
Abstract
Background:
Knot tying is a crucial component of successful arthroscopic shoulder surgery. It is currently unknown whether sliding or nonsliding techniques result in superior clinical outcomes.
Purpose:
To assess the clinical outcomes of arthroscopic sliding knot (SK)– versus nonsliding knot (NSK)–tying techniques during arthroscopic shoulder surgery, including rotator cuff repair, Bankart repair, and superior labral anterior-posterior (SLAP) repair.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic search of the PubMed, Embase, and Cochrane Library databases was performed using PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines. All English-language literature published between 2000 and 2018 reporting clinical outcomes utilizing SK- or NSK-tying techniques during rotator cuff repair, Bankart repair, and SLAP repair with a minimum 24-month follow-up was reviewed by 2 independent reviewers. Information on type of surgery, knot used, failure rate, patient satisfaction, and patient-reported outcomes was collected. Patient-reported outcome measures included the Constant-Murley score, Rowe score, and visual analog scale for pain. Study quality was evaluated using the modified Coleman Methodology Score.
Results:
Overall, 9 studies (6 level 3 and 3 level 4) with a total of 671 patients (mean age, 52.8 years [range, 16-86 years]; 65.7% male; 206 SK and 465 NSK) were included. There were 4 studies that reported on Bankart repair in 148 patients (63 SK and 85 NSK), 3 on SLAP repair in 59 patients (59 SK), and 2 on rotator cuff repair in 464 patients (84 SK and 380 NSK). Also, 6 studies compared knot-tying with knotless techniques (3 Bankart repair studies and 3 SLAP repair studies), while the studies reporting the outcomes of SLAP repair evaluated SK-tying techniques only. The failure rate for Bankart repair was 3.2% (2/63) for SKs and 4.7% (4/85) for NSKs. The failure rate for rotator cuff repair was 2.4% (2/84) for SKs and 6.3% (24/380) for NSKs. The failure rate for SLAP repair was 11.9% (7/59). Because of inconsistencies in outcomes and procedures, no quantitative analysis was possible. The mean modified Coleman Methodology Score for all studies was 65.1 ± 8.77, indicating adequate methodology.
Conclusion:
The literature on clinical outcomes using SKs or NSKs for shoulder procedures is limited to level 4 evidence. Future studies should be prospective and focus on comparing the use of SKs and NSKs for shoulder procedures to elucidate which arthroscopic knot results in superior clinical outcomes.
As indications for arthroscopic shoulder surgery have expanded, arthroscopic knot tying has become an essential surgical skill for practicing orthopaedic surgeons. 9 Success in knot tying is pivotal for achieving results comparable with open surgery and is dependent on numerous factors. 50 An ideal arthroscopic knot must be able to withstand the greatest amount of stress during cyclic loading encountered during the early postoperative period 35 while maintaining a low profile, optimal tissue apposition for healing, 38 and ease of knot tying. 3 Surgeon experience, patient-specific factors, 15 type of surgical intervention, wet surgical conditions, 9,37 and different surgical techniques and materials used 10 can all influence the performance of the knots. With numerous confounding factors, knot configuration crucially contributes to knot security, with different techniques resulting in differing amounts of tension and performance under biomechanical strain. 50
A nonsliding knot (NSK) is generally utilized in situations when the suture material does not slide easily through soft tissue or the anchor 3 or when there is concern about damage to the tissue. 3,48 Nonsliding configurations do not require the surgeon to pull the suture through the anchor and tissue to tighten the knot and approximate tissue tension. 33,42 However, maintaining tension on the initial knot loop of an NSK is difficult and can make preserving tension more difficult than when tying a sliding knot (SK). 26,36 Although several studies 16,32,34,49 have compared the biomechanical features of SKs and NSKs, the results are controversial and do not definitively demonstrate the superiority of one knot-tying technique over the other. Biomechanical analyses have used differing suture materials and in vitro procedures, which have produced varied results. For example, some studies 32,49 have suggested that the sliding French knot exhibits the best tissue tension and knot security compared with other sliding and nonsliding techniques, while other studies 7,16 have demonstrated that the nonsliding square knot and surgeon’s knot had superior performance. While biomechanical studies make important contributions to understanding the role of suture configurations in stability and strength, in vivo analysis provides insight into the performance of techniques in the environment where they will ultimately be used.
In light of this, understanding the performance of SK- compared with NSK-tying techniques on surgical success could allow orthopaedic surgeons to make informed decisions regarding which techniques to use in vivo. To our knowledge, no previous study has reviewed the clinical outcomes of SK- versus NSK-tying techniques in arthroscopic shoulder surgical procedures, including arthroscopic rotator cuff repair, arthroscopic Bankart repair, and arthroscopic superior labral anterior-posterior (SLAP) repair. The purpose of this systematic review was to assess the clinical outcomes of arthroscopic SK- or NSK-tying techniques for arthroscopic rotator cuff repair, arthroscopic Bankart repair, and arthroscopic SLAP repair.
Methods
Using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, 40 2 independent reviewers (C.D.M. and E.J.) conducted a search of English-language literature using the PubMed, Cochrane Library, and Embase databases up to September 6, 2018, using the following search terms: “arthroscopic” OR “arthroscope” OR “arthroscopy,” “knot,” “shoulder.” An initial search of the 3 databases resulted in 291 results, with 1 additional article that was identified by title through a search of the references. 5 After the removal of 98 duplicates, 194 titles were screened for eligibility. Included studies assessed the clinical outcomes of arthroscopic rotator cuff repair or arthroscopic shoulder instability surgery (posterior or anterior) using arthroscopic knot tying (levels of evidence 1-4). Studies reporting on knotless anchors only or in which the knot type was unclear were excluded. Disparities among eligible studies were resolved by a discussion between the 2 reviewers. This resulted in 9 remaining studies, which were included in this review. The literature search is summarized in the PRISMA flowchart (Figure 1).
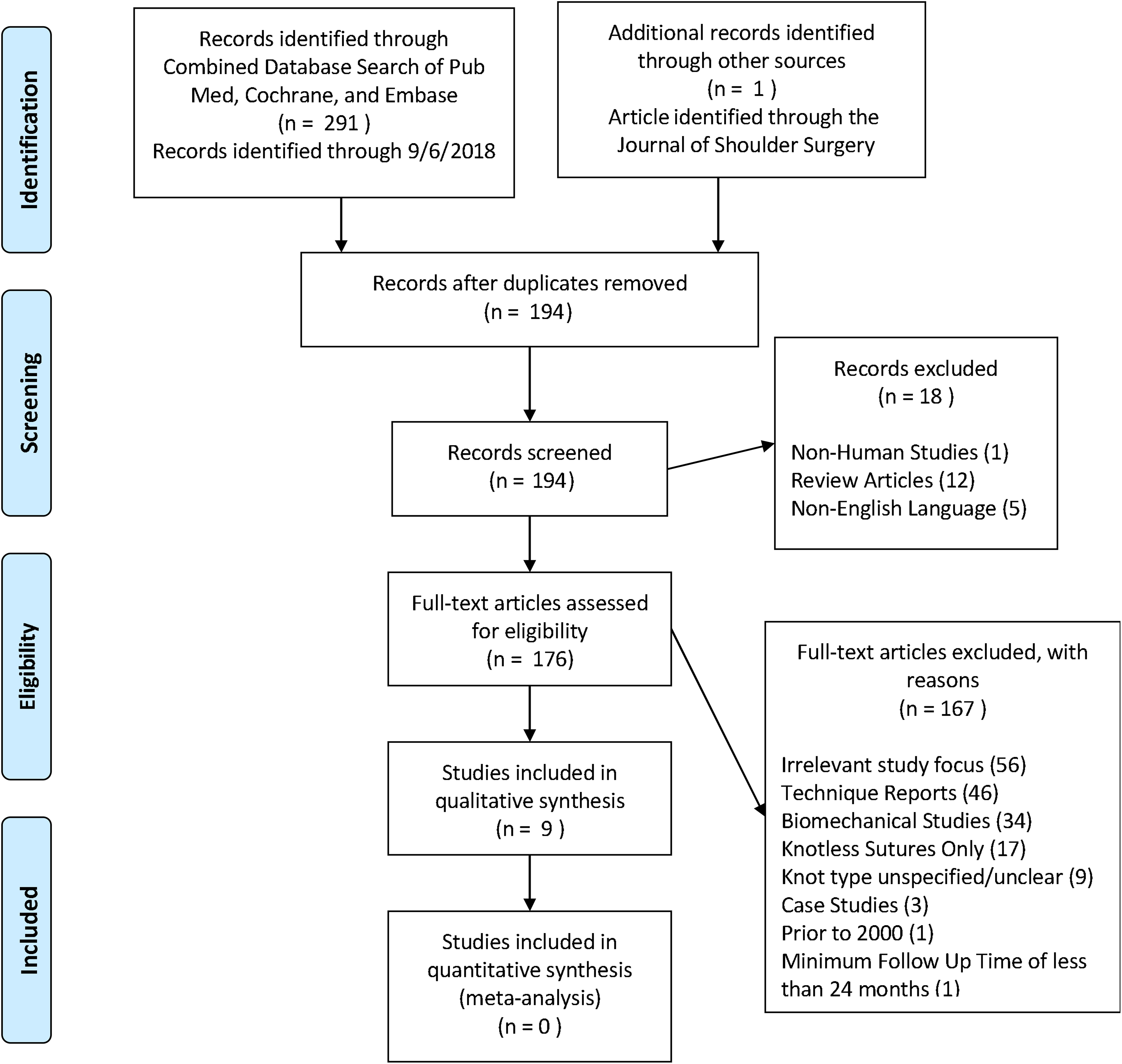
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
SKs were defined as knot-tying techniques that involve a variation of the slip knot, which can be “slid” up the post strand and into the joint to provide a good approximation of tissue tension. 36 NSKs were defined as knot-tying techniques that do not involve the sliding of suture through the eyelet or tissue to achieve knot security.
Reporting Outcomes
Outcomes reported included treatment failure rates, range of motion, and patient-reported outcome scores.
Assessment of Study Quality
There were 2 authors (C.D.M. and E.J.) who independently used the modified Coleman Methodology Score (MCMS) 12 to assess the methodological quality of included studies. The MCMS is based on a scale ranging from 0 to 100; scores of 85-100 are considered excellent, 70-84 are considered good, 55-69 are considered fair, and <55 are considered poor.
Statistical Analysis
Because of the heterogeneity and quality of the included studies, pooling of study results and reporting weighted mean calculations were avoided. 19 Rather, descriptive statistics are presented.
Results
Included Studies
A total of 9 studies (6 level 3 and 3 level 4), 5,6,8,28,29,31,41,45,52 published between 2004 and 2018, met inclusion and exclusion criteria (Figure 1). Of these, 2 studies 6,31 included patients who underwent arthroscopic rotator cuff repair (1 SK 6 and 1 NSK 31 ), 4 studies 8,28,29,41 included patients who underwent arthroscopic Bankart repair (2 SK 28,41 and 2 NSK 8,29 ), and 3 studies 5,45,52 included patients who underwent arthroscopic SLAP repair with the use of SKs exclusively. Because all 3 studies 5,45,52 reporting the outcomes of arthroscopic SLAP repair compared SK-tying and knotless techniques only, no descriptive comparisons between NSKs and SKs were possible.
Assessment of Study Quality
Table 1 shows the MCMS scores from the 9 included studies (mean MCMS score, 65.1), 2 of which (1 NSK 31 and 1 SK 41 ) achieved good scores and 6 of which (5 SK 5,6,28,45,52 and 1 NSK 8 ) achieved fair scores. The remaining study (1 NSK 29 ) was of poor quality. This indicated that the overall quality of the study was fair.
Modified Coleman Methodology Score

Country of Origin
Essentially, 3 of the included studies originated in Germany (1 NSK study of Bankart repair, 29 1 SK study of SLAP repair, 45 and 1 SK study of rotator cuff repair 6 ). Further, 2 studies were authored in the Republic of Korea (1 NSK study of Bankart repair 8 and 1 SK study of SLAP repair 52 ). Moreover, 2 other SK studies of Bankart repair were from Turkey 28 and Singapore. 41 The final SK study of SLAP repair was conducted in France, 5 and the only NSK study of rotator cuff repair was conducted in the United States. 31
Conflict of Interest
Of the 9 included studies, 2 studies 6,28 did not clearly report whether there was a conflict of interest, while 7 of the studies 5,8,29,31,41,45,52 did not report a conflict of interest.
Patient Demographics
A total of 671 patients were included in this systematic review (65.7% male; 206 SK and 465 NSK), including 148 patients who underwent arthroscopic Bankart repair (63 SK and 85 NSK) between August 2001 8 and December 2014, 29 464 patients who underwent arthroscopic rotator cuff repair (84 SK and 380 NSK) between January 1997 6 and September 2007, 31 and 59 patients who underwent arthroscopic SLAP repair (59 SK) between January 2000 5 and 2014 45 (Table 2). The mean follow-up time ranged from 29 8 to 40.5 45 months (range, 24 5,8,31,41,52 to 84 31 months). The mean age of the patients ranged from 21.1 41 to 67 31 years (mean age, 52.8 years [range, 16 8 to 86 31 years]). The mean time to surgery varied among the studies. Only 4 studies 6,28,41,45 stated the time between onset and surgery; 2 of these studies 28,41 reported on Bankart repair, with 1 study 41 reporting surgery 6 weeks after the second dislocation and the other study 28 reporting an intervention after the first dislocation. The study 45 reporting time to surgery before SLAP repair had a mean of 13.6 months before surgery. In the SK study 6 reporting on rotator cuff repair, surgery was performed a range of 3 to 14 months after the onset of pain. Further details on patient demographics and study design are presented in Tables 2 and 3, respectively.
Descriptive Data a
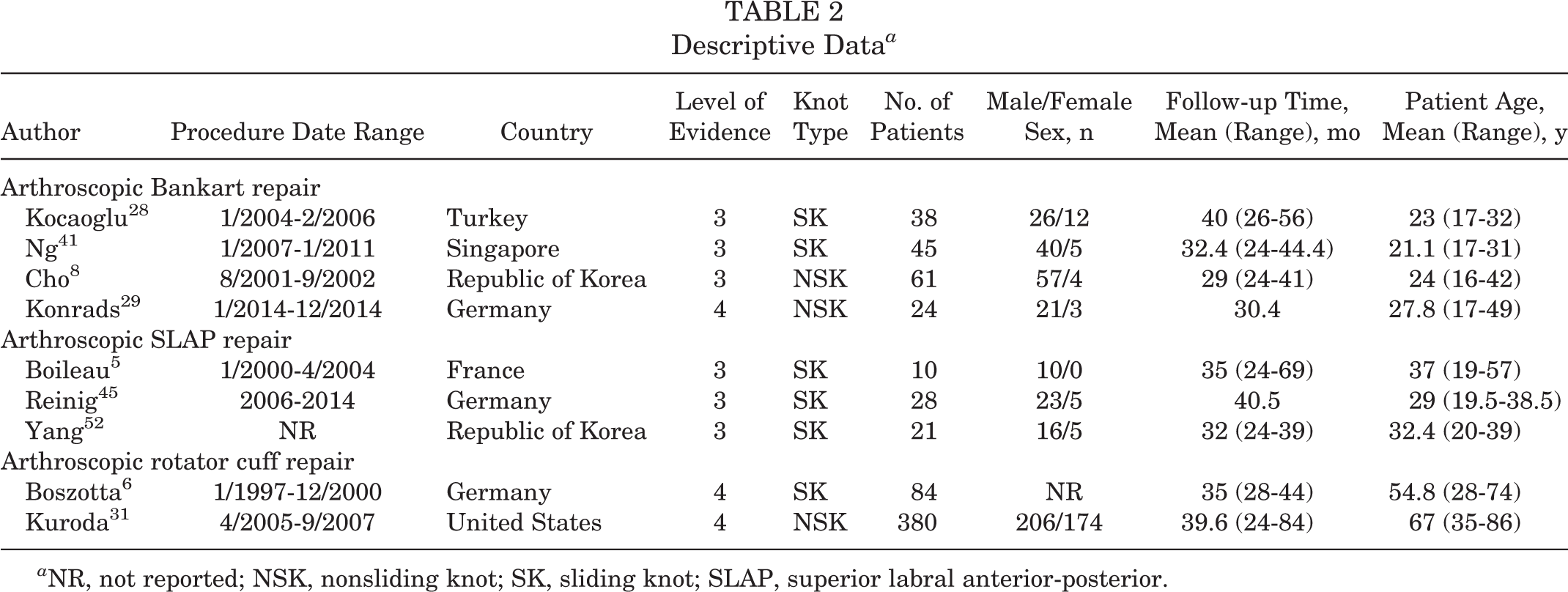
a NR, not reported; NSK, nonsliding knot; SK, sliding knot; SLAP, superior labral anterior-posterior.
Summary of Included Studies a
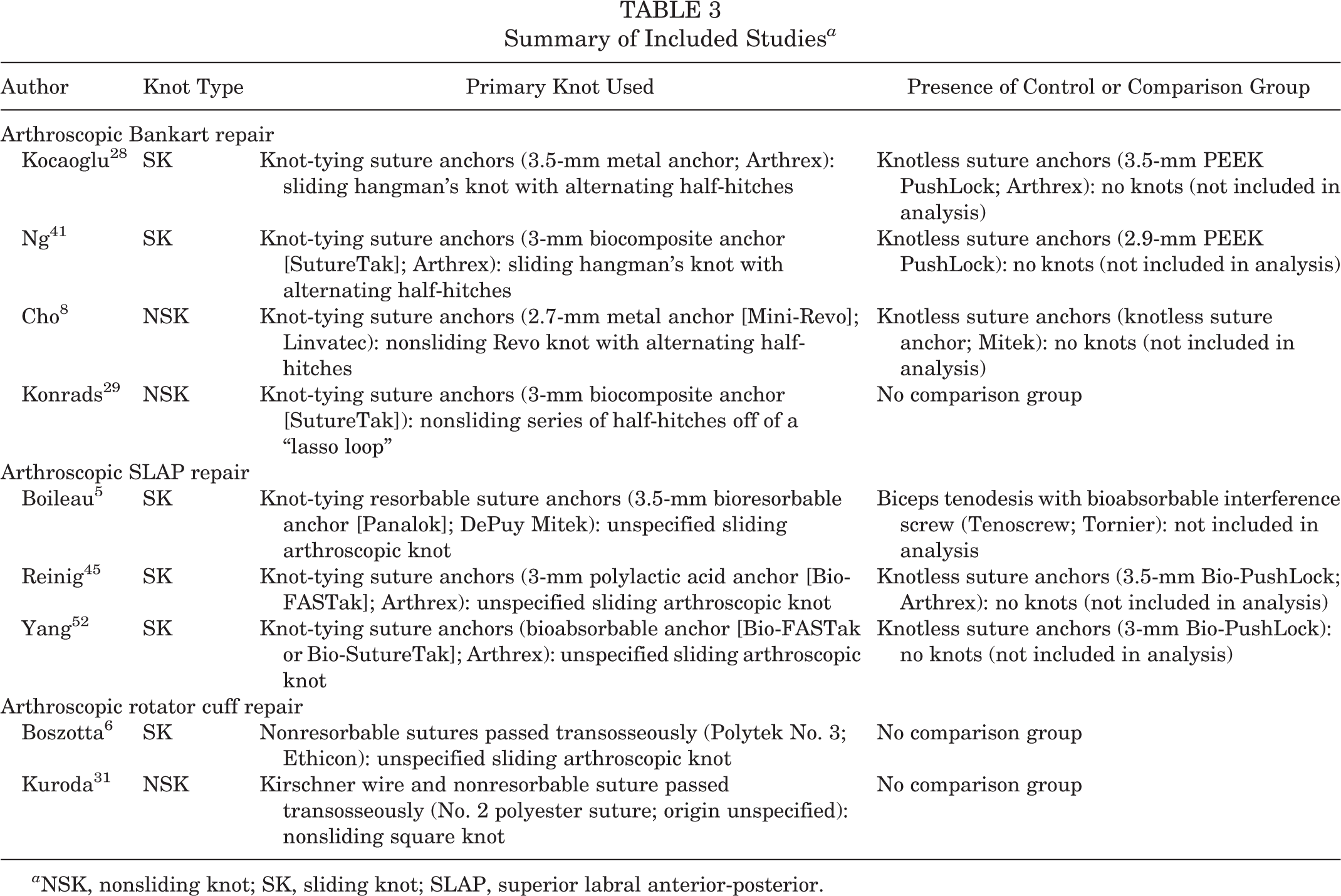
a NSK, nonsliding knot; SK, sliding knot; SLAP, superior labral anterior-posterior.
Surgical Techniques
This systematic review of 9 studies 5,6,8,28,29,31,41,45,52 evaluated knot-tying techniques used during 3 different arthroscopic surgical procedures, including arthroscopic SLAP repair, arthroscopic Bankart repair, and arthroscopic rotator cuff repair (Table 3). The procedures included the use of a wide variety of indications, suture materials, and knot types. To simplify comparisons, knot-tying techniques were separated into 2 broader categories: SK and NSK.
Failure Rate
All 9 studies 5,6,8,28,29,31,41,45,52 reported failure rates.
Arthroscopic Bankart Repair
Failure after arthroscopic Bankart repair using SKs was defined as a redislocation, recurrent anterior subluxation, 41 or a positive apprehension test finding. 28 For the 2 studies 8,29 using NSKs for arthroscopic Bankart repair, a redislocation or complication related to surgery was also reported as failure.
Of the 2 studies assessing patients treated with arthroscopic Bankart repair using SKs, 1 study 28 reported a failure rate of 5.6% (1/18), while the other study 41 reported a slightly lower rate of failure (2.2%; 1/45). The 2 studies assessing patients undergoing arthroscopic Bankart repair using NSKs had failure rates of 4.9% (3/61) 8 and 4.2% (1/24). 29
Arthroscopic SLAP Repair
Failure after arthroscopic SLAP repair using SKs 5,45,52 was defined as residual pain with overhead activities precluding participation in sports, revision surgery, or reported surgery-related complications.
One study 5 reported a failure rate of 40.0% (4/10), resulting in a subsequent reoperation (biceps tenodesis) at a mean of 15 months after SLAP repair. Other studies showed lower rates of failure of 0.0% (0/21) 52 and 10.7% (3/28), 45 resulting in subsequent reoperations (2 biceps tenodesis procedures and 1 tenotomy procedure).
Arthroscopic Rotator Cuff Repair
For the 2 studies 6,31 reporting on arthroscopic rotator cuff repair, failure was defined as a complication related to surgery for the SK group and a retear after repair in the NSK group. Retears in the NSK study 31 were identified using magnetic resonance imaging (MRI) according to the Sugaya grading system. 20 All retears identified on MRI scans were reported as failures. 31
The SK study reported a failure rate of 2.4% (2/84), 6 while the NSK study resulted in a failure rate of 6.3% (24/380). 31 Complications arose for 2 patients (2.4%; 2/84) in the SK study, 6 with 1 patient developing a seroma (1.2%; 1/84) and the other patient developing frozen shoulder symptoms, requiring manipulation under general anesthesia (1.2%; 1/84). No retears were reported in the SK study. All failures reported in the NSK study (24/380) 31 were caused by either small or large tears identified on MRI scans.
Clinical Outcomes
The most commonly reported outcome measures from included studies were the Constant-Murley score, 13 the University of California, Los Angeles (UCLA) score, visual analog scale (VAS) for pain, 21 range of motion, and patient satisfaction (Table 4).
Outcomes Reported a
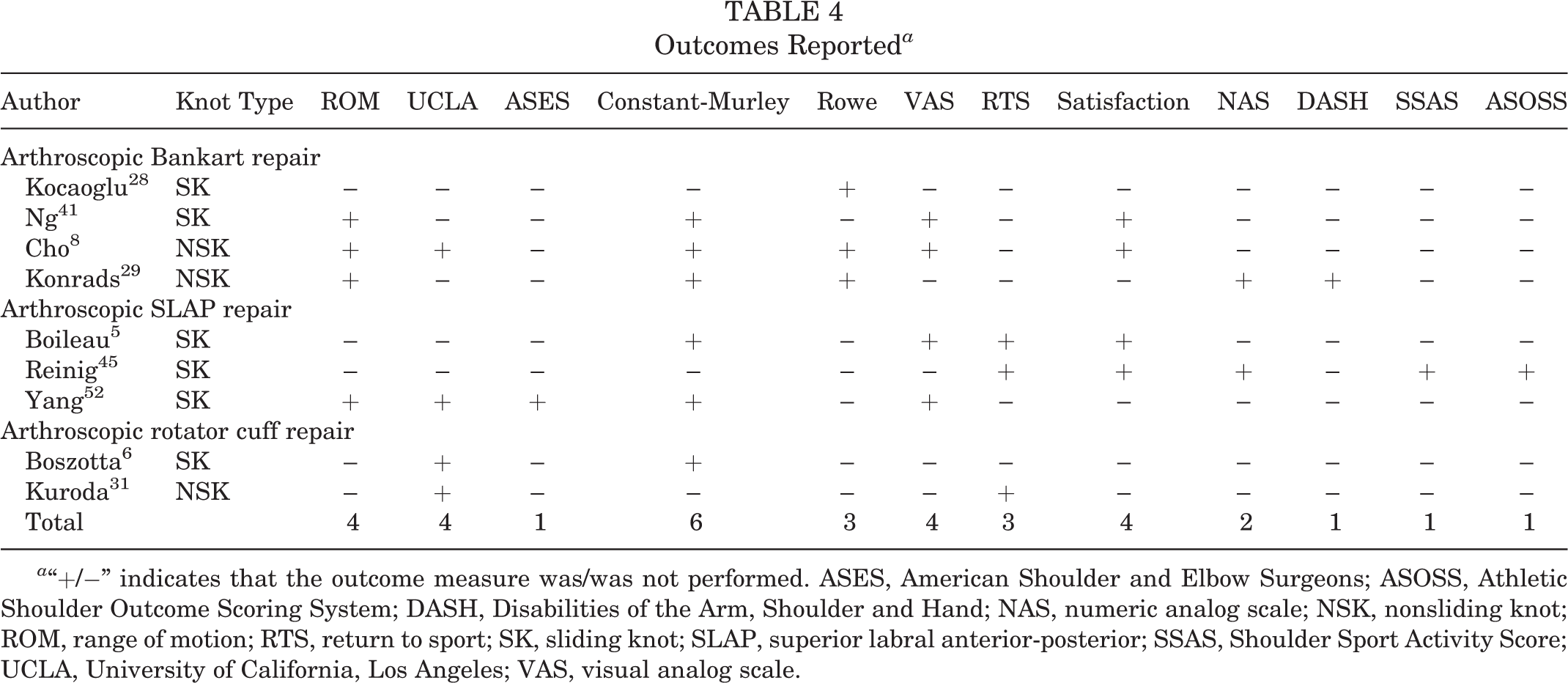
a “+/−” indicates that the outcome measure was/was not performed. ASES, American Shoulder and Elbow Surgeons; ASOSS, Athletic Shoulder Outcome Scoring System; DASH, Disabilities of the Arm, Shoulder and Hand; NAS, numeric analog scale; NSK, nonsliding knot; ROM, range of motion; RTS, return to sport; SK, sliding knot; SLAP, superior labral anterior-posterior; SSAS, Shoulder Sport Activity Score; UCLA, University of California, Los Angeles; VAS, visual analog scale.
Patient-Reported Outcomes
Preoperative and postoperative Constant-Murley scores were reported for patients in 4 of the studies 5,8,41,52 involving shoulder instability procedures (2 arthroscopic Bankart repair 8,41 and 2 arthroscopic SLAP repair 5,52 ). An additional study reported on preoperative scores only. 29 For the 2 studies 5,52 reporting the Constant-Murley score after arthroscopic SLAP repair using SKs, mean improvements between preoperative and postoperative scores were demonstrated (18 ± 5.2 5 and 20.8 ± 7 52 ; P value not reported). The Constant-Murley score after arthroscopic Bankart repair showed similar mean improvements after the use of both SKs (28 ± 10; P < .05) 41 and NSKs (29; P < .001). 8
There were 2 studies 8,28 that reported on the improvement of Rowe 46 scores in patients after arthroscopic Bankart repair, with 1 SK study reporting a mean improvement of 51 points 28 and 1 NSK study reporting a mean improvement of 48 points. 8
Also, 2 studies reported on the improvement of VAS scores in patients after arthroscopic Bankart repair, with 1 SK study reporting a mean improvement of –1.8 (P < .05) 41 and 1 NSK study reporting a mean improvement of –1.9 (P < .001). 8
VAS scores after arthroscopic SLAP repair were not comparable; only 1 SK study 52 reported on both preoperative and postoperative VAS scores, with an improvement of –3.8 (preoperative: 4.8; postoperative: 1.0; P value not reported).
The UCLA score improved after arthroscopic rotator cuff repair for both the SK 6 and the NSK 31 studies, with SK procedures showing a slightly higher improvement in scores (SK, 19.8; NSK, 13.6). The reported preoperative UCLA score was lower for the patients who underwent rotator cuff repair with the use of SKs (11.3) 6 compared with patients who underwent repair with the use of NSKs (19.1). 31 Both the SK 6 and the NSK 31 studies showed comparable postoperative UCLA scores, with the SK study 6 reporting a mean postoperative score of 31.1 (P < .001) and the NSK study 31 reporting a mean postoperative score of 32.7 (P value not reported). Tear size, Constant-Murley scores, and patient satisfaction were not reported by both studies and could not be compared.
Patient satisfaction was reported in 2 5,45 of the 3 arthroscopic SLAP repair studies and 2 arthroscopic Bankart repair studies. 8,41 After arthroscopic Bankart repair, 1 SK study 41 reported a mean patient satisfaction of 6.9 on a scale from 1 to 10, whereas 1 NSK study 8 reported a satisfaction rating of 4.53 ± 0.01 on a scale from 1 to 5 using the modified UCLA score. Both of these results indicated moderate to high patient satisfaction after arthroscopic Bankart repair with the use of both SK- and NSK-tying techniques. In contrast, an SK study 5 on patient satisfaction after arthroscopic SLAP repair reported that only 4 of 10 (40.0%) patients were “satisfied or very satisfied.” Another SK study 45 on patient satisfaction after arthroscopic SLAP repair reported a mean score of 2.0 ± 0.8 on a scale from 1 to 15.
Range of Motion
The differences in range of motion after arthroscopic Bankart repair were described in 1 SK study 41 and 1 NSK study. 8 The SK study 41 reported a 2° difference in forward flexion and a –3° difference in external rotation with the arm at the side. Neither of these findings was significantly different from preoperative values (P > .05). 41 The NSK study 8 reported a –1° difference in forward flexion and a –4° difference in external rotation at the side. These findings were also not significantly different from the preoperative values (P > .05). 8 An NSK study 29 reported on postoperative range of motion after arthroscopic Bankart repair (extension/flexion: 30°/0°/170°; abduction/adduction: 70°/0°/20°; external rotation/internal rotation 60°/0°/95°) but did not report preoperative range of motion data. Range of motion differences after arthroscopic SLAP repair were noted in 1 SK study, 52 which indicated no significant difference between operated and contralateral shoulders (P > .05). No other studies on arthroscopic SLAP repair reported on range of motion.
Discussion
The results of this systematic review suggest that during arthroscopic shoulder surgery (arthroscopic Bankart repair, arthroscopic SLAP repair, and arthroscopic rotator cuff repair), there may be a mild qualitative superiority of SK- compared with NSK-tying techniques in Constant-Murley and Rowe scores at a minimum follow-up of 24 months (range, 24-84 months). Failure rates did not clearly suggest the superiority of one technique over the other. For example, failure rates after arthroscopic Bankart repair using SKs showed a range of 2.2% to 5.6%, 28,41 and NSK studies reported failure rates with a range of 4.2% to 4.9%. 8,29 While the 3 studies 5,45,52 reporting on failure rates after arthroscopic SLAP repair demonstrated a larger range of failure (0.0%-40.0%), 5,52 all arthroscopic SLAP repair studies were performed using SKs and may simply be demonstrating this variation based on the SK type and numerous other factors (suture type, surgeon experience, patient demographics, etc). The reported failure rates for arthroscopic rotator cuff repair were somewhat comparable for the SK study 6 (failure rate: 2.4%; mean age, 54.8 years) and NSK study 31 (failure rate: 6.3%; mean age, 67 years). However, failure definitions differed between studies, with the NSK study 31 using postoperative MRI to determine the presence of retears and the SK study 6 describing only complications without reporting on the incidence of retears as evidenced on MRI scans. Additionally, in the older patient population in the NSK study, 31 failure rates may have been higher because of more fragile tissue and a higher risk of retears rather than a difference in knot types.
The surgical techniques, indications, and knot types varied widely among the 9 included studies, making it impossible to definitively state that 1 type of knot resulted in superior clinical outcomes. Unfortunately, no previous comparative studies were identified in the currently available literature that specifically examined SKs in comparison with NSKs exclusively. Moreover, knot types differed even within the sliding and nonsliding categories (see Table 3). With SKs, the slip knots tend to loosen easily, and thus, techniques have been modified to ensure that they remain seated in place within the shoulder. This class of knot can be further separated into locking (or self-locking) and nonlocking knots. Nonlocking knots are most reliably secured by a series of half-hitches on alternating posts, while locking knots can generally be flipped or otherwise modified within the joint to prevent the knot from backing off. This study included both kinds of locking knots. The key drawback to SKs is the possibility of injuries or cutting of the tissue on the suture-tendon interface while the knot is being secured. 48 With NSKs, tissue must be held in place while the knot is tied to ensure correct placement and additional compression. This added complication makes these knots more challenging to master but critical for situations when the suture cannot slide freely. 47 Biomechanical studies 1 –3,20,22,23,44 have demonstrated that different types of SKs and NSKs have different ultimate loads to failure, 1,2 resistance to sliding, 20,23 ease of knot tying, 3 elongation and knot migration, 24,25,44 and distance to failure. 22 Therefore, even if 2 studies use SKs, they may produce inconsistent results because of differences between the knot types. In a study by Hanypsiak et al, 18 it was shown that knot strength varies even among expert orthopaedic surgeons, both among arthroscopic surgeons and among knots tied by the same surgeon. Even in studies in which 1 surgeon tied all knots, there may have been variation in knot strength from patient to patient.
Other technical factors may include patient positioning, 39 arthroscope orientation, 51 bone-tendon contact pressure, 17 anchor type, 43 or suture type and strength, 22 all of which have been studied as independent factors with the potential to affect the outcome of a procedure. Additionally, wet conditions within the joint can lead to increased friction of the suture material, 9 and knot security may ultimately be reduced compared with hand-tied knots by the requisite use of instrumentation. 37 Patient-specific factors, such as intrinsic tendon degradation and osteoporosis in older patients, may compromise repair fixation, requiring advanced reinforcement techniques. 15
Different surgical interventions involve using knots under differing amounts of tension depending on placement and, therefore, different modes of failure. This study included surgical interventions for the treatment of shoulder instability and rotator cuff tears, but techniques and indications for these surgical procedures also vary and are not directly comparable across studies. It should be noted, however, that there are studies 27,30 that suggest that as long as 3 reversing half-hitch knots are tied, the strength of the SK is dependent on the half-hitch throws and independent of SK configuration. Additionally, the suture material and number of reversing half-hitches on alternating posts locking the knot in position affect the amount of friction holding the knot in position and, therefore, the integrity of the knot itself. 10
These confounding factors make arthroscopic knots challenging and may contribute to the inconsistency in knot performance even among trained arthroscopic surgeons performing hundreds of procedures annually. 18 However, in practice, the arthroscopic knot utilized is often determined by surgeon preference, training, and experience. 7,11,14 In a study by Baumgarten and Wright, 4 an internet-based survey was used to determine arthroscopic knot preferences of American Orthopaedic Society for Sports Medicine members. Interestingly, the survey 4 demonstrated that most surgeons rely on experience and preference of a knot type over biomechanical evidence, with only 17.4% of respondents basing their knot tying on a literature review and the majority using the same knot configuration for all arthroscopic procedures.
Limitations
The strengths of this study include a comprehensive systematic review of available (level 3-4 evidence) studies by 2 independent reviewers. In addition, this is the first systematic review to specifically compare the clinical outcomes of SK- and NSK-tying techniques for shoulder instability repair. The limitations of this study should also be noted. The knot type differed greatly among studies (see Table 3), with all studies using a slightly different variation, as well as additional differences in suture types, indications, and procedures, further complicating comparisons. Treatment failure was not defined equally in all studies, and a variety of patient-reported outcome measures were used without much consistency among studies. A study 29 did not report on improvement of various patient-reported outcomes, and others 5,29,31,52 did not include P values for a comparison. Additionally, of the 3 studies 5,45,52 reporting on SLAP repair, none included the use of NSK-tying techniques, and thus, knot types could not be compared. Performance and time period bias may have been present. Finally, some studies did not provide precise means for various patient-reported outcomes, thereby prohibiting the authors from performing a meta-analysis or calculating weighted means for these scores.
Conclusion
The literature on clinical outcomes using SKs or NSKs for shoulder procedures is limited to level 3 and 4 evidence. The quality of the literature precludes any definitive conclusions regarding the performance of arthroscopic knot-tying techniques in a clinical setting. The data analyzed in this systematic review involved a wide variety of knot-tying techniques and surgical procedures in addition to varied measures for patient-reported outcomes. The lack of consistency made quantitative analysis impossible. However, described evidence suggests little discernable qualitative difference in clinical performance between SK- and NSK-tying techniques.
It is unclear from the data whether variability is caused by the quality of a surgeon’s knot or if surgical success is operator-dependent. Inconsistency in knot strength and tension, even when tied by the same surgeon, has been demonstrated in other studies and may prove to have a large effect on clinical outcomes. To conduct a more thorough and conclusive review, more consistent data on knot types are needed to determine the most effective arthroscopic knot for the procedures studied. Future studies should be prospective and focus more heavily on study design. Studies should utilize explicit eligibility criteria regarding knot-tying procedures in addition to comparing the most commonly employed techniques.
Footnotes
Final revision submitted December 16, 2019; accepted December 23, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.C.M. has received research support from Arthrex, Biomet, Breg, Mitek, Ossur, Smith & Nephew, and Stryker; consulting fees from DePuy and Zimmer Biomet; speaking fees from Arthrex; and royalties from Elsevier and Zimmer Biomet. A.J.S. has received educational support from Gemini Mountain Medical and Arthrex, honoraria from Encore Medical, and consulting fees from Medacta. M.L.W. has received educational support from Gemini Mountain Medical. A.F.V. has received educational support from Arthrex, consulting fees from Stryker and Smith & Nephew, and speaking fees from Arthrex and Smith & Nephew. R.M.F. has received grant support from Arthrex; educational support from Arthrex, Medwest, and Smith & Nephew; speaking fees from Arthrex; and royalties from Elsevier. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.