
Abstract
Background:
There is disagreement among team physicians, without conclusive evidence, as to when high-level athletes with a Jones fracture should be allowed to return to play after being treated operatively with an intramedullary screw.
Purpose:
To report our experience of early return to sport in collegiate athletes after intramedullary screw fixation of Jones fractures.
Study Design:
Case series; Level of evidence, 4.
Methods:
We identified all collegiate athletes with an acute fracture at the base of the fifth metatarsal treated by 1 of 2 orthopaedic surgeons with intramedullary screw fixation over a 22-year period (1994-2015), and we performed a retrospective review of their records. Fixation consisted of a single intramedullary screw. Athletes were allowed to bear weight as tolerated in a walking boot immediately postoperatively and return to play as soon as they could tolerate activity. Patients were contacted to complete patient-reported outcome scores that included the Foot and Ankle Ability Measure (FAAM) score, a brief survey specific to our study, and follow-up radiographs.
Results:
A total of 26 acute Jones fractures were treated in 25 collegiate athletes (mean age, 20 years; range, 18-23 years). Overall, the athletes returned to play at an average of 3.6 weeks (range, 1.5-6 weeks). Three screws were removed for symptomatic skin irritation. There was 1 refracture after screw removal that was done after radiographic and clinical documentation of fracture union, which was treated with repeat cannulated percutaneous screw fixation. One screw was observed on radiographs to be broken at 1 year postoperatively, but the fracture was healed and the athlete was playing National Collegiate Athletic Association Division I sports without symptoms and continued to play professionally without symptoms. Of 25 athletes, 19 completed the FAAM at an average follow-up of 8.6 years (range, 1.5-20.0 years). They reported scores of 94.9% (range, 70.2%-100%) for the activities of daily living subscale and 89.1% (range, 42.9%-100%) for the sports subscale. Follow-up radiographs were obtained, and no nonunion, malunion, or additional hardware complications were identified.
Conclusion:
Athletes with acute Jones fractures can safely be allowed to return to play after intramedullary screw fixation as soon as their symptoms allow, without significant complications. In our experience, this is usually within 4 weeks from injury.
The fifth metatarsal is the most commonly fractured metatarsal in the foot, comprising approximately 70% of all metatarsal fractures; such fractures are relatively common in young athletes. 22 Dr Robert Jones 10 first described fractures of the proximal aspect, or base of the fifth metatarsal, in 1902. The radiographic anatomy of the fracture is crucial for treatment decisions, as not all fifth metatarsal fractures are considered “Jones fractures.” Fractures can be classified using the Torg classification as follows: type I, fracture on the lateral aspect of the tuberosity, extending proximally into the metatarsocuboid joint; type II, Jones fracture, beginning laterally in the distal part of the tuberosity and extending obliquely and proximally into the medial cortex at the fourth and fifth metatarsal base articulation; and type III, fracture distal to the fourth and fifth metatarsal base articulation. Lawrence and Botte 14 also classified these fractures based on the zone of injury: proximal tuberosity avulsion fractures caused by excess inversion of the foot (zone I), metaphyseal-diaphyseal junction (zone II), considered true “Jones fractures,” and diaphyseal fractures, distal to the fourth and fifth metatarsal articulation (zone III). More recent studies 1,12 have included both zone II and zone III fractures when describing Jones fractures, as they have similar healing patterns, with a high risk of nonunion.
The delayed and decreased healing rates of zone II and zone III fractures are attributed to the anatomy of the blood supply of the fifth metatarsal. A “water-shed” area is present at the metaphyseal-diaphyseal junction, as the base of the metatarsal is perfused by metaphyseal arteries that enter at the base, whereas the nutrient arteries enter the proximal shaft and provide retrograde perfusion to the metaphyseal-diaphyseal junction. 24 To further complicate this matter, the nutrient artery that supplies the watershed area is often compromised by zone II and zone III fractures. 3,24 Athletes are especially susceptible and predisposed to nonunion and refracture because of the excessive repetitive stress the bone must endure. Kavanaugh et al 11 and DeLee et al 4 reported a high rate of delayed union or nonunion in athletes treated nonsurgically.
Intramedullary fixation in the treatment of Jones fractures is accepted among team physicians as the standard of care in elite athletes to optimize outcomes and expedite return to play. 2,5,7,9,12,17 A 2011 systematic review 26 reported that operative fixation with intramedullary screw fixation results in faster time to union and faster return to play with fewer complications compared with nonoperative management. Despite early surgical fixation and improvement in surgical techniques, the published nonunion and refracture rate of 4%-12% persists. 18,23 While it has become widely accepted that operative fixation facilitates an early return to sport, there is limited information on when an athlete is deemed ready to return to play without compromised fracture healing. Some authors 7,13,23 have hypothesized that surgical failure is the result of returning to vigorous activity too soon. However, even in studies 8,9,23,28 with prolonged protected weightbearing postoperative protocols, a high ratio of patients with nonunions and refractures was demonstrated. Controversy persists among physicians and sports medicine teams on the timing of return to play and the ideal postoperative protocol.
The purpose of this study was to report our experience of early return to sport in collegiate athletes after intramedullary screw fixation of Jones fractures.
Methods
Institutional review board approval was obtained for this study. A retrospective review of the injury database of 2 collegiate athletic programs treated by our practice was performed, and all patients with fifth metatarsal fractures from August 1994 through December 2015 were identified. Inclusion criteria were as follows: age ≥18 years, skeletal maturity, collegiate-level athlete at time of injury, surgical fixation with intramedullary screw, and a fifth metatarsal Jones fracture (Lawrence and Botte zone II and zone III, Torg III 27 ) as identified on anteroposterior (AP), lateral, and oblique radiographs. All operative fractures included in the study were complete, acute fractures as indicated radiographically; no stress reactions or stress fractures were treated operatively and included in this series. Individuals were excluded if they had a previous injury to the ipsilateral foot.
Return to play was defined as competing in intercollegiate competition (in-season athletes) or full participation in practice/training without limitations (out-of-season athletes). This was documented prospectively by athletic training staff in the National Collegiate Athletic Association (NCAA) injury database at the collegiate institutions. Certified athletic trainer records from each university were used to identify athlete characteristics, length of follow-up at the university, and any complications after surgical fixation.
Operative reports of all the included patients were reviewed. Details of fracture morphology, and implant details, including manufacturer, type (solid, cannulated, or variable pitch compression screw), and screw diameter, were recorded.
After the retrospective review, attempts were made to contact each patient to request new foot radiographs and participation in an online survey. The survey included the Foot and Ankle Ability Measure (FAAM), 16 which is divided into activities of daily living and sports subscales, as well as a brief questionnaire specific to our study (see Appendix).
Surgical Technique
All surgical procedures were performed by 1 of 2 authors (S.M. or L.B.). The surgical technique used by each surgeon was identical, although the implant of choice differed over the 23-year study collection period. All cases were performed utilizing a percutaneous intramedullary screw fixation under fluoroscopy guidance. After identification of the base of the fifth metatarsal and the fracture site, a small incision was made at the base of the fifth metatarsal at the intersection of the peroneus brevis and tertius tendon. Blunt dissection was used to create a soft tissue plane. A guide wire was then inserted to the tip of the base of the fifth metatarsal in line with the intramedullary canal in multiple planes. Placement was confirmed with AP, lateral, and oblique views. The wire was advanced across the fracture site down the intramedullary canal in a trajectory that would not penetrate the cortical bone. The canal was then prepared with drills and taps according to the technique of the specific implant chosen in each case, with a goal of placing a screw diameter large enough to adequately control the distal segment with evidence of torque on the fifth metatarsal shaft during tap and screw placement. A depth measurement was taken from the wire, and a screw of the appropriate length was selected to allow for the longest screw possible without hitting the far cortex when using variable pitch screws. For partially threaded screws, solid or cannulated, a screw length long enough to ensure that the threads would all be past the fracture site to achieve lag screw fixation was selected. Implants included standard AO cannulated screws (stainless steel; Synthes), variable pitch headless compression screws (titanium; Acumed), or solid Jones fracture–specific screw systems (titanium; Arthrex). Care was taken in all cases to obtain intramedullary fixation on AP, lateral, and oblique views, with adequate screw fixation distal to the fracture site.
Postoperative Protocol
Postoperative rehabilitation was divided into 5 phases, as outlined in Table 1. Patients progressed through each phase sequentially based on proper technique and tolerance of the additional workload. Rehabilitation was focused on ensuring the maintenance of proper gait, with gradual progression of workload while maintaining conditioning in anticipation of return to full participation. Throughout this process, the athlete was allowed to participate in all team weight-lifting sessions in a modified manner, to maintain upper and lower body strength. The time required to progress through each phase was athlete dependent, but it was generally 4-7 days. Of note, our protocol includes a bone stimulator to promote healing and decrease the recovery time in this challenging fracture pattern and patient population. Routine radiographs to document fracture healing were not routinely taken unless the athlete’s symptoms were not progressing and pain was not decreasing appropriately with attempted return to play or full training by 6-8 weeks postoperatively.
Postoperative Rehabilitation Protocol for Jones Fractures

Results
During the study period, 27 athletes were treated with surgical fixation of Jones fractures; however, 2 athletes were excluded based on previous injuries to the ipsilateral foot, giving a total study population of 25 athletes. One patient fractured both of his fifth metatarsals during his collegiate career, and therefore, a total of 26 fractures were included in this study. The study group was made up of 22 male and 3 female athletes, with an average age of 20 years (range, 18-23 years) and an average body mass index (BMI) of 28.4 (range, 21.6-38.7). The study sample consisted of 14 football players (56%), 2 basketball players, 7 soccer players (28%), 1 volleyball player (4%), and 1 tennis player (4%).
Surgical fixation was achieved with intramedullary screw fixation in all cases. Implants included 10 partially threaded cannulated screws, 13 cannulated variable pitch screws, and 3 solid screws. The screw type was chosen based on patient anatomy and surgeon preference and evolved over the 23 years of the study period. See Table 2 for details on screws utilized for fixation.
Screw Types

All study athletes returned to play within 6 weeks of surgery, at an average of 3.6 weeks (range, 1.5-6 weeks). In-season fractures made up 61% of the total. The average return to play for in-season injuries was 3 weeks (range, 2-4.5 weeks). Out-of-season athletes returned to full activity at an average of 4.6 weeks (range, 3-6 weeks). The breakdown of timing of return to play is displayed in Figure 1.
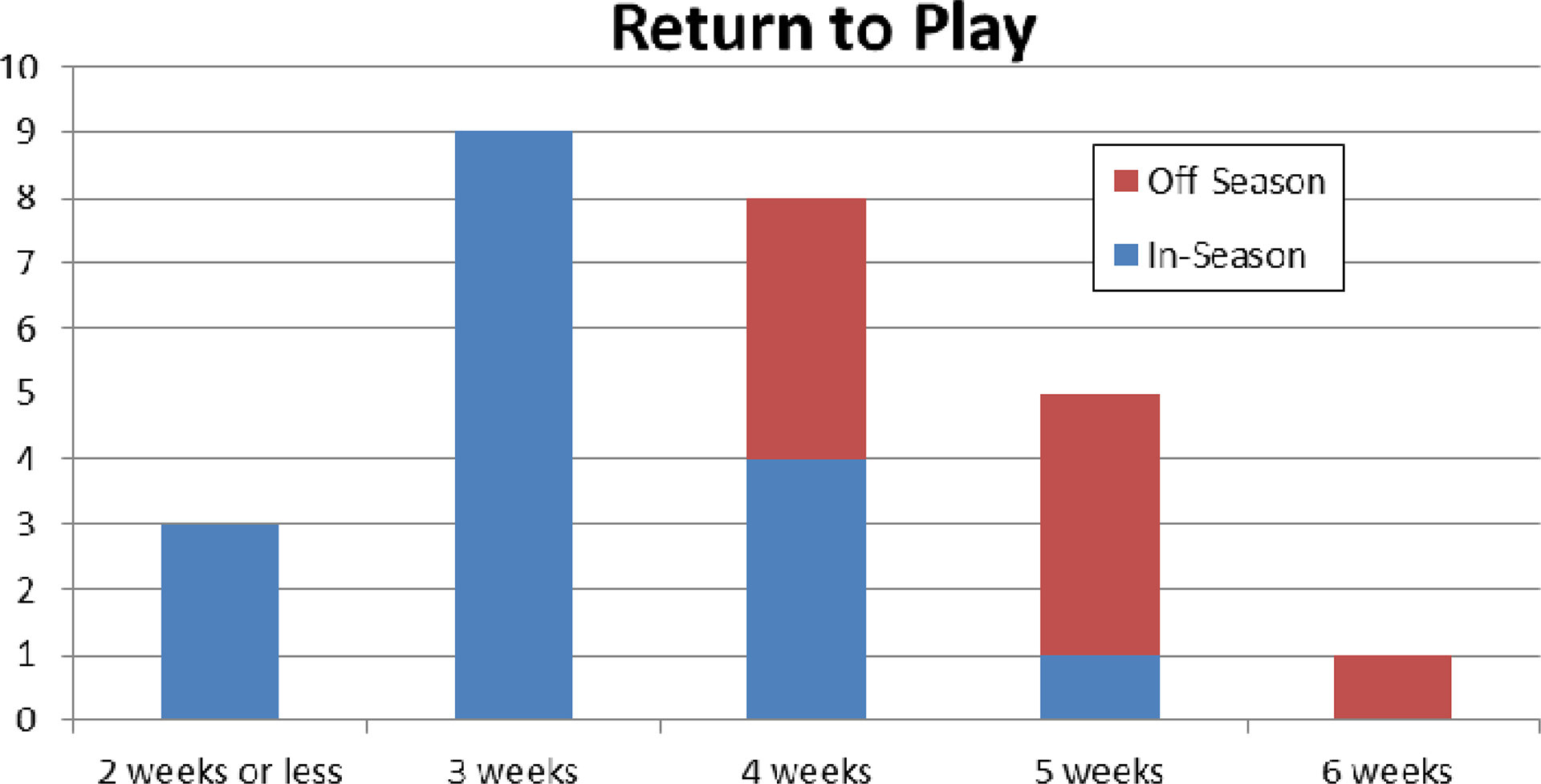
Number of athletes who returned to play by weeks after surgery. All midweek returns were rounded up to the nearest full week.
No surgical wound complications or infections were recorded. Zero nonunions or malunions were identified radiographically or reported symptomatically. Of the 26 screws, 3 (11%) screws were removed because of soft tissue irritation. All 3 screws were partially threaded cannulated screws with a standard head, and the surgeries were performed early in the study period (1990s), prior to current screw technology and the availability of fracture-specific screws. Only 1 athlete (4%) suffered a refracture. Six months after the initial surgery in this patient, the screw was removed because of soft tissue irritation. The athlete then refractured the same fifth metatarsal 1 year from the initial injury and was treated a second time with revision intramedullary surgical fixation, returning to play within 2 weeks of surgery. He participated in the study survey and reported no other problems with his foot in the 16 years since his surgery.
One 4.0-mm cannulated screw was incidentally identified as broken on an ankle radiograph at 1 year postoperatively, but on further foot imaging, the fracture was healed and the athlete was playing NCAA Division I basketball without lateral foot symptoms. We were unable to obtain an updated radiograph of this player during the study, but she was able to complete the FAAM study forms, where she reported minimal symptoms at 9-year follow-up (86% on the FAAM sports subscale and 100% on the FAAM activities of daily living subscale). In addition, this player has been playing professionally for 7 years and continues to be asymptomatic. The only other incidence of broken hardware was a 4.5-mm cannulated screw identified in the study follow-up, with bridging callous and no appreciable fracture line visible on the radiograph taken for study purposes at 12 years postoperatively. The patient had completed his athletic career without any significant further foot pain or limitations and reported FAAM scores of 100% on the sports subscale and 100% on the activities of daily living subscale. Table 3 summarizes the complications.
Complications (N = 26 Patients)

A total of 20 former athletes with 21 fractures (84% of the total fractures included) participated in the patient survey, imaging, or both. Nineteen athletes (76% of the total athletes included) completed the FAAM at an average follow-up of 8.6 years (range, 1.5-20 years). Patients scored an average of 94.9% (range, 70.2%-100%) for the activities of daily living subscale and 89.1% (range, 42.9%-100%) for the sports subscale. When participants were asked to rate their current level of function during usual activities as a percentage of their preinjury level, they reported an average 93.9% (range, 70%-100%), with 14 of the 19 athletes reporting >95% of preinjury function. When asked to rate their current level of sports activity as a percentage of their preinjury level, participants reported an average of 90.3% (range, 40%-100%), with 11 of the 19 athletes reporting >95% return of athletic function. Table 4 summarizes the results of the patient-reported outcomes.
Patient-Reported Outcomes (n = 19) a
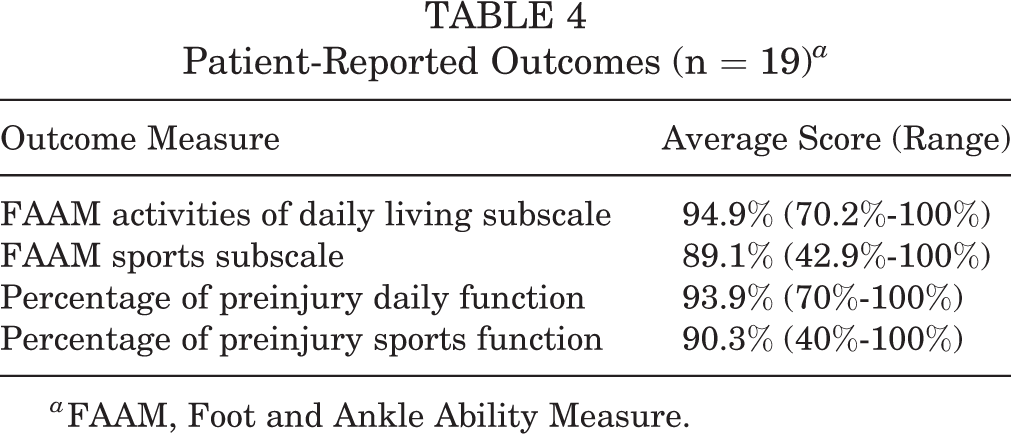
a FAAM, Foot and Ankle Ability Measure.
Long-term follow-up radiographs (>1 year) were obtained on 14 of 26 (54%) fractures at an average of 6.5 years postoperatively (range, 1.2-16.5 years). Of those who participated in the survey or had long-term follow-up radiographs (84%), there were no reported refractures or additional surgery of the included fifth metatarsal.
Discussion
In our cohort, we did not observe any nonunions or fracture-related complications after Jones fracture fixation, with an accelerated average return to play of 3.6 weeks (<6 weeks for all athletes). While an early return to play without radiographic evidence of union remains controversial, we only observed 1 refracture (4%), and this was 1 year from the initial injury and after the screw had been removed for soft tissue irritation 6 months after the primary fixation procedure. Even if this is considered a true refracture, our results did not demonstrate a higher refracture rate than previous studies in high-level athletes returning to play. 7,9,12,18,23 These studies described a much longer recovery before return to sport than we describe in our current protocol, but failed to demonstrate superior outcomes.
Debate continues among team physicians about when athletes should be allowed to return to play and what criteria must be met. Our protocol for 22 years has been to use clinical progression of symptoms as the guide for return to play, and this study demonstrates excellent clinical results with this. We believe that our results are related to early stable surgical fixation combined with routine bone stimulator use as well as a defined protocol of progression based on symptoms that allows the athlete to return to play quickly and safely. While most authors advocate for radiographic evidence of healing before return to play, the results still vary. Glasgow et al 8 reported on a series of fractures in athletes treated with 4.5-mm malleolar screws, and early return to play was associated with delayed union and refracture, suggesting the screw diameter did not provide sufficient support to allow healing. Wright et al 28 reported 6 refractures upon return to play despite all athletes showing radiographic healing before return to play. Lareau et al 12 hypothesized that this high rate may have been related to the use of 4.0- and 5.0-mm cannulated intramedullary screws that were undersized. However, in our series, similar cannulated 4.0- or 4.5-mm implants were used in 38% of our cases, and we did not observe the same complications.
A variety of implants were utilized over the long study period reported in this series. Based on biomechanical studies demonstrating the superior strength of solid, indication-specific screws, previous authors have advocated for their use. 20,21,25 While we currently prefer indication-specific screws, we observed excellent early return to play and long-term results with a low complication rate in our series, despite 38% of implants being cannulated screws and 50% being variable-pitch screws. This again points to accelerated rehabilitation and progression based on symptoms as the key factors for successful return to play in our study, as opposed to implant selection alone. Nagao et al 19 reported findings similar to ours in a series of Jones fractures in athletes treated with headless compression screws and an early return to running at an average of 6 weeks.
Our study is not the first to describe return to play based on clinical symptoms. A study by de Oliveira Massada et al 6 reported good results with 100% union rate in a series of 15 high-level athletes. The authors used the absence of pain on clinical examination and during physical activities to indicate that an athlete was ready to return to sport, even in the absence of radiographic union. This series of athletes, a large majority of whom were soccer players, had an average return to play of 7.5 weeks (range, 2-12 weeks). Lareau et al 12 also concluded that “physical examination and ability to return to play are as important as degree of radiographic healing” when determining the timing of return to play and reported an average return to play of in-season National Football League athletes of 8.7 weeks (range, 5.9-13.6 weeks).
Several authors have attempted to identify factors that contribute to poor outcomes in Jones fractures in athletes. Lee et al 15 found, in a large series of 163 elite athletes, that high BMI and radiographic protrusion of the fifth metatarsal head have a significant association with refracture after surgery and recommended that these athletes return to sport more slowly. The average BMI of athletes in our study was 28.4, with excellent results.
This study has several strengths. First, the study period over 22 years is the longest published series we are aware of, with an average follow-up greater than 8 years and 26 fractures included. Our patient population consisted of high-level collegiate athletes across a variety of sports and included both male and female patients; return-to-play data were accurately recorded prospectively into a database by athletic trainers. Also, 2 experienced surgeons who work closely together, with the same surgical indications, performed the same surgical technique for all procedures.
We acknowledge the limitations of our study, most obviously the limitation of retrospective review of our clinical experience. Also, there was a lack of routine and long-term radiographic follow-up on 46% of patients, although 76% completed patient-reported outcomes. Altogether, 21 of 25 (84%) patients were reached for the study follow-up, and based on the excellent outcome scores reported, we feel it is safe to assume there were no hardware complications or nonunions that radiographs would have elicited. In addition, most complications should have been evident in this patient population at short-term follow-up during their collegiate athletic career, while they were being treated exclusively by our practice. Additional limitations include the use of variable implants and the absence of a control group.
Conclusion
Our study demonstrates that operative treatment of athletes with acute Jones fractures and a symptom-guided rehabilitation program allows athletes to return to play quickly without significant risk. In our experience, and based on the results presented in this study, most (81%) returned to play in less than 5 weeks. Not only does this protocol result in early return to play, but it has demonstrated successful long-term outcomes as well.
Footnotes
Final revision submitted November 29, 2019; accepted December 17, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.W. has received educational support from Arthrex and Peerless Surgical and hospitality payments from DePuy, Smith & Nephew, and Stryker. S.M. has received speaking fees, consulting fees, and royalties from Arthrex; educational support from Arthrex and Peerless Surgical; and hospitality payments from Smith & Nephew. L.B. has received educational support from Arthrex and Peerless Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Greenville Health System (file No. Pro00053666).
Appendix
Jones Fracture Questionnaire