immobilization was 68% compared with IR immobilization. In contrast, no significant differences in recurrence rate were seen between ER and IR immobilization in the cohort younger than 20 years (P = .44) (Figure 7). We noted a significant effect of age on the outcome of ER immobilization (P = .01).

Forest plot of the recurrence rate between immobilization in external rotation versus internal rotation in patients aged 20 to 40 years. A significant effect of ER immobilization was observed in this cohort (risk ratio, 0.32; P < .0001). M-H, Mantel-Haenszel.

Forest plot of the recurrence rate between immobilization in external rotation versus internal rotation in patients younger than 20 years. No significant effect of immobilization position was observed in this cohort (risk ratio, 0.77; P = .44). M-H, Mantel-Haenszel.
Among 4 studies 2,5,9,20 with more than 24 months of follow-up after primary shoulder dislocation, the recurrence rate was 21.9% (41/187) in the ER group and 40.1% (69/172) in the IR group. The risk ratio of ER immobilization was 0.56 compared with IR immobilization, which was statistically significant (P = .04) (Figure 8).
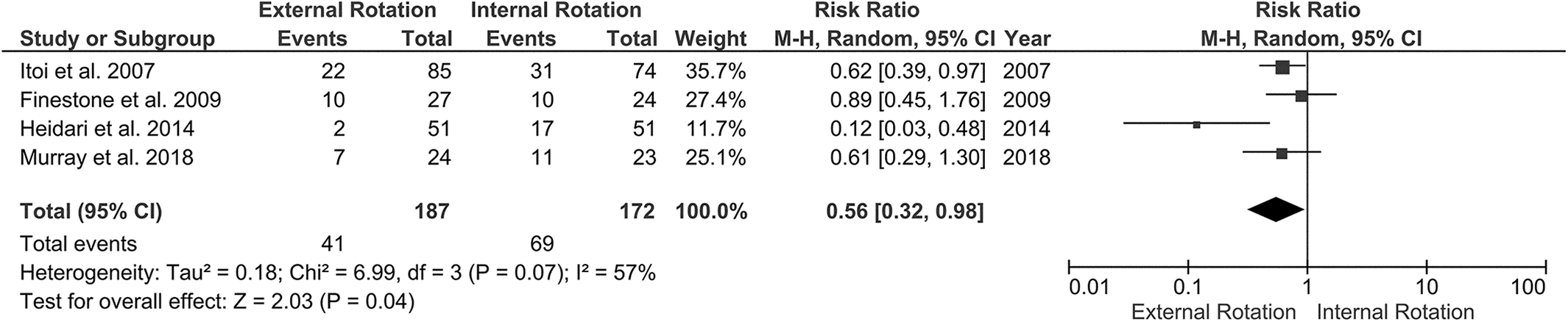
Forest plot of patients with more than 24 months of follow-up. External rotation immobilization had a significant effect on reducing the recurrence rate compared with internal rotation immobilization (risk ratio, 0.56; P = .04). M-H, Mantel-Haenszel.
Discussion
Several meta-analyses regarding arm immobilization for patients with primary anterior shoulder dislocation have been reported; however, the efficacy of immobilization in ER compared with IR remains controversial. Some meta-analyses demonstrated significant effects of ER immobilization in reducing the recurrence rate, 18,24,32 whereas others demonstrated no significant effect. 3,13,17,36,38 We adopted the literature search method used in a recent meta-analysis. 38 Subsequently, we added 3 RCTs that had not been included in the previous studies 20,21,37 and could update the outcomes of the meta-analysis. The current meta-analysis including 9 RCTs has demonstrated that ER immobilization reduces recurrence rate by 44% compared with IR immobilization. The positive conclusion of our study seems to be influenced by the most recent RCT with positive outcomes. 20 More RCTs are needed to determine the true efficacy of this treatment.
During nonsurgical treatment, it is imperative to reduce the detached labrum back to the glenoid and keep it reduced until healing occurs. For that purpose, keeping the arm in ER is extremely important. In most studies, patients kept their arms in ER almost all day, except when they showered or changed clothes. Liavaag et al, 16 however, considered patients who maintained immobilization for more than 16 hours per day as compliant. We believe that if a patient immobilizes the arm for 16 hours per day but moves the arm freely during the remaining 8 hours, reduction of the lesion will not be maintained and the lesion will not heal. In 2 other studies, information regarding immobilization time per day was lacking. 21,37 Excluding these 3 low-compliance or unknown-compliance studies, we found that heterogeneity was much lower in this subgroup of 6 studies (P = .15; I2 = 39%) than in all 9 RCTs (P = .01; I2 = 60%). This result clearly indicates that wearing the brace full-time is crucial when it comes to immobilization.
Several authors have reported that 3 weeks of immobilization after primary shoulder dislocation may be necessary. 9,25,30 ER immobilization for 3 weeks has proven to be effective in reducing the detached labrum back to the glenoid in previous magnetic resonance imaging (MRI) studies. 10,25,30 Also, no difference was seen in reduction and healing of the Bankart lesion between those immobilized for 3 weeks versus 5 weeks. 30 Thus, there seems to be a consensus as to how long the shoulder should be immobilized, if immobilization is to be applied.
What makes this treatment less popular among doctors is the issue of compliance. Keeping the arm in ER is less comfortable for patients compared with the conventional position of IR. 4 In addition to the discomfort of brace application, the position of the arm in ER immobilization is problematic (the arm “sticks out” from the body). Because of this unusual position, patients may report that they have to walk sideways to go through a narrow doorway, they occupy too much space on a crowded train, and so on. In a previous study, to avoid these problems, we used a brace that allowed patients to extend their elbow while keeping the shoulder in ER. 9 Extending the elbow makes the immobilization position less space occupying and thus makes this treatment more comfortable for patients and more acceptable for doctors.
Patient age is known to be an important risk factor for recurrence after primary anterior shoulder dislocation. 8,31 Previous meta-analyses comparing data stratified by patient age concluded that immobilization in ER did not provide clinical benefit regardless of patient age. 17,36 Recently, Murray et al 20 reported that immobilization in ER reduced the recurrence rate in patients aged 20 to 40 years. Pevny et al 26 reported that among patients older than 40 years, 35% had a rotator cuff tear and 4% developed recurrent instability after primary shoulder dislocation. This finding indicates that patients older than 40 years differ from those younger than 40 in terms of recurrent instability and pathologic conditions. To compare different age groups with similar pathologic conditions, we performed a subgroup analysis of patients aged 20 to 40 years who were believed to have similar conditions to patients younger than 20 years. In this subgroup analysis, we found a significant effect of ER immobilization in reducing the recurrence rate. Even in patients with similar conditions, efficacy of ER immobilization was observed only in those aged between 20 and 40 years.
There are several possible explanations for this finding. First, we know that age is a significant risk factor for recurrent instability, 12,15,31 even after surgical stabilization. 1 Patients aged 20 to 40 years revealed a significant effect of ER immobilization. Our interpretation is that they had a greater chance of tissue healing after ER immobilization. Age as a risk factor may have had a negative impact on this healing process in patients younger than 20 years. Second, only 2 studies were available for subgroup analysis of patients younger than 20 years. A relatively small number of patients might have caused a type II error. Third, we believe that the levels of sports and occupational activities and/or sex might influence the recurrence rate, according to previous literature. 8,12,22,23,33 Further analyses with an increased number of RCTs could provide detailed and accurate factors in addition to the arm position for immobilization.
Among the 9 studies used for the current analysis, 1 study assessed patients with minimal follow-up duration of 6 months after initial treatment. 34 However, as the previous meta-analyses adopted the same inclusion criterion regarding the follow-up duration, 3,17,18,36,38 we followed the previous studies for comparison. At the same time, because we appreciate the importance of minimum 2-year follow-up, we further analyzed the data based on a follow-up of more than 24 months. After we excluded 3 low- or unknown-compliance studies, this subgroup analysis showed a significant effect of ER immobilization on reducing the recurrence rate. Given that the longer the follow-up period the higher the recurrence rate, 7,11 we need more long-term follow-up studies to confirm the efficacy of this treatment.
This meta-analysis had several limitations. First, EMBASE was not included in our database search because it was not available in our institution. Second, we could not separately analyze the data on intention-to-treat analysis and per-protocol analysis because they were not necessarily provided. Third, only 2 studies routinely assessed the labral tear using MRI or magnetic resonance arthrography. 20,34 The remaining 7 studies did not mention the status of the labrum. We strongly believe that more high-quality RCTs are necessary to determine the true efficacy of this immobilization.
Conclusion
This meta-analysis demonstrates that ER immobilization reduces the recurrence rate after primary shoulder dislocation compared with IR immobilization in patients older than 20 years.
Footnotes
Final revision submitted October 14, 2019; accepted October 25, 2019.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.