
Abstract
The first collegiate rowing race was held in 1829 between the University of Oxford and the University of Cambridge, making rowing the oldest known collegiate sport. In 1896, it was one of the inaugural events of the modern Olympics. The number of female intercollegiate rowing teams has nearly doubled since Title IX was enacted in 1976, 15 and over the past 20 years, the number of injuries reported in high-level rowers has increased. 9
Rowing is a nonimpact sport involving repetitive motions that require both endurance and strength. Low back pain is the most common complaint in rowers. 1,5,10,15,16,18,24 A review of rowing injuries in elite rowers revealed that low back was the second most common location of injury, with the knee being the first. 15 Holden and Jackson 14 showed that 82.2% of elite female rowers experienced low back pain, and the majority of injuries related to rowing are repetitive use injuries. 16,24
Stress fractures in athletes may develop in bones unadapted to excessive repetitive loading, where the repetitive force leads to bone resorption out of proportion to repair. 8 Rib stress fractures are the most widely reported, accounting for 10% of all rowing injuries. 14,15 Here, we report the case of an elite collegiate female rower with a stress fracture of the left transverse process of the third lumbar vertebra. The first reported case of a sports-related transverse process stress fracture was in a young fast bowler in cricket 2 ; to our knowledge, this is the second reported case of a transverse process stress fracture in an athlete and the only published reported case of transverse process stress fracture in a rower.
Case Report
A 21-year-old female National Collegiate Athletic Association (NCAA) Division I collegiate varsity rower with 1 week of acute-onset left-sided lower back pain presented to our sports medicine clinic during in-season training. The patient had been a high-level rower since the age of 15 years. Her current training schedule was 20 hours per week. She had a 3-year precollege history of intermittent, generalized low back pain that resolved after physical therapy. The patient did not have any significant back pain for 2 years before presenting to the clinic. In high school, she had developed a relative energy deficiency, manifesting as overtraining syndrome, restrictive eating habits, weight loss, and secondary amenorrhea, which resolved 6 months before she had low back pain.
Her acute back pain began 4 days before her presentation to the clinic. She had been rowing during practice in a coxless pair to which she had just transitioned during that week. She denied any inciting event or trauma. She was bedridden because of the severity of her pain for 4 days before being seen by her team physician. Her pain was mostly left-sided and nonradiating. She denied any associated numbness, tingling, or weakness of her extremities and was self-treating with anti-inflammatories. She also received treatment by her athletic trainer but could not tolerate any direct pressure, soft tissue massage, or therapeutic ultrasound to the area.
Physical examination of her lumbar spine was carried out for a flexion of 30° and extension of 25°. She reported pain with transitions between body position and tenderness along the left paraspinal muscles with noted paraspinal hypertonicity. Strength in the lower extremity was normal, and a seated slump examination was negative. Her patellar and Achilles reflexes were normal. She denied any spinous process or sacroiliac joint tenderness. She was found to have acute muscle strain at time of her initial visit and was started on anti-inflammatories and muscle relaxants as needed.
During a follow-up examination 1 week later, she reported improvement of her left-sided back pain while doing water therapy and using a recumbent bicycle; however, her pain was still functionally limiting. Her examination demonstrated improved lumbar flexion/extension; however, paraspinal muscle tenderness persisted. Her physician performed manual therapy on her (eg, muscle energy technique), and she was referred to a physical therapist.
Physical therapy was started 3 weeks after injury onset, and the athlete felt she had hit a plateau in improvement. Spinal rotation was still painful, and she was still unable to fully train because of her pain. Her physical examination was similar to her initial follow-up examination, and lumbar radiographs were ordered.
Four-view lumbar radiographs were normal other than loss of lordotic curve (Figure 1), so magnetic resonance imaging (MRI) was obtained. The MRI showed a left, nondisplaced transverse process fracture at L3, which was best visualized on T1- and T2-weighted axial sequences (Figure 2).
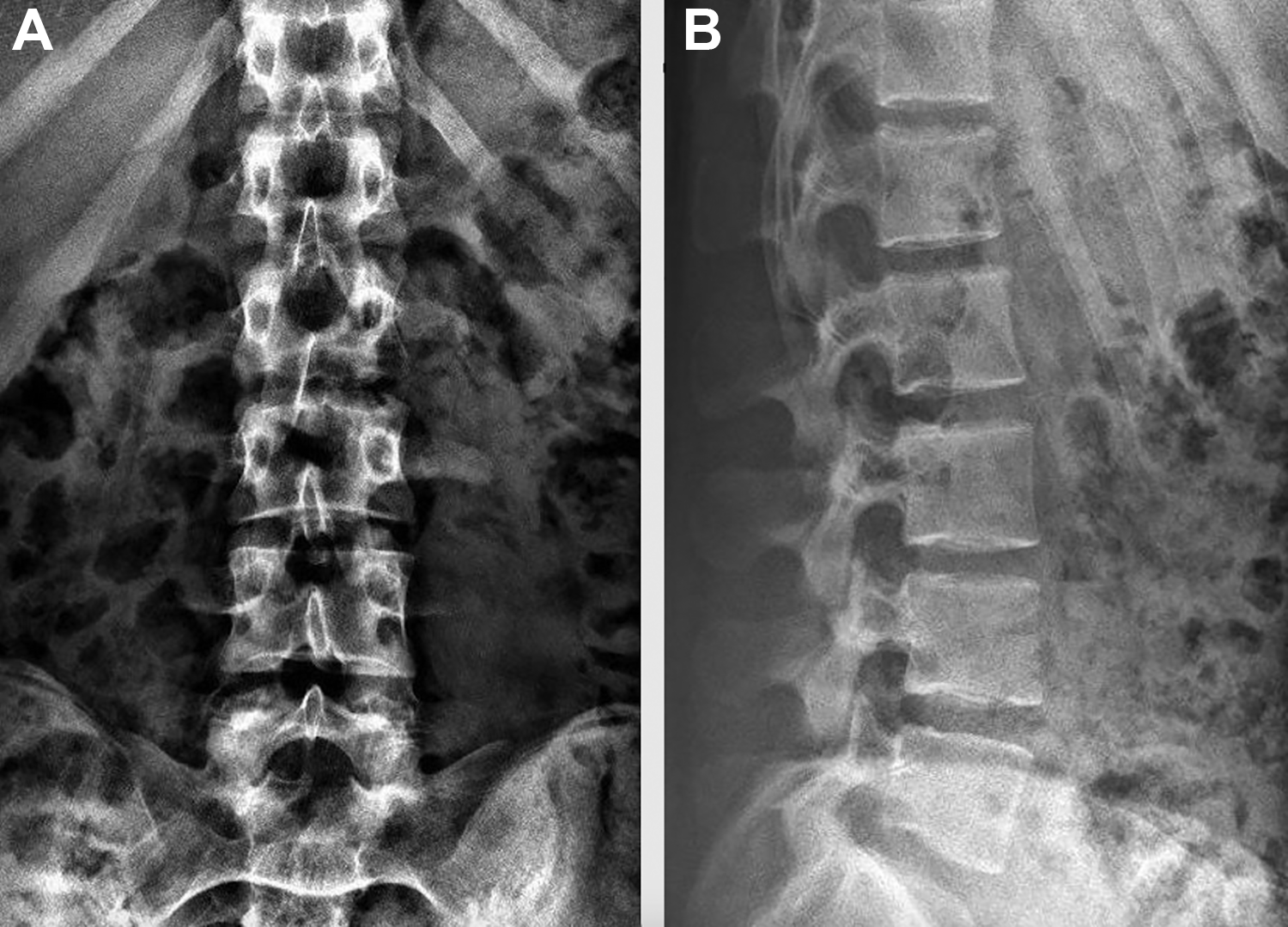
Radiographs of lumbar spine. (A) Anteroposterior projection demonstrating normal appearance of lumbar spine. (B) Lateral projection demonstrating loss of lordotic curve, no fractures identified.

Axial projection of L3 vertebra, fast recovery fast spine-echo T2-weighted magnetic resonance imaging. L3 transverse process nondisplaced fracture is visible (circle).
T2-weighted and short tau inversion recovery sequences demonstrated bone edema, signifying an acute/subacute nature of injury (Figure 3). She was found to have a left L3 nondisplaced stress fracture of the transverse process 1 month after the onset of symptoms.

Sagittal projection of the lumbar spine, short tau inversion recovery magnetic resonance imaging. Arrow indicates bone marrow edema of the transverse process, denoting acute/subacute injury.
Workup for her relative energy deficiency 10 months prior demonstrated normal sex hormone levels as well as vitamin D level. She also had a normal dual-energy x-ray absorptiometry (DEXA) scan with a normal body composition score. No further metabolic workup was done or repeated at the time of the current injury.
The athlete was advised to continue activities as tolerated while avoiding rotational spine exercises. She was given a sacrolumbar support brace with compression straps to be used while doing prolonged activity, as well as to wear during class and times of prolonged sitting. She was withheld from rowing activities and continued supervised rehabilitation under the guidance of her physical therapist and athletic trainer.
Over the next several weeks, the rower was able to increase her activity level and return to light dryland rowing activities 7 weeks after the onset of symptoms. She was able to perform asymptomatic, full, unrestricted activities 13 weeks after initial symptom onset and was subsequently cleared for rowing competition.
Discussion
The vast majority of injuries related to rowing are repetitive use injuries, 16,24 and in elite racers, the ribs, knee, back, and upper extremity are the most common sites of injury, with the low back being the most prevalent. 1,5,10,15,26 Rib stress fractures are the most widely reported stress fractures and have an average incidence of around 10% in rowers. 9,14,15,24,26 Stress fractures occur when bone loses the ability to heal from compounding microdamage during cyclical mechanical loading of bone that is either deficient in mineral/elastic resistance or unaccustomed to muscle stress/torque. 8 The near-maximal isotonic muscle contractions generated in elite rowers may increase the likelihood of stress fractures as muscle fatigue redistributes force to the underlying bone. 20
The mechanism of a transverse process fracture is usually an acute high-energy trauma, violent muscle contraction, or both, such as when a pedestrian is struck by a car. 23,25 In the general public, these fractures are usually associated with complex underlying injuries, 7 but in athletes they tend to be isolated, perhaps because of a lower-energy mechanism of action. 12,25 Acute transverse process fractures are almost exclusively reported in American football, 6,25 but they have also been documented in soccer, 12 skiing, and snowboarding. 11
The rowing stroke is divided into 4 phases—the catch, drive, finish, and recovery—with the drive phase further broken into 3 subphases (legs, body swing, and arm pull through). 19 As the oar enters the water during the catch, the force on the blade of the oar is transmitted through the oar and into the musculoskeletal system. The force rapidly increases during the drive phase. Surface electromyography shows that the rectus femoris provides the power, while thoracic paraspinal muscles stabilize the spine and transfer force to the oar during the drive. As the knees and hips extend during the drive, the lower back works as a braced cantilever for power and stabilization. Lumbar compression and shear loads are stabilized by the lumbar paraspinal muscles during the drive. Toward the end of the drive and during the finish, the abdominal muscles continue to stabilize the spine. During the recovery, the paraspinal muscles relax as the hamstrings and abdominal muscles pull the body forward in preparation for the catch. 15 There are immense forces transmitted to the lower spine during the rowing stroke. In female rowers, the peak shear force in the lumbar spine during a simulated race pace effort was measured to be from 660 ± 117 to 717 ± 69 N. 21
In our athlete, since there was no trauma, we must assume the muscles and their attachments played a major role in development of her stress fracture. There are multiple tissues that act on the lumbar transverse processes. The middle layer of lumbar fascia attaches the transversus abdominis, internal oblique, and external oblique (variable) to the lumbar transverse process. 3,4,27 Cadaveric studies 3,4 have shown that the middle layer of lumbar fascia can transmit forces capable of tearing off lumbar transverse processes and should be considered as contributors to avulsion fractures. Other studies 20,23 have pointed to the attachment of the psoas major and quadratus lumborum on lumbar transverse processes as contributors to fracture. Significant, and of particular relevance, to this case is that the incidence of avulsion fracture clinically is greatest at L3, which coincides with the cumulative attachments of transversus abdominis (via the middle lumbar fascia) and the quadratus lumborum. 4,23 It is important to keep in mind that these studies revolved around acute fracture rather than stress fracture as seen in our case. However, it is impossible to ignore the demonstrated force these muscles may impart to the lumbar transverse processes, particularly L3. A limitation of this case report is that no video analysis of the athlete’s rowing stroke was performed. Video analysis is highly recommended for this type of case in the future. Given that our athlete had just transitioned to rowing in coxless pairs, we believe that the underlying cause of her stress fracture was the recent asymmetric increase in cyclical mechanical load/torque generated by her muscle attachments to her L3 transverse process.
Stress fractures of the lumbar transverse process are likely underreported, as even acute transverse process fractures require high index of suspicion to be correctly identified. 6,17 Computed tomography (CT) is the diagnostic standard for detecting transverse process fractures, as plain radiographs often do not detect them. 17 Plain radiographs did not reveal our athlete’s fracture, and an MRI was done to evaluate both soft tissue and bony pathology. The L3 lumbar transverse stress fracture clearly visible on MRI, thus a CT scan was not performed as it would not have added additional diagnostic value or change in treatment. Typically, however, MRI is unnecessary if the fracture is detected on CT without other spinal injuries. Acute isolated transverse process fractures are typically stable and not associated with neurological deficits. 13 There is increasing evidence that neurosurgical or orthopaedic consultation is not necessary in the management of these injuries. A recent systematic review 22 suggested that transverse process fracture may be nonsurgically managed with pain medication, muscle relaxants, and early mobilization. Healing of transverse process fractures without radiologic signs of instability may be hampered by the use of braces or orthotics; however, the use of such devices may increase patient comfort. 22 Average return-to-play time in sports after transverse process fracture is about 9 weeks. 2,12,25
Our athlete was treated initially with anti-inflammatories and muscle relaxants. She returned to low-level physical activity within 1 week, and when the transverse process stress fracture was diagnosed, she was given a sacrolumbar support brace with compression straps to use during painful, prolonged activity. Her activity level was progressively increased, and she returned to light rowing at 7 weeks after the onset of symptoms. At 13 weeks, she was asymptomatic and cleared to return to full training without restrictions.
This case highlights the unusual presentation of lumbar transverse process stress fracture. Given the high likelihood of underreporting, we recommend that clinicians include transverse process fracture in the differential diagnosis during diagnostic workup for low back pain in female rowers. Furthermore, we suspect that transverse process fracture may be more broadly represented among athletes who were evaluated for low back pain after other athletic endeavors that share a similar biomechanical and metabolic profile with rowing.
Footnotes
Final revision submitted November 13, 2019; accepted December 17, 2019.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.