
Abstract
Background:
Superior labral anterior to posterior (SLAP) tears are one of the most common injuries to the shoulder, with the type II variant representing the most frequently encountered subtype.
Purpose:
To systematically review the literature to better understand outcomes after arthroscopic repair of isolated type II SLAP lesions using knotted versus knotless anchors based on implant number, implant location, patient position, and portal position.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review investigating all studies in the literature between January 2000 and June 2019 reporting on patients undergoing arthroscopic repair for isolated type II SLAP lesions using knotted versus knotless suture anchors was performed following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines using the PubMed, BIOSIS Previews, SPORTDiscus, PEDro, and Embase databases.
Results:
A total of 234 patients undergoing isolated arthroscopic repair of type II SLAP lesions using suture anchors were identified, with 76% (179/234) treated using knotted anchors versus 24% (55/234) treated using knotless anchors. Complications were reported in 12% of patients treated using knotted anchors versus no patients treated using knotless anchors (P = .008). The incidence of complications for knotted anchor repair was not significantly affected by patient position (P = .22) or portal position (P = .19). Using multiple regression analysis, we found no significant association with the incidence of complications when analyzing for anchor design (R 2 = 0.02; P = .06) or anchor position (R 2 = 0.02; P = .92). No significant difference in return-to-activity timing was appreciated based on anchor type (P = .28), patient position (P = .98), or portal position (P = .97) in patients treated using knotted anchors.
Conclusion:
Patients treated using knotted anchors were significantly more likely to experience a postoperative complication compared with patients treated using knotless anchors after arthroscopic repair of isolated type II SLAP lesions. Despite the increased incidence of a postoperative complication after knotted anchor fixation compared with knotless anchor fixation, multiple regression analysis showed that anchor design and anchor position were not significantly predictive of the incidence of complications. Given the increasing popularity of knotless anchor fixation, further study on the long-term outcomes after knotless repair for isolated type II SLAP lesions is warranted.
Superior labral anterior to posterior (SLAP) lesions are among the most commonly reported injuries of the shoulder, identified in up to 26% of patients undergoing shoulder arthroscopic surgery. 21,38 SLAP lesions are classified into 4 subtypes, with type II SLAP tears characterized by labral fraying with detachment of the long head of the biceps tendon (LHBT) anchor representing the most commonly reported variant, present in 21% to 75% of patients with SLAP lesions. 1,12,15,17,37,38 Type II lesions generally occur from a combination of tensile, shear, and compressive forces acting across the biceps-labral complex, primarily during overhead activity and throwing. 1,6 Patients generally report pain with overhead activity and mechanical symptoms, such as clicking or catching. 9 While SLAP lesions are typically associated with concomitant abnormalities within the shoulder, such as rotator cuff injuries, isolated SLAP lesions are commonly encountered. 4,21
Because of the limited intrinsic healing capacity of the labrum, nonsurgical management of patients with symptomatic type II SLAP lesions is often unsuccessful. 10 Currently, arthroscopic repair represents the standard of care for young, active patients with type II injuries in whom nonoperative management has failed. 33 Multiple fixation methods have been described, including biointerference screw fixation, transosseous sutures, and bioabsorbable tacks. 5,35 The current standard of care is repair with suture anchors. 24 Previous studies reporting outcomes in patients undergoing repair for type II SLAP lesions have demonstrated inconsistent return to activity and functional scores, especially in overhead athletes. 5,7,19,24,27,37 While knotted anchors have traditionally been utilized during arthroscopic repair, 18,30 concerns over knot migration and knot abrasion within the shoulder have led to an increased interest in the use of knotless anchors over the past decade. 2,3,13,31,32,40 However, no investigation has examined postoperative outcomes based on differences in implant type in patients undergoing arthroscopic management of isolated type II SLAP lesions using suture anchors. 15,18,34
This systematic review of the literature sought to determine differences in postoperative complications and return to activity between knotted and knotless anchors after arthroscopic repair of isolated type II SLAP lesions based on (1) the number of anchors utilized, (2) anchor location (relative to the LHBT), (3) patient position (lateral decubitus vs beach-chair), and (4) portal position (rotator interval vs trans–rotator cuff). Based on previous investigations, we hypothesized there would be fewer complications in patients treated using knotless anchors, 2,11 with no significant differences in return to activity between patients treated using knotted versus knotless anchors.
Methods
A systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines using a PRISMA checklist. 23 All literature pertaining to patients undergoing arthroscopic repair of isolated type II SLAP lesions using suture anchors published between January 2000 and June 2019 was identified. There were 2 authors (D.M.K. and J.G.K.) who independently conducted a literature search in April 2019 using the following databases: PubMed, BIOSIS Previews, SPORTDiscus, PEDro, and Embase. Each search included the following terms: type II AND superior labral anterior to posterior AND tear AND arthroscopy AND surgery AND complications AND failure AND reoperation AND activity.
The inclusion criteria consisted of English-language articles or articles with English translations on human participants with isolated type II SLAP tears undergoing primary arthroscopic repair with details regarding the surgical technique and implant utilized. Studies with levels of evidence of 1 to 4 were included. Exclusion criteria included studies consisting of patients with concomitant shoulder injuries including rotator cuff tears, Bankart lesions, and shoulder instability; patients with a history of shoulder surgery; and patients with isolated lesions treated nonsurgically or without suture anchors, as well as case reports and studies with a level of evidence of 5. Studies including patients who underwent concomitant arthroscopic rotator cuff repair, distal clavicle resection, or subacromial decompression were excluded, along with any studies including patients treated using biceps tenodesis.
After the 2 independent authors’ search of the literature, a total of 525 articles were identified. The search process is shown in the flow diagram in Figure 1. After an assessment of titles and abstracts, 38 articles were selected for further evaluation. Of these studies, 28 were excluded because of a lack of details regarding the surgical technique (n = 2); being case reports (n = 6); the presence of additional procedures or concomitant abnormalities (n = 14); the inclusion of patients with type I, III, or IV SLAP lesions (n = 4); the exclusion of patients with complications (n = 1); and having a level of evidence of 5 (n = 1). After the application of the inclusion and exclusion criteria, 10 studies were identified for analysis. To ensure that all available studies were identified, references cited in the included articles were cross-referenced for inclusion if they were overlooked during the initial search, during which no further studies were identified.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of studies.
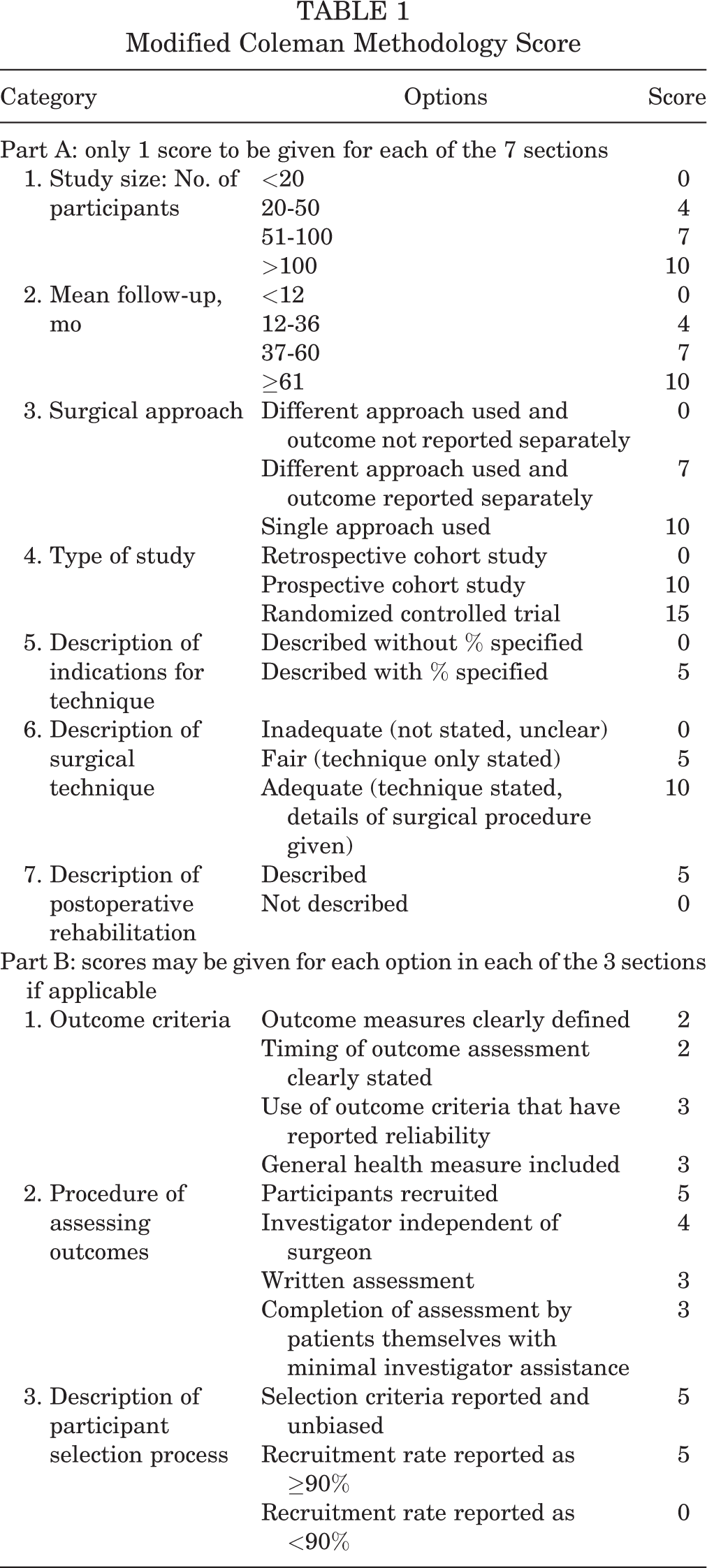
To assess the quality of the studies, the modified Coleman Methodology Score (MCMS) was used, which allows for the evaluation of study methodology based on 10 criteria, for a total score between 0 and 100. The subsections that compose the Coleman Methodology Score are based on the subsections of the CONSORT (Consolidated Standards of Reporting Trials) statement (for randomized controlled trials), which are modified to allow for other trial designs. The Coleman Methodology Score was modified to make it reproducible and relevant for the systematic review examining outcomes following arthroscopic repair of isolated Type II SLAP lesions using suture anchors. Each study was independently scored in duplicate by 2 authors (D.M.K. and J.G.K.) for each of the criteria adopted (Table 1). Any disagreements were resolved by a discussion with the senior author (J.E.V.). Scores of 85-100 were considered excellent, 70-84 good, 55-69 fair, and <55 poor.
Modified Coleman Methodology Score
The chi-square test was used to evaluate for differences between knotted versus knotless anchors based on the number of anchors utilized and the incidence of complications after fixation. Differences in return-to-activity timing were evaluated using the Shapiro-Wilk test to determine the normality of data, followed by analysis using the Mann-Whitney U test. The incidence of complications after knotted anchor fixation based on anchor position, patient position, and portal position was analyzed using the chi-square test. Multiple regression analysis was performed to investigate the association with the incidence of complications after fixation using anchor design and anchor position as independent variables. Return-to-activity timing for patients treated using knotted anchors based on patient position and portal position was analyzed using the Mann-Whitney U test. A P value <.05 was considered to be statistically significant. All analyses were performed using SPSS statistical software (version 25.0; IBM). The normal distribution of data was determined using the Shapiro-Wilk test.
Results
Of the 10 articles meeting inclusion criteria, a total of 234 patients undergoing arthroscopic repair for isolated type II SLAP lesions using suture anchors were identified (Table 2). The mean patient age at the time of surgery was 33.5 ± 6.5 years. Furthermore, 74% (165/222) of patients were male, while sex was not reported in 1 study consisting of 12 patients. 24 The mean final follow-up after surgery was 35.0 ± 7.8 months (range, 24-48 months) (Table 3). The dominant arm underwent repair in 80% (107/133) of patients, while arm dominance was not reported in 5 studies. 16,24,27,28,29
Overview of Included Studies a
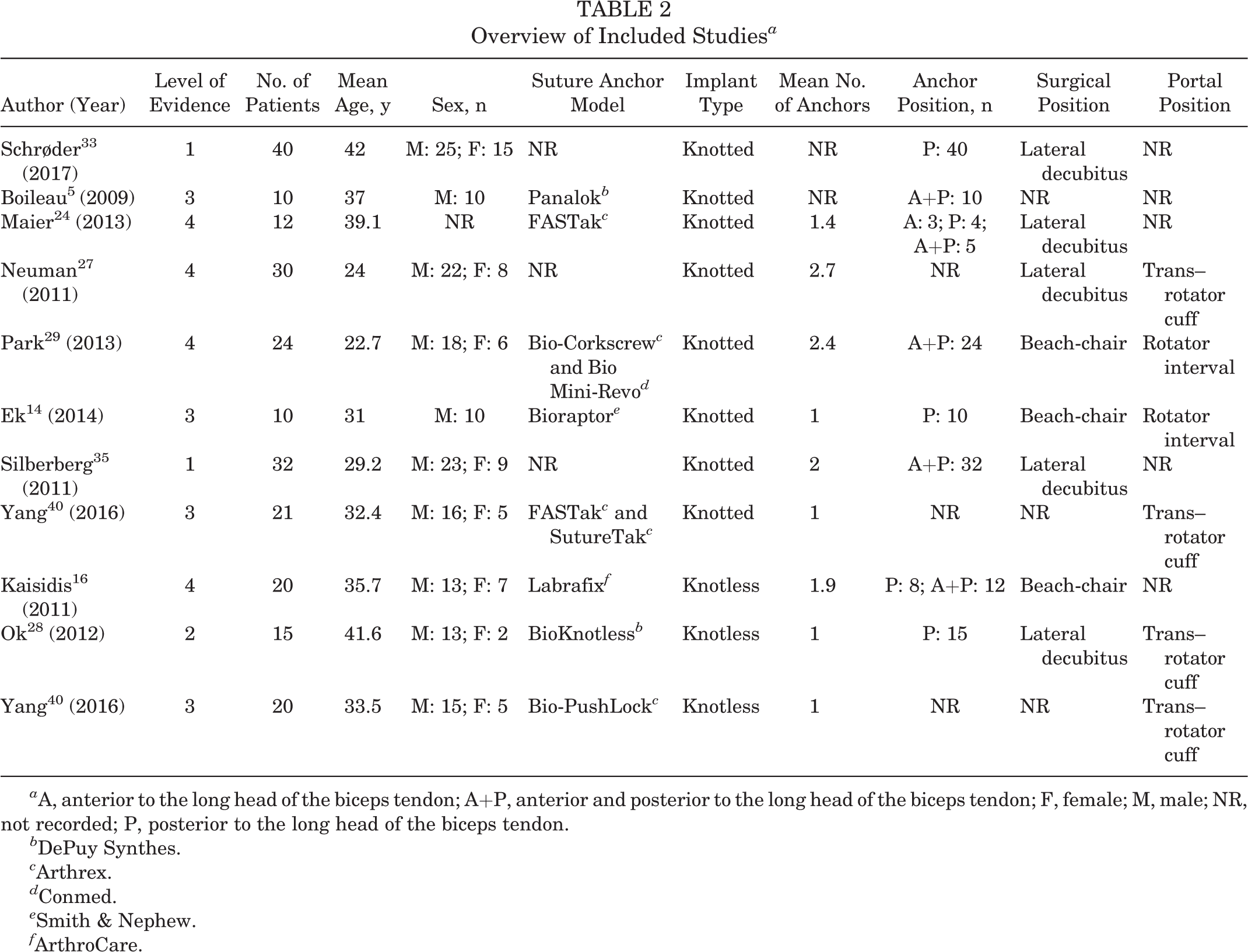
a A, anterior to the long head of the biceps tendon; A+P, anterior and posterior to the long head of the biceps tendon; F, female; M, male; NR, not recorded; P, posterior to the long head of the biceps tendon.
b DePuy Synthes.
c Arthrex.
d Conmed.
e Smith & Nephew.
f ArthroCare.
Overview of Study Results a

a MCMS, modified Coleman Methodology Score; NR, not recorded.
Additionally, 76% (179/234) of patients were treated using a knotted suture anchor, 5,14,24,27,29,33,35,40 while 24% (55/234) of patients were treated using a knotless suture anchor 16,28,40 (Table 2). The median number of anchors used per patient was 1.4 (range, 1.0-2.7). No significant difference in the anchor number was appreciated when comparing knotted (median, 1.7 [range, 1.0-2.7]) with knotless (median, 1.0 [range, 1.0-1.9]) anchors (P = .22). For knotted anchors, implants were primarily placed anterior and posterior to the LHBT (55%; 71/128), followed by placement that was posterior (42%; 54/128) and anterior (2%; 3/128) to the LHBT. For knotless anchors, 34% (12/35) of implants were placed anterior and posterior to the LHBT, 66% (23/35) of implants were placed posterior to the LHBT, while no implants were placed anterior to the LHBT. Data on the patient position were provided for 183 patients, with the lateral decubitus position most commonly used in knotted anchor placement (77%; 114/148), while the beach-chair position was more commonly utilized during knotless anchor placement (57%; 20/35). The portal position was reported in 120 patients, with the trans–rotator cuff portal being utilized in 60% (51/85) of knotted anchors and 100% (35/35) of knotless anchors.
The presence or absence of postoperative complications was reported in 214 patients (Table 3). No complications were reported in patients treated using knotless anchors (0%; 0/55), 28,40 while a complication was recorded in 12% (21/179) of patients treated using knotted anchors (P = .008). 5,14,24,27,29,33 Complications in patients treated using knotted anchors included postoperative stiffness (n = 7), 14,33 suture anchor failure requiring revision surgery (n = 7), 24,27,29 persistent pain with overhead activity (n = 4), 5 osteolysis (n = 2), 29 and revision requiring rotator interval closure (n = 1). 27 Using multiple regression analysis, we found no significant association between anchor design (R 2 = 0.02; P = .06) or anchor position (R 2 = 0.02; P = .92) and the incidence of complications after fixation. The incidence of complications was not significantly different when comparing patients treated using knotted anchors in the lateral decubitus position (10%; 11/114) 24,27,33 versus the beach-chair position (18%; 6/34) (P = .22). 14,29 No significant difference in complications was appreciated based on the utilization of a trans–rotator cuff portal (8%; 4/51) 27,40 versus a rotator interval portal (18%; 6/34) (P = .19). 14,29
Return to full activity after surgery was reported in 53% (57/107) of patients treated using knotted anchors, 5,14,24,27,29,40 while the number of athletes returning to full activity following knotless repair was only explicitly reported in a single study, occurring in 45% (9/20) of patients 16,28,40 (Table 3). The mean time to return to full activity was 7.7 ± 3.2 months (range, 3.0-11.7 months). No significant difference in return-to-activity timing was reported when comparing patients treated using knotted (mean, 6.8 ± 3.1 months) versus knotless (mean, 6.3 ± 1.4 months) anchors (P = .28). Moreover, return-to-activity timing was not significantly different when comparing patients treated using knotted anchors in the lateral decubitus (mean, 7.4 ± 6.2 months) versus the beach-chair position (mean, 7.9 ± 1.6 months) (P = .98). 14,16,24,27,29 In the 2 studies examining return-to-activity timing based on positioning in patients treated using knotless anchors, those undergoing repair in the lateral decubitus position returned to activity sooner (mean, 5.5 months) versus patients treated in the beach-chair position (mean, 8 months). 16,28 Based on portal position, return-to-activity timing in patients treated using knotted anchors was not significantly different when comparing those with a trans–rotator cuff portal (mean, 8.6 ± 4.4 months) versus a rotator interval portal (mean, 7.9 ± 1.6 months) (P = .97).
The mean MCMS score was 60.3 (range, 51-73), demonstrating that the quality of the studies was fair. No significant difference was appreciated between the mean MCMS scores calculated by the 2 examiners (Table 3).
Discussion
The principal findings from this investigation were that in patients undergoing arthroscopic repair for isolated type II SLAP lesions, no significant differences in the number of knotted versus knotless anchors were appreciated; the majority of knotted anchors were placed anterior and posterior to the LHBT, while knotless anchors were most commonly placed posterior to the LHBT. The lateral decubitus position was primarily utilized for knotted anchor repair, while the majority of patients undergoing knotless anchor repair were treated in the beach-chair position, with the trans–rotator cuff portal utilized most commonly in both groups. Complications were reported in 12% of patients treated using knotted anchors, while no complications were reported in patients treated using knotless anchors. No significant difference in the incidence of complications was appreciated based on patient position or portal position for patients treated using knotted anchors, and using multiple regression analysis, we found no significant correlation with the incidence of complications when analyzing anchor design and anchor position as independent risk factors. Moreover, no significant difference in return-to-activity timing was appreciated based on the use of knotted versus knotless anchors or based on patient position or portal position in patients treated using knotted anchors.
Currently, the optimal number and position of different anchor implants used during arthroscopic repair of isolated type II SLAP lesions remain controversial. The use of multiple anchors has been shown to improve labral stability and enlarge the footprint of the attachment. 18,20 However, few studies have documented the reasoning behind the number of anchors utilized, with most authors reporting the use of the fewest possible number of anchors to minimize hardware failure and potential irritation for isolated type II SLAP lesions. 14,24,29,30 Meanwhile, anchor placement has not been shown to possess any biomechanical advantage when comparing the placement of knotted anchors anterior versus posterior to the LHBT. 26 Functionally, the cadaveric investigation performed by McCulloch et al 25 demonstrated that knotted anterior anchor placement relative to the biceps anchor had a small but statistically significant effect on limiting external rotation potentially because of tensioning of the anterior tissues, which may be detrimental to overhead athletes in whom external rotation is necessary for optimal performance. Although we found that anchor position was not predictive of a complication occurring after fixation, further investigations are warranted to better understand the role of anchor position in predicting the postoperative complication risk. As such, the interplay of stability and performance must be taken into account when planning surgical fixation for athletes and physically active patients with isolated type II SLAP lesions.
A trans–rotator cuff portal was more commonly utilized for both knotted and knotless anchors, with no significant difference in the incidence of complications or return-to-activity timing appreciated based on portal position in patients treated using knotted anchors. Few previous studies have compared the use of a trans–rotator cuff portal versus rotator interval portal for arthroscopic treatment of isolated type II SLAP lesions. The investigation by Cohen et al 8 demonstrated that patients with a trans–rotator cuff portal reported significantly lower American Shoulder and Elbow Surgeons scores and satisfaction when compared with patients treated using a rotator interval portal for isolated SLAP lesions. The authors also reported that 81% of patients had postoperative night pain after treatment using a trans–rotator cuff portal. In addition, Stephenson et al 39 found a positive correlation for the potential development of full-thickness rotator cuff tears in patients who underwent previous SLAP repair with an incorrectly placed trans–rotator cuff portal. As such, while portal position remains dependent on the surgeon’s preference and comfort, further studies examining long-term outcomes related to subjective scores, complication rates, and return-to-activity timing are necessary to determine the optimal portal position for both knotted and knotless anchors.
No difference in return-to-activity timing was appreciated when comparing knotted versus knotless anchors. Moreover, no complications were reported in patients treated using knotless anchors, while the most commonly reported complications using knotted anchors included anchor failure and postoperative stiffness. While not specifically reported, potential causes responsible for these complications occurring in patients with knotted anchors include knot migration, leading to anchor failure, and knot irritation of the rotator cuff, leading to decreased motion and subsequent stiffness. 32 The theoretical advantage of knotless anchors when compared with traditional knotted anchors is less risk of irritation because of the absence of bulky knots in the small paralabral space, particularly in overhead athletes in whom contact of the posterior rotator cuff frequently occurs. Rhee and Ha 32 noted a case of knot-induced glenoid erosion after arthroscopic repair of a type II SLAP lesion using a knotted suture anchor, resulting in pain and bony damage postoperatively. Moreover, knotless anchors are low profile and capable of restoring the anatomic footprint of the labrum. 12 However, biomechanical studies have demonstrated mixed benefits of knotless anchors when compared with knotted anchors. The cadaveric study by Leedle and Miller 22 reported that knotless anchors (Knotless Suture Anchor; Mitek) had statistically higher loads to complete failure when compared with 2 commercially available knotted suture anchors (Panalok 3.5-mm Anchor and GII QuickAnchor; Mitek). Moreover, the study by Reinig et al 31 found that knotless suture anchors allowed greater shoulder range of motion when compared with knotted anchors, while a recent study by de Groot et al 11 reported that knotless anchors were less likely to require revision surgery when compared with knotted anchors after SLAP repair. In contrast, the cadaveric study by Sileo et al 36 reported that knotted suture anchors possessed higher loads to failure and more cycles until failure compared with knotless anchors. Meanwhile, retrospective reviews and cohort studies have reported equivalent clinical outcomes based on visual analog scale scores, range of motion, operative time, and return-to-activity timing when comparing knotted versus knotless suture anchor fixation. 2,3,40 As such, causes behind anchor failure and postoperative stiffness in knotted anchors, as well as studies examining long-term outcomes and return-to-activity timing after knotless anchor fixation, are needed to better understand the risks and benefits of knotted versus knotless anchor repair for the treatment of isolated type II SLAP lesions.
Limitations
This study was not without limitations. Because of the heterogeneity of reported subjective outcomes, we were unable to directly evaluate patient satisfaction or outcome scores, as well as narcotic utilization after surgery, based on anchor type. Moreover, only 3 studies reported postoperative range of motion, preventing any meaningful statistical analysis from being performed. 28,35,40 The small sample size and fair MCMS scores were related to the strict inclusion/exclusion criteria utilized. The manufacturer and type of suture anchors utilized were infrequently reported, preventing any reliable reporting of the most commonly utilized implants and whether implants were single- or double-loaded. The identification of additional patient- and surgeon-specific factors is necessary to determine potential differences in postoperative outcomes, complications, and return-to-activity rates and timing based on implant type. Not all patients included in this review were competitive athletes; as such, the generalizability of these results to investigations examining return to play and functional outcomes exclusive to nonathlete or athlete-specific cohorts is unknown. Moreover, because of the heterogeneity of the reported data, studies reporting differences in type II subtypes were combined to allow for improved homogeneous statistical analysis. 24,35
Conclusion
Patients treated using knotted anchors were significantly more likely to experience a postoperative complication compared with patients treated using knotless anchors after arthroscopic repair of isolated type II SLAP tears, while no significant difference in return-to-play timing was appreciated based on anchor type. As the popularity and use of knotless anchors increase, future studies examining outcomes after knotless anchor repair are warranted.
Footnotes
Final revision submitted September 20, 2019; accepted October 4, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.J.G. has received consulting fees from Tornier, Encore Medical, Aevumed, DJO, and Wright Medical; speaking fees from Arthrex; and hospitality payments from Shoulder Innovations and Stryker. M.J.S. has received consulting fees from Smith & Nephew and Stryker, speaking fees from Smith & Nephew, educational support from Elite Orthopaedics, and honoraria from Fidia Pharma. J.E.V. has received consulting fees from Stryker and Linvatec, speaking fees from Arthrex, and educational support from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.