
Abstract

Keywords
The incidence of injuries to the anterior cruciate ligament (ACL) in skeletally immature patients is increasing. 1,10 The primary goal of managing ACL injury is to restore knee stability to minimize the risk of the secondary damage of menisci and joint cartilage. To avoid the risk of growth disturbance from iatrogenic physeal damage, ACL reconstruction (ACLR) was traditionally delayed until the child was close to the end of the prepubertal growth spurt; however, studies have suggested that the incidences of meniscal damage and cartilage destruction were higher when ACLR was delayed. 8,12 Therefore, surgical intervention has been advocated early to improve functional outcomes even in these skeletally immature patients. 21
Restoring knee stability after ACL injury without growth disturbances is crucial, and various surgical techniques have been described. The 2 main surgical techniques are transphyseal- and physeal-sparing techniques. Physeal-sparing techniques have several variations, depending on the graft passage routes: extra-articular “over-the-top” graft placement, partial physeal-sparing, and complete physeal-sparing (or all-epiphyseal) reconstruction. Each technique has advantages and disadvantages.
According to cadaveric studies, 13,16,25,27 a more anatomic reconstruction might be necessary to improve the knee stability after ACL injury, 26 especially with regard to rotational stability. Although the clinical benefits of double-bundle ACLR are still unclear, the double-bundle technique has gained popularity for adult ACL injury because of an improved ability to replicate the morphology of the intact ACL. Therefore, we have performed all-epiphyseal double-bundle ACLR on patients with wide open physes, in which all bone tunnels were created with the physeal-sparing technique in an attempt to achieve anatomic reconstruction without physeal injury.
According to recent reviews, 6,11 the risk of growth abnormalities is not necessarily eliminated in physeal-sparing procedures. In addition to the surgical technique, bone growth during a growth spurt is expected to have some effects on the ACL graft and, consequently, on knee stability. However, the literature contains few descriptions of these effects. The aim of this study was to evaluate the midterm results of all-epiphyseal double-bundle ACLR on skeletally immature patients and to assess the alignment and morphometric changes in the bone around the knee after the surgery.
Methods
Patients
Since 2012, we have performed all-epiphyseal double-bundle ACLR in 3 children (2 boys and 1 girl). At the time of the operation, 1 boy was 12 years old, the other was 14 years old, and the girl was 13 years old. All patients were evaluated clinically and with magnetic resonance imaging (MRI), and a high-intensity wide band of physes was confirmed on MRI. The mean time from injury to surgery was 3 months (range, 2-5 months). Arthroscopy revealed no concomitant meniscal lesions. The mean length of follow-up was 52.7 months (range, 42-60 months). All methods of data collection received the approval of an institutional review board.
Surgical Technique
Both femoral and tibial bone tunnels were created within the distal femoral and the proximal tibial epiphyses; with fluoroscopic imaging, we ensured that the tunnels did not affect the epiphyseal line (Figure 1). Femoral tunnels for the anteromedial bundle (AMB) and posterolateral bundle (PLB) were created with the outside-in technique, and their positioning on the intercondylar wall of the lateral femoral condyle was determined by reference to the lateral intercondylar ridge. Tibial tunnels were created with remnants of ACL fiber for anatomic placement. A doubled autologous semitendinosus tendon and a gracilis tendon were prepared as the grafts for the AMB and PLB, respectively. The mean diameters of the AMB and PLB grafts were 6 and 5 mm, respectively. Each graft was fixed by an Endobutton CL (Smith & Nephew) on the femoral side and by double-stapling over the surface of the metaphysis away from the proximal physis on the tibial side. The staples were removed 1 year after ACLR.
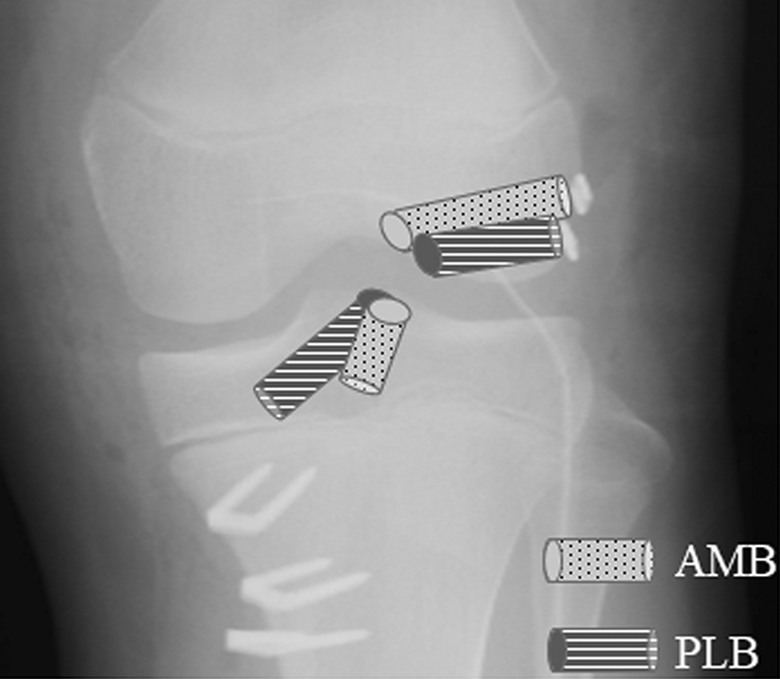
Diagrams of the surgical technique and the 4 drill hole placement. AMB, bone tunnels for anteromedial bundle; PLB, bone tunnels for posterolateral bundle.
Rehabilitation Program
Patients began partial weightbearing with crutches 1 week after surgery, and full weightbearing was allowed at 4 weeks after surgery. The operated limb was initially placed at 30° of flexion in an immobilizing brace, and gentle range of motion exercise was allowed 1 week after surgery. Maximum knee flexion was restricted to 120° until the third week postoperatively. When proper muscle conditioning was achieved, running was permitted at 3 months after surgery.
Clinical Evaluation
Clinical examination comprised the assessment of knee stability and range of motion. Postoperative knee stability was evaluated with the Lachman test, with the pivot-shift test, and by arthrometric measurement with a KT-1000 arthrometer (MEDmetric) 1 year after surgery and at the last follow-up. Patients completed the Lysholm knee rating scale and the Knee injury and Osteoarthritis Outcome Score (KOOS) at the last follow-up. We also evaluated their self-assessment of the function of the operated knee in the Activities of Daily Living and Sports/Recreation activities using a 100-mm visual analog scale.
Radiological Assessment
The presence of leg-length discrepancies and angular deformities was assessed with full-length standing digital radiographs. To evaluate leg-length discrepancies, the distance between the lateral margin of the acetabulum and the medial malleolus was measured in each leg. To evaluate axial malalignment, the hip-knee-ankle angles in both legs were compared (Figure 2A). To assess morphometric changes, anteroposterior knee radiographs before surgery and at the last follow-up were used to compare the tibial plateau widths. The distance between the anterior border of the tibial joint surface and the most posterior point of the Blumensaat line represented the approximate length of the AMB of the ACL; the measurements of both legs were compared on lateral radiographs (Figure 2B). Measurements were performed 3 times, and the average was taken within 0.1° and 0.1 mm with a PACS (picture archiving and communication software) system (NEOVISTA I-PACS; Konica Minolta).

Radiological assessment of (A) leg-length discrepancies and angular deformities on full-length standing digital radiographs and (B) bone growth on lateral radiographs. a, most lateral edge of the acetabulum; b, tip of the medial malleolus; c, most posterior point of the Blumensaat line; d, anterior border of the tibial joint surface. HKA, hip-knee-ankle (the angle between the mechanical axis of the femur and the tibia).
Results
Clinical Evaluation
The average increase in body height between the preoperative period and the last follow-up was 9.7 cm (range, 2.5-14.8 cm) (Table 1).
Patient Chacteristics and Clinical Data From the Subjective and Arthrometric Evaluations a

a F, female; M, male; SSD, side-to-side difference at 13.6 kg (30 lb).
b Growth from time of surgery to the latest follow-up.
Clinical examination revealed no limitation in the range of motion in any patient. The mean Lysholm score was 95, and the mean scores on the visual analog scale were 90 (Activities of Daily Living) and 81.3 (Sports/Recreation activities). The 2 boys were able to return to their previous sports activities. The girl had played softball before her ACL injury. She returned to her preinjury level at 1 year after the surgery but dropped her sports activity because of knee pain at the patellofemoral joint and the graft harvest site at the last follow-up.
At the 1-year follow-up, only 1 patient had a grade 1 positive score on the pivot-shift test, but at the last follow-up, all 3 patients had a grade 1 positive score on the Lachman test; the pivot-shift tests revealed a grade 1 positive score in 2 of the 3 patients. The mean side-to-side difference (SSD) at 13.6 kg (30 lb), measured by KT-1000 arthrometer, was 1.3 ± 0.5 mm at 1 year, but it increased to 2.5 ± 0.2 mm by the last follow-up (Table 1).
Radiological Assessment
Morphometric results are listed in Table 2. The mean increase in the tibial plateau width on anteroposterior knee radiographs was 4.2 mm over an average of 4 years. The mean increase in the distance between the anterior border of the tibial joint surface and the most posterior point of the Blumensaat line was 5.7 mm (range, 1.5-10.3 mm).
Radiological Assessment of Limb Alignment and Length a

a Negative symbol indicates valgus deformity of the operated knee. AMBL, distance from the anterior border of the tibial joint surface to the most posterior point of Blumensaat line; F, female; M, male; TPW, tibial plateau width.
b Side-to-side difference between the lateral margin of the acetabulum and the medial malleolus of the operated side and the nonoperated side.
c Growth from time of surgery to the latest follow-up.
On full-length standing radiographs, the distance between the lateral margin of the acetabulum and the medial malleolus of the operated limb was longer than that of the nonoperated limb in all 3 patients by an average of 4.8 mm. Varus deformity of <3° in the operated versus nonoperated limb was observed in 1 case.
Discussion
This is the first report of an all-epiphyseal double-bundle ACLR in skeletally immature patients, although it was a small series with only 3 cases. Anderson 2 originally performed an all-epiphyseal single-bundle ACLR in 2003 on 12 patients with a mean age of 13.3 years. Subsequently, several authors 7,9,17,18 have modified and refined this technique and have reported good objective clinical results. According to Koch et al 14 however, KT-1000 arthrometer measurements revealed an SSD of >3 mm in a high percentage of patients, and 3 of 13 knees sustained graft failure on midterm evaluation of the Anderson technique. In comparison with the clinical results of adult cases, the overall complication rate after ACLR in skeletally immature patients seemed to remain high. Although whether the double-bundle reconstruction technique is superior to the single-bundle reconstruction technique remains an issue of controversy from a clinical standpoint, several cadaveric biomechanical studies 13,16,25 –27 and a recent review 19 have demonstrated the superiority of double-bundle reconstruction techniques in the restoration of knee stability, especially with regard to rotational stability. Therefore, we expected a similar level of superior stability and functional outcome, even in pediatric ACL injuries, by a more anatomic reproduction of the AMB and PLB of the ACL. 24 In comparison with single-bundle reconstruction, double-bundle reconstruction with the transphyseal technique carries a higher risk for iatrogenic physeal injury in children with open physes. 23 We therefore created all 4 bone tunnels in an all-epiphyseal manner, despite the technical difficulties of this technique.
There have been few clinical reports of double-bundle ACLR with transepiphyseal technique 24 or partial physeal-sparing techniques, as opposed to a complete physeal-sparing technique, in skeletally immature patients. 15,22 Koizumi et al 15 evaluated the clinical outcomes of double-bundle ACLR in 15 adolescents at Tanner stages III and IV of physical development, in which the AMB of the femoral side was passed via an over-the-top route, and these outcomes were compared with those of 40 adult cases. Koizumi et al noted that their clinical results were similar to those in adult cases, but the rate of positive scores on the manual laxity test and the rerupture rate tended to be higher in the adolescent cases, although the differences were not significant. Our 3 patients achieved restoration of knee stability by 1 year after ACLR; however, KT-1000 arthrometer measurements revealed deterioration of the SSD, although the anteroposterior laxity of the operated knee was <3 mm in all cases. In addition, growth disturbances such as overgrowth and varus angulation were found in varying degrees in 2 of the 3 patients, although intervention was not necessary. Thus, our all-epiphyseal double-bundle ACLR technique did not yield expected clinical results in the midterm evaluation.
During a growth spurt, bones and joints rapidly grow wider and longer, thereby extending the distance between a femoral tunnel exit and a tibial tunnel exit. Therefore, we used the anteroposterior distance between the anterior margin of the tibial joint surface and the most posterior point of the Blumensaat line as the simulated length of the AMB. Its length extended by an average of 5.7 mm, with patient height increasing concurrently by an average of 9.7 cm. Very little is known about the behavior of the graft as related to the postoperative growth of patients. 4 Although some literature suggests that the graft would be expected to grow along with the patient, 4 a recent study has demonstrated a significant decrease in the graft diameter at 1 year after ACLR in patients at Tanner stages II to IV; thus, the newly reconstructed ligament is thought to stretch without hypertrophy. 3 In our patients, the stability of the reconstructed knee might be impaired because of excessive stretching of the graft in association with bone growth.
Another possible explanation is that the acute angle between the graft and the tunnel leads to stress concentration at the tunnel exit, 20 resulting in graft abrasion or thinning similar to a “killer-turn” effect in posterior cruciate ligament reconstruction. Because femoral and tibial tunnels run in the horizontal direction within the epiphysis, the graft bending angle was steeper than that used in ACLR in adults or in transphyseal reconstruction. In comparison with single-bundle reconstruction, the thinner size of the graft in double-bundle reconstruction may have increased this adverse effect in our cases.
Physeal-sparing techniques are intended to avoid iatrogenic physeal injury and the resultant growth disturbance. However, recent reviews have revealed that physeal-sparing techniques are not without risk, 1 and 1 meta-analysis 11 showed that the rate of growth disturbance was higher after physeal-sparing procedures than after transphyseal procedures. Collins et al 6 conducted a systematic review to identify all reported cases of growth disturbances after ACLR in patients with open physes, and they found that the overall percentage of limb-length discrepancies or angular malformation was 13% (39 cases) among the 313 patients included across the 21 studies. Most cases of limb-length discrepancies in physeal-sparing ACLR involved limb lengthening, which was attributed to increased vascularity and mitotic activities within the physes, as would occur after a diaphyseal femoral fracture in a child. In all 3 of our patients, we found that the operated limb was longer than that of the nonoperated limb by an average of 4.8 mm; a lengthening of 9.0 mm was observed in 1 case. Because our surgical technique entailed the creation of 4 epiphyseal tunnels instead of 2, increased vascularity could have increased growth. In addition, creating multiple tunnels within the restricted space of the epiphysis was technically demanding, which could have increased the risks for the iatrogenic injury.
Collins et al 6 stated that the most common angular malformation was valgus malalignment and that only 3 of 16 patients had a varus deformity. Of the 3 patients with varus deformity, 2 had undergone a physeal-sparing procedure, but the cause of the angular deformity was unspecified. 5,14 In our cases, we found a slight varus deformity of the operated limb in 1 case (patient M1). This patient showed a gradual decrease in posterior tibial slope in addition to the decrease in medial tibial proximal angle; therefore, the varus angulation was probably caused by the physeal violation at the anteromedial aspect of the proximal tibial physis that resulted from drilling of the bone tunnels or the graft fixation across the physis, which might have some influence on the development of the varus malalignment.
The major limitation of this study was that it included only 3 patients. As explained previously, however, the midterm results after physeal-sparing double-bundle ACLR were not what we expected in any of these patients. We have therefore discontinued this technique in skeletally immature patients, and thus we do not have findings from a larger patient population. Although the clinical superiority of double-bundle over single-bundle ACLR is debatable, the double-bundle technique is the one generally used for adult ACL injury. We therefore inferred that other surgeons may try double-bundle ACLR in children with open physes hereafter. Despite our study being based on only 3 patients, we believe that our findings provide meaningful information.
Conclusion
This study was an evaluation of the midterm results of all-epiphyseal double-bundle ACLR on 3 skeletally immature patients. Although outcomes were generally satisfactory 1 year after surgery, knee stability deteriorated somewhat by the last follow-up. Growth disturbances such as overgrowth and varus angulation were found in varying degrees in 2 of the 3 patients, but no intervention was required. Because of the limited number of patients, our results should be interpreted carefully. We recommend caution in treating children with all-epiphyseal double-bundle ACLR. Although the importance of anatomic ACLR is evident, the benefits from double-bundle reconstruction must be weighed against the potential risks, such as graft elongation and growth disturbance.
Footnotes
Acknowledgment
The authors are grateful to Professor Kunihiko Mabuchi (Tokyo University, Tokyo, Japan) for critical reading of the manuscript and helpful suggestions.
Final revision submitted November 13, 2019; accepted December 17, 2019.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.