
Abstract
Background:
Tibial-sided graft fixation is thought to be critical for the success of anterior cruciate ligament (ACL) reconstruction. Nevertheless, little is known about the graft force after fixation during the first 24 hours after surgery or the influence of screw diameter and length during this time.
Purpose:
To investigate the force, over the course of 24 hours, in soft tissue grafts secured with a tibial interference screw and to evaluate the effect of different screw diameters (7, 8, and 9 mm) and lengths (25 and 30 mm) on the force in these grafts.
Study Design:
Controlled laboratory study.
Methods:
Quadruple-strand flexor tendon grafts were fixed with bioabsorbable interference screws in 60 porcine tibiae. Grafts were pretensioned at 80 N over 10 minutes, and screws were inserted outside-in while a preload force of 80 N was applied. Different screw lengths (25 and 30 mm) and diameters (7, 8, and 9 mm), resulting in 6 groups with 10 specimens each, were tested. After release of the preload, graft force was recorded over 24 hours.
Results:
A significant decrease in graft force progressed in all groups over the 24-hour period. In total, a median loss of 75 N (IQR, 68-79 N) compared with the initial loading force was observed. Compared with the loading force of 80 N, this corresponded to a median loss of 91%. No significant differences in the remaining graft force could be found among the 6 different screw length and diameter groups after 10 minutes, 100 minutes, or 24 hours.
Conclusion:
Graft force in soft tissue grafts secured with a tibial interference screw decreased substantially over the first 24 hours after fixation. Neither the screw diameter nor the screw length affected the decrease in graft force. This raises substantial questions regarding the remaining fixation strength in vivo.
Clinical Relevance:
It should not be expected that ACL reconstruction can mechanically restabilize an injured knee as would an intact ACL. Reconstructed knees should be protected from mechanical overload in the early postoperative period.
In anterior cruciate ligament (ACL) reconstruction, fixation of the graft to the bone tunnel represents a weak point of the ACL construct, especially in the immediate postoperative period. 16,29,47 Bioabsorbable interference screw (BIS) fixation is a commonly used method for securing grafts to tibial bone tunnels. 4,12,16,25,41 Tibial fixation is considered to be the “weak link” in the immediate postoperative period due to the relatively low bone density and the angle at which force is applied to the graft attachment. 6,31 Decreasing graft force due to fixation failure equate with a loss of fixation strength. This may result in postoperative knee laxity and limited clinical success. 11 Therefore, knowledge about the intra-articular graft force in the early postoperative phase is important for a secure graft fixation.
Biomechanical studies have shown significant decreases in the initially set loading force of the grafts despite adequate pretensioning. 41 The reported decrease in graft force varies according to the time of the measurement (15 minutes, 30 minutes, 60 minutes, and 4 hours after fixation) and the type of graft used (isolated double-strand semitendinosus and gracilis grafts, bone–patellar tendon–bone grafts, and quadrupled hamstring ACL grafts). The decrease in graft force ranges between 49% and 78% over a maximum of 4 hours. 10,14,15,22,41 To our knowledge, mechanical evaluations of the ACL fixation strength over longer periods have not been published thus far. The early postoperative period after fixation is known to be a vulnerable phase. Regarding the time-dependent viscoelastic behavior of soft tissue grafts, a 24-hour postfixation measurement would be a reasonable amount. 54
The effects of different screw diameters 7,24,28,33,38,39,50,60 and lengths 5,19,20,24,49,52,53,60 on tibial ACL fixation have been evaluated, with controversial results, but only at time zero and without analysis of the postfixation resting period. Thus, little is known about the influence of these parameters during the first 24 hours after fixation, which is a critical phase. Especially in the early postoperative period, patients are in danger of uncontrolled knee movements during awakening from anaesthesia due to reoval of the endotracheal tube or exaggerated postoperative pain.
According to the current literature, it is not clear whether the graft fixation strength reaches a plateau at a certain level after the initial decline or whether it continues to decrease. Furthermore, it is unclear whether the diameter or the length of the interference screw has any effect on this progression.
Therefore, the purpose of this mechanical study was 2-fold. The first specific aim was to determine the development of intra-articular graft fixation strength over 24 hours. The hypothesis was that after the initial loss of intra-articular graft force in the first 4 hours, there would be no further decrease over the first 24 hours after interference screw fixation.
The second aim of this study was to assess the influence of different screw diameters and screw lengths on the graft fixation strength in the first 24 hours after interference screw fixation. The hypothesis was that larger screw diameters and screw lengths would show significantly higher intra-articular graft force after 24 hours. The present study conducted graft force (N), not tension (N/m2), measurements.
Methods
A total of 60 fresh porcine cadaveric limbs were obtained from a local butcher. Superficial flexor digitorum tendons were initially harvested from the porcine cadavers and cleared of adherent muscle fibers and surrounding soft tissues. Subsequently, all soft tissue was removed from the tibia. All tendons and tibiae were packed in moist saline dressings and frozen at –20°C in sealed plastic bags. At 24 hours before testing, the tendons and tibiae were thawed at room temperature. 36,45,61 All specimens were kept moist with 0.9% saline during the specimen preparation, fixation, and biomechanical testing procedures. The tendons were shortened to a length of 240 mm, and the ends were sutured using a whipstitch technique, analogous to the technique used in human ACL reconstruction. Then, the tendons were folded 2 times into 4 strands, resulting in a graft length of 60 mm. The grafts were trimmed to a diameter of 8 mm. A sizing tube with 0.5-mm increments was used to check the diameter of the prepared grafts.
Tibiae were embedded in custom-made metal tubes through use of the 2-component plastic Memecryl (Bauer Handels GmbH). The fibula and interosseous membrane remained connected to the tibia to stabilize the bone complex and ease orientation. After the Memecryl hardened, a guide pin for the tibial tunnel was placed using a drill guide (Acufex Drill Director; Smith & Nephew) set at 65°. The aperture of the tibial drill tunnel was positioned at the center of the native ACL insertion. The bone tunnel started extra-articularly at the anteromedial tibial cortex, 1.4 cm medial to the tibial tubercle. 37 The tunnel length was set at approximately 40 mm. 8,63 The tunnel was drilled with increasing drill-bit diameters (6- and 7-mm diameter) until it was expanded to match the 8-mm diameter of the quadrupled soft tissue graft. The bone tunnel and graft diameter were set equally following the recommendations of Steenlage et al. 56 Subsequently, overlapping soft tissue on the tibial tunnel was safely removed for easy passage of the graft. The embedded tibia was securely mounted to the custom-made mechanical testing machine to apply the initial tension force parallel to the long axis of the graft and bone tunnel (Figure 1).

Experimental setting: (1) force sensor, (2) embedded tibia with graft, (3) screwdriver during screw insertion, (4) custom-made mechanical testing machine, (5) pretensioning device.
Before biomechanical testing, each quadruple-strand hamstring graft was pretensioned for 10 minutes starting at 80 N to simulate tensioning on a graft board. Directly after preconditioning, the looped end of each graft was placed through the bone tunnel with 30 mm protruding from the proximal aperture of the tunnel. Therefore, the 6-cm hamstring graft was divided into an intra-articular portion of 30 mm and a tibial tunnel portion of 30 mm. 8,49,65 The looped part of the graft was attached to a shackle bolt and connected to the force sensor. Intra-articularly, the graft was positioned at the angle of the physiological anteromedial bundle of the ACL (47.9° sagittal, 73.8° coronal to tibial level) (Figure 2). 55
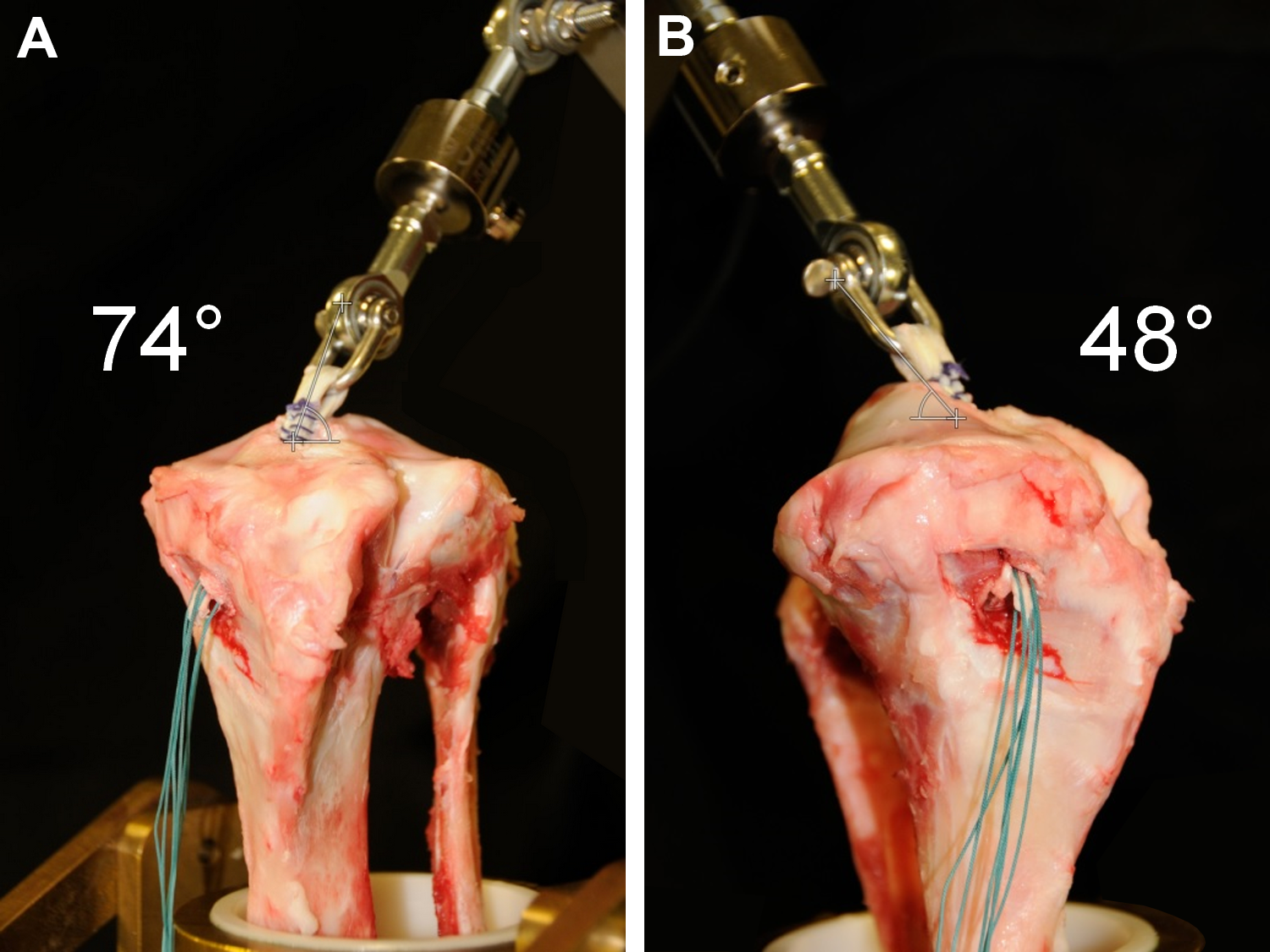
Diversion of anterior cruciate ligament graft (A) coronally and (B) sagittally to tibial level.
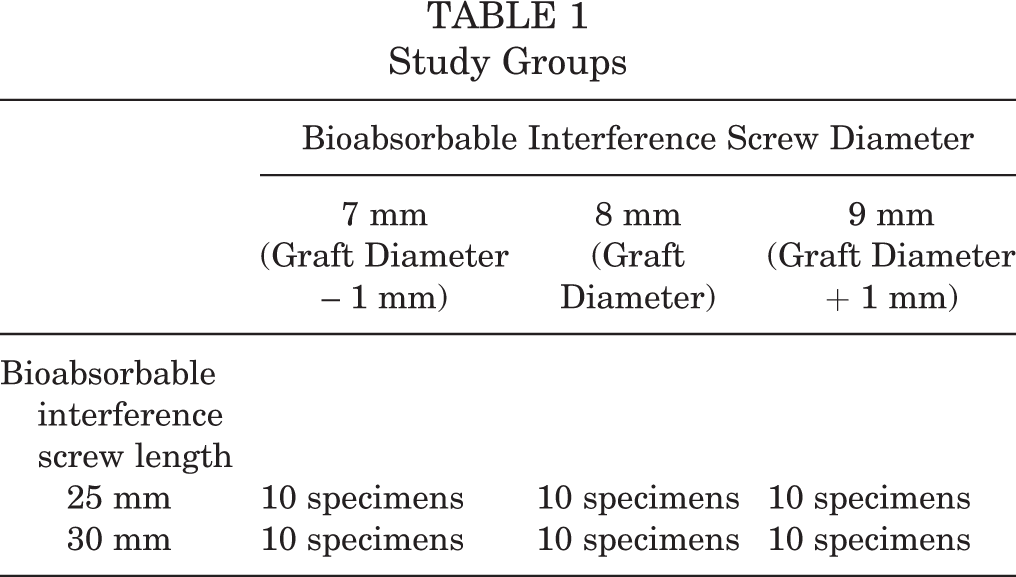
After graft insertion, at the distal end of the graft, an initial load of 80 N was applied along the long axis of the bone tunnel as recommended in previous studies. 27,64 A bioabsorbable interference screw (BioactIF Osteotrans; Richard Wolf GmbH) was manually inserted in an outside-in fashion anterior to the tendon according to the manufacturer’s recommendations. Samples were randomly assigned to 1 of 6 groups through use of randomization.com to evaluate the influence of the different screw lengths (25 and 30 mm) and screw diameters (7, 8, and 9 mm) on the graft force over 24 hours. In each group, 10 specimens were tested (Table 1). During screw insertion, the initial load of 80 N was maintained. 27,64
Study Groups
Immediately after screw insertion, the sutures applying this initial load were cut. Intra-articular force in newtons was recorded from application of the initial load before screw insertion and up to 24 hours after suture cutting. Data were recorded at 5 Hz using the data acquisition system spider3 (HBM) and measuring software Catman 4.5 (HBM). To reduce the extent of data and still register the expected massive loss of force in the first minutes after fixation, data recording proceeded in 2 phases. Phase 1 consisted of continuous data acquisition for 10 minutes. In phase 2, the measuring occurred periodically for 60 seconds at 10-minute intervals. Specimens were kept moist with 0.9% saline during the entire testing period with a specially designed moisturization device (Figure 3).

Moisturization device.
For statistical analyses, the recorded forces for the different screw lengths and diameters were compared with each other at 5 time points: Before application of the initial loading tension At the moment of cutting the sutures After 10 minutes After 4 hours After 24 hours
Time points were chosen to adequately evaluate the graft behavior during screw insertion (time points 1 and 2), such as during the well-studied early phase (10 minutes), the maximum measurement period published so far (4 hours), and after a full 24-hour period.
The D’Agostino-Pearson omnibus normality test was used to verify the non-Gaussian distribution of all data. To determine whether there was a proceeding decrease in tension loss after the first 100 minutes, we used the nonparametric Wilcoxon matched-pairs signed rank test. When assessing the differences between the groups at the relevant time points, we analyzed the data using the Friedman nonparametric 2-way analysis of variance and the Tukey multiple comparisons test as a post hoc test.
Data are presented in box plots showing the median, the interquartile range (IQR) (25%-75%), and the 5th and 95th percentiles as whiskers. All statistical analyses were performed using GraphPad Prism version 6.01 (GraphPad Software). A P value < .05 was considered significant in 2-group comparisons and adjusted in multiple-group comparisons.
Results
A significant increase in graft force was seen after interference screw insertion (Figure 4). The initially applied load of 80 N increased by a median of 14 N (IQR, 2-25 N) (P < .0001). We found no significant differences in graft force after screw insertion between the groups when comparing screw length and diameter.

Gain of intra-articular graft force through interference screw insertion presented as box plots with the median, interquartile range (25%-75%), and whiskers (5%-95%). *Statistically significant (P < .0001).
The initially applied load showed a significant decrease of a median of 79 N (IQR, 73-86 N) in all groups in the first 4 hours after fixation. The decrease in graft force significantly progressed in all groups up to 24 hours after fixation by a median of 49% (IQR, 40%-63%) compared with the force at 4 hours (Table 2).
Graft Force a

a Graft force is expressed in newtons as median (25%-75% interquartile range).
In total, over the 24 hours after interference screw fixation, we observed a median loss of 75 N compared with the initial loading force of 80 N. This corresponded with a median loss of 91% and a total percentage change between 89% (9 × 30-mm screw group) and 94% (8 × 30-mm screw group) compared with the initial loading force over the 24 hours after fixation (Figure 5).
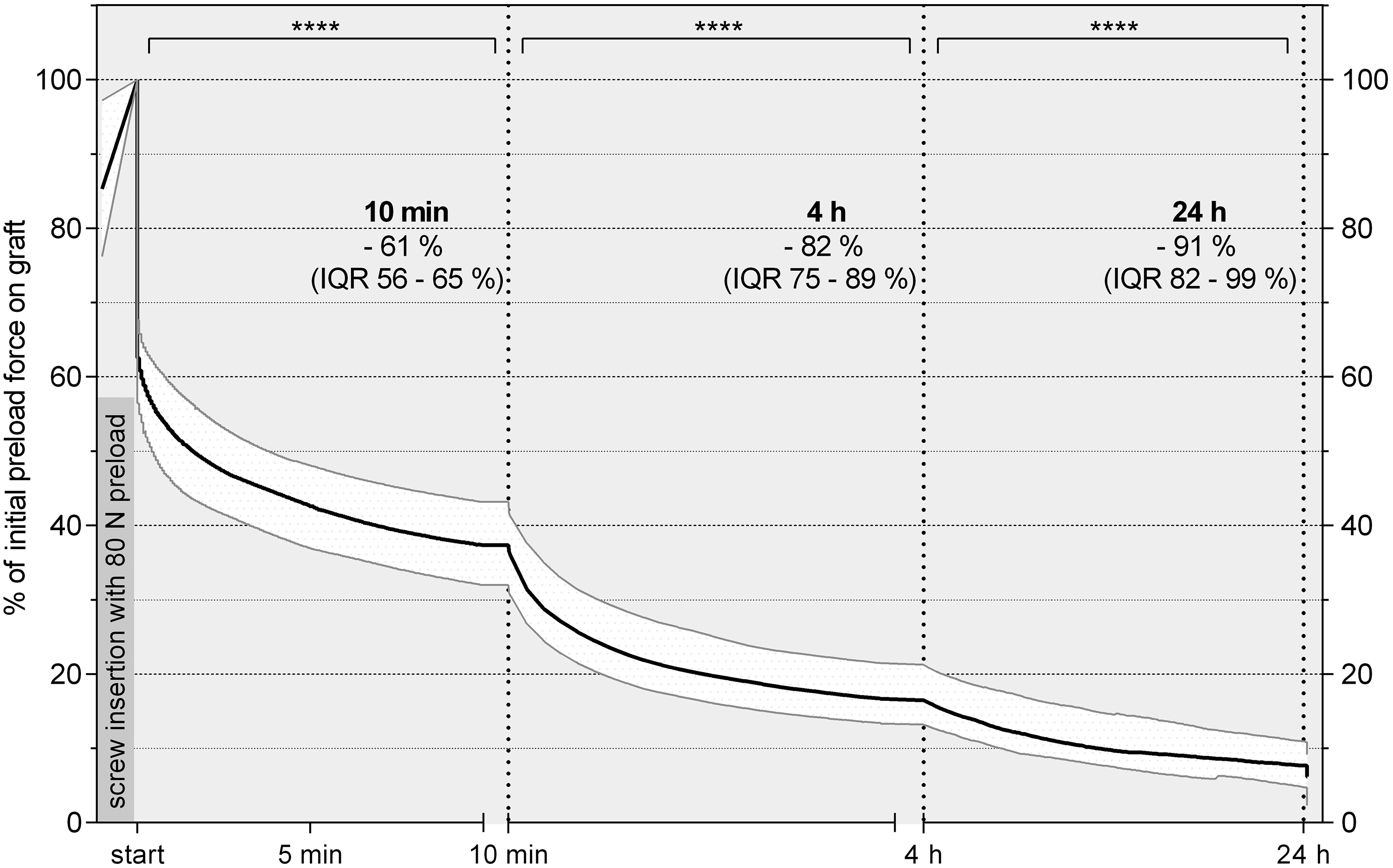
Percentage decrease in graft force for all groups over the first 24 hours after fixation presented as a curve with the median line and interquartile range (IQR) (25%-75%). ****Statistically significant (P < .0001). Initial preload force after screw insertion was considered to be 100% graft force.
Screw diameter and length did not influence the remaining graft force at the investigated time points. No significant differences were seen among the 6 groups after 10 minutes, 100 minutes, or 24 hours. The results of the force measurements for the different screw designs are demonstrated in Table 2. Comparing screws 25 mm and 30 mm in length, we found no significant differences in the remaining graft force. No significant differences were seen in the remaining graft force among screws 7 mm, 8 mm, or 9 mm in diameter (Figure 6).

(A) The remaining graft force after 100 minutes and 24 hours for different screw diameters presented as box plots with the median, interquartile range (25%-75%), and whiskers (5%-95%). No significant differences among the groups at the same time points could be observed. (B) The remaining graft force after 100 minutes and 24 hours for different screw lengths presented as box plots with the median, interquartile range (25%-75%), and whiskers (5%-95%). No significant differences among the groups at the same time points could be observed.
Discussion
The most important finding of this study was that the intra-articular graft force continuously decreased over the initial 24 hours when tibial interference screw fixation of soft tissue grafts was used. The measured 91% median decrease occurred irrespective of screw diameter and length.
In the current literature, biomechanical studies have shown significant decreases of as much as 78% of the initially set load force of hamstring ACL grafts fixed with interference screws. Studies investigating this progress have been limited to a time period between 15 minutes and 4 hours. 10,14,15,23,41 In contrast, the present study demonstrated further progression in the loss of the initial applied fixation load. Despite numerous previous studies describing a relevant decrease in graft force in a relatively short time, the amount of loss after 24 hours, as observed in the present study, was remarkable. The results of this study with a comparatively long measurement period appear to be clinically meaningful for the early postoperative rehabilitation phase after ACL reconstruction.
The impressive early loss of intra-articular graft force may have occurred because of (1) a failure at the bone, graft, and screw interface (slippage effect) or (2) an elongation of the graft. 41 With regard to the inferior effect of the screw that was used, a loss of graft tension due to elongation and not a loss of fixation strength due to poor fixation appears to have the major effect on the measured force after 24 hours.
Regarding the decrease in graft force in the first minutes after fixation, careful consideration should be taken in the process of applying backup fixation methods. The results of this study indicated that if backup fixation is used, the device should be attached quickly after screw insertion to minimize decreased graft force. 48
The measured 91% decrease in intra-articular graft force may have indicated frequent mild knee laxity in the early postoperative phase after ACL reconstruction. This is consistent with earlier in vivo sheep 59 and human patient measurements. 35 However, clinical studies have reported good long-term functional scores and knee stability with the use of interference screw fixation. 32,46,57
Currently, surgeons use a range of initial tensioning methods during surgery for optimal restoration of knee joint stability. It is commonly assumed that insufficient graft tension results in increased anteroposterior laxity of the tibiofemoral joint and that excessive graft tension limits the range of motion. This might lead to an overconstrained knee and negatively affect knee joint kinematics, leading to a higher risk of cartilage degeneration in the long term. 2 Existing evidence has suggested that there may be a relatively wide range of safe and acceptable ACL graft tensions for achieving optimal outcomes. 2,64 Regarding the observed early postoperative loss of fixation strength and generally excellent clinical results, the need for graft tensioning and maintaining loads around 80 N on the graft may be overstated.
In this study, a preconditioning protocol similar to that used in clinical practice was applied. Despite numerous studies describing the positive effects of tendon preconditioning, there is still no consensus on an optimal treatment protocol and no evidence for beneficial clinical outcomes of specific protocols. Several studies indicated reduced knee laxity by objective measurements of the outcomes when using a pretensioning protocol with static loading of approximately 80 N. 3,17,26,64 Therefore, Arneja et al 3 and Yasuda et al 64 suggested the application of 80-N pretensioning force during ACL reconstruction. The methodical procedure in the current study followed these recommendations.
Previous studies have demonstrated improved graft fixation strength for serial tunnel dilatation when soft tissue grafts and interference screw fixation were used. 9,51 Similar biomechanical experiments using porcine specimens have revealed no differences in maximum load-to-failure tests. 21,40 Differences in tunnel diameter, graft size, screw diameter, or screw materials may precipitate the discrepancy in these findings. 21 The aim of the present study was to assess the influence of different screw diameters while keeping the diameter of bone tunnel and tendon graft constant. Therefore, no tunnel dilatation was performed.
The current data suggest that the remaining force on the graft after 24 hours approached a limit. More research needs to be conducted to further determine the development of fixation strength beyond the 24-hour period. To improve simulation of the human knee after ACL surgery, a temperature increase should be considered, as it might trigger an additional decrease in intra-articular graft force. 10,15
Furthermore, this study assessed the influence of different screw diameters and lengths on intra-articular graft force. However, no significant differences were found. Consequently, in this experimental setting, different screw diameters and lengths did not influence the intra-articular graft force. This result was obtained by use of a single fixation device and single graft type. Additional fixation devices or graft types may have varying outcomes. The design of this study focused on soft tissue grafts as well as tibial-sided interference screw fixation, because it is commonly used for ACL reconstruction. 18,30
This study has some limitations. Despite continuous moistening of the graft and the related bone region, the study design could not mimic the in vivo condition. The use of porcine material for biomechanical testing is widely accepted because its mechanical behavior and characteristics are similar to those of human tendons and bone. 17,34,43,62 Nevertheless, the translation of the results of such studies into clinical practice is controversial. Porcine flexor digitorum tendons have similar biomechanical properties, such as stiffness and high failure loads, compared with human hamstring tendons, and the elongation of porcine samples has been shown to be comparable with that of human hamstring tendons. 13,43 Considering that a maximum load-to-failure test was not performed, it seems reasonable to use porcine tendons because of the easy acquisition and the high comparability among cadavers.
The porcine tibia is commonly used for biomechanical evaluations because of its similar size, shape, and bone quality to the young human tibia. 1,44,58 Given the higher trabecular bone density, the porcine tibia can underestimate graft slippage and overestimate the failure load of the soft tissue graft in ACL reconstruction. 31,42 This may have affected the comparison of different BIS diameters and lengths.
Furthermore, this study focused on tibial ACL fixation with BIS. When different fixation devices (titanium interference screws, combination screw and sheath) or supplementary fixation (spiked washers, staple) is used, an overall decrease of graft force might be different from this experimental setting. Backup fixation methods could reduce the failure at the bone, graft, and screw interface (slippage effect), resulting in a less extensive decrease of graft force. Additional loss of graft force may occur with the femoral fixation device. In this experimental setting, only the tibial side was evaluated.
Conclusion
Graft force in soft tissue grafts secured with a tibial interference screw decreased substantially during the first 24 hours after fixation. Neither the screw diameter nor the screw length affected the decrease in graft force. This finding raises substantial questions regarding the remaining fixation strength in vivo. Thus, it should not be expected that ACL reconstruction can mechanically restabilize an injured knee as would an intact ACL.
Footnotes
Acknowledgment
The authors thank the Richard Wolf Company, which provided the screws used in this study, and the Charité–University Medicine Berlin for funding this study by an internal research fund.
Final revision submitted January 2, 2020; accepted January 22, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: The screws used in this study were provided by the Richard Wolf GmbH. S.K. has received speaking fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.