
Abstract
Background:
Despite the increasing international popularity of CrossFit, there is a paucity of scientific evidence on the risk of CrossFit-related musculoskeletal injuries (CRMIs).
Purpose:
To investigate the incidence (cumulative incidence proportion [IP] and incidence density [ID]) of CRMIs and the association of CRMIs with personal and training characteristics.
Study Design:
Descriptive epidemiology study.
Methods:
A prospective, 12-week descriptive epidemiology cohort study was conducted in a convenience sample of CrossFit facilities in a single Brazilian city. Printed baseline questionnaires were distributed to 13 CrossFit boxes. All participants who filled out the questionnaire and consented to participate in the study were invited to respond to an online follow-up questionnaire every 2 weeks to collect data on CrossFit training characteristics and CRMIs. A CRMI was defined as any self-reported musculoskeletal injury or pain that prevented an athlete from exercising for at least 1 day. The IP was defined as the number of new cases divided by the entire population at risk, while the ID was defined as new events divided by the total person-time exposure in hours. Logistic mixed models were developed to investigate the association of CRMIs with personal and training characteristics.
Results:
A total of 515 CrossFit participants filled out the baseline questionnaire and provided informed consent, and 406 (78.8%) completed at least 1 follow-up measure. There were 133 participants who reported at least 1 CRMI during the study, and a total of 247 unique and new CRMIs were reported over a total estimated person-time exposure to CrossFit of 13,041 hours. The IP was 32.8% (95% CI, 28.4%-37.5%). The ID was 18.9 (95% CI, 16.6-21.3) per 1000 hours of CrossFit exposure. The shoulders (19.0%; n = 47) and lumbar spine (15.0%; n = 37) were most affected. Muscle injuries (45.3%; n = 112) and joint pain (24.7%; n = 61) were the most common CRMI types reported. Switching between prescribed and scaled down training loads (odds ratio [OR], 3.5 [95% CI, 1.7-7.3]) and previous injuries (OR, 3.2 [95% CI, 1.4-7.7]) were risk factors for a CRMI, while CrossFit experience was identified as a protective factor (OR, 0.7 [95% CI, 0.5-1.0]).
Conclusion:
In this 12-week prospective study, the ID was 18.9 CRMIs per 1000 hours of exposure; switching between training loads and previous injuries was associated with 3.5- and 3.2-fold higher odds, respectively, of sustaining CRMIs.
Physical benefits related to high-intensity interval training 8,24 and a sense of community have led CrossFit to an unprecedented level of global popularity. 39 CrossFit is a strength and conditioning exercise program with constantly varied multiarticular functional movements and high-intensity intermittent exercise sessions designed to improve fitness and health. 16,31 One of the most distinctive elements of CrossFit is that its exercises are multifaceted; that is, activities can include weight lifting, gymnastics, running, biking, plyometric training, and rowing. 16,31
Part of the popularity of CrossFit is its claim that the exercise program is suitable for everyone: professional athletes, pregnant women, the elderly, teenagers, and people with disabilities. 15,16 All participants, called “athletes” according to CrossFit philosophy, share the same exercise space, called a “box,” independent of their skill level. Each box’s head coach designs the workout sequence and intensity using his or her methodology and personal experience, and then, individual class coaches help athletes execute these workouts, offering additional assistance as needed. 16 However, adaptations and assistance are not always carried out in a standardized way, meaning that while each box follows the same principles, athletes’ particular workouts vary according to their perceived skill level, the box that they attend, and the head coach or class coach with whom they exercise at a given moment.
As CrossFit has been gaining in popularity, so has the scientific evidence on this exercise program. 2 While several authors have demonstrated the benefits of practicing CrossFit, 10,29,31 others have found a disproportionate musculoskeletal injury risk. 3 The prevalence of CrossFit-related musculoskeletal injuries (CRMIs) has been found to range from 19.4% to 73.5% in periods of time between 6 and 18 months, while the incidence of CRMIs has been estimated to vary from 2.1 to 3.1 injuries per 1000 hours of exposure. 12,17,26 –28,34,39 However, most of these previous studies used a retrospective design, which hampers conclusions on incidence estimates. 17,26,27,34,38 Prospective studies are considered the most appropriate design for studying the incidence of health-related conditions, 32,40 including sports injuries. 18,37 In addition, a systematic review has found that existing evidence on CRMIs is of low quality because of the studies’ high risk of bias. 7
We designed and conducted this study after becoming aware of the low-quality evidence on CRMIs and the paucity of prospective studies on the epidemiology of CRMIs, observing a number of CRMIs in our clinical practice, and learning about CrossFit workout variations in greater detail. The objectives of this study were (1) to investigate the incidence rates (cumulative incidence proportion [IP] and incidence density [ID]) of CRMIs and (2) to examine the association between CRMIs and personal and training characteristics of CrossFit athletes in a metropolitan area of Brazil.
Methods
Study Design
This article presents the results of a prospective, 12-week observational cohort study with 6 biweekly repeated measures. The study was conducted in 2016 and 2017 under the supervision of sports medicine researchers from a local university. We selected participants from CrossFit boxes in a single metropolitan area of Brazil after obtaining ethical approval from the relevant local ethics committee.
Population Sample, Setting, and Eligibility Criteria
This study population was made up of a convenience sample of general CrossFit athletes in a single metropolitan area of Brazil. Adults aged ≥18 years and who participated in physical exercise at CrossFit boxes were eligible to participate in this study. Participants were not eligible for this study if they provided incomplete data on the baseline questionnaire or if they reported an existing injury at baseline. The informed consent form and research team contact information were attached to the printed baseline questionnaire. All athletes who voluntarily signed the informed consent form agreeing to participate in this study and who met all eligibility criteria were included in this study. Participants could withdraw from the study at any time either by communicating their desire to research staff or by neglecting to fill out the follow-up questionnaires.
Data Collection
All included participants received a paper baseline questionnaire in the CrossFit box where they were training. The baseline questionnaire collected personal variables (ie, age, sex, weight, and height), exercise variables (ie, CrossFit experience, coaching variation, use of protective equipment, preventive exercises, stretching exercises, competitions, demonstration of the proper form to perform CrossFit exercises, and practice of other sports), and data on previous injuries.
An online questionnaire was then administered to collect follow-up data on time-dependent variables (ie, hours of CrossFit exposure and type of workload) and the emergence of new CRMIs and their characteristics (ie, type, body location, symptoms, and missing CrossFit training days because of a CRMI). The follow-up questionnaires were developed and administered with an online tool (SurveyMonkey [www.surveymonkey.com]). A total of 6 follow-up questionnaires were sent to all included participants, once every 2 weeks, during the 12-week follow-up period.
CRMI Definition and Classification
A CRMI was defined as any musculoskeletal injury or pain (in joints, bones, ligaments, tendons, or muscles) that prevented an athlete from exercising for at least 1 day. This time-loss injury definition is similar to that in a previously reported study on CrossFit. 17 Injuries were self-reported and classified by (1) body location (head, back, shoulders, elbows, wrists, hands, hips, thighs, knees, legs, ankles, feet, or other location); (2) type (concussions, cramps, cuts, fractures, muscle soreness, sprains, tendinitis, or other); (3) severity, defined as the number of consecutive missed training days (mild: 1-3 days; moderate: 4-7 days; severe: >7 days); and (4) pain severity, measured using the 11-point Numeric Rating Scale (NRS), ranging from 0 (no pain) to 10 (severe pain).
CrossFit Exercise Sessions
All exercise sessions were planned by the corresponding box’s head coach and were carried out in CrossFit boxes. Each CrossFit session was estimated to last, on average, 60 minutes, and 2 levels of training loads were offered: as prescribed (“Rx”), meaning that the workout weights and movements should be performed as prescribed, or “scaled,” referring to weights and movements scaled down by the head coach for those not able to perform the Rx workout. This study used the concept of “training load” as a composite measure of exercise frequency, duration, and intensity. Therefore, the categories of Rx and scaled workouts were used to measure external training loads in our participants. In CrossFit, workout loads (ie, Rx or scaled) are sex-specific, meaning that the actual absolute load is different between sexes.
Primary and Secondary Outcomes
The primary outcome of this study was the incidence of CRMIs (measured as both the IP and ID), while the secondary outcomes were characteristics hypothesized to be associated with CRMIs. Characteristics statistically associated with higher odds of developing CRMIs were considered risk factors, while those statistically associated with lower odds of developing CRMIs were considered protective factors. Before running the association analysis, we discussed the rationale and relevance of including each collected variable in the model. The consensual variables were age, sex, weight, previous injuries, CrossFit experience, training workload (Rx, scaled, or alternating Rx/scaled), stretching exercises, preventive exercises, use of protective equipment, coaching variation, demonstration of the proper form to perform CrossFit exercises, competitions, and practice of other sports. Exercises related to injury prevention included any warm-up exercises, core strength training exercises, or rotator cuff strengthening exercises performed in a CrossFit box. Protective equipment included any external equipment used by participants, such as gloves, knee braces, back support, or wrist wraps.
Statistical Analysis
Descriptive analyses were conducted to summarize the characteristics of the sample. Results were presented as the mean and 95% confidence interval (CI) for numeric variables presenting a normal distribution. The median and interquartile range (IQR) were used to summarize numeric variables not presenting a normal distribution. The normal distribution was investigated through an inspection of histograms and probability distribution functions. Frequencies and percentages were used to summarize dichotomous and categorical data. Linear and linear probability mixed models were conducted to summarize the follow-up measures data for numeric and dichotomous variables, respectively, to account for the dependency within participants’ observations. 36 Results were expressed as percentages and presented as weighted means for linear models and as mean probabilities for linear probability models.
The incidence of CRMIs was analyzed using 2 measures: IP and ID. The IP was defined as the number of new cases (participants reporting new CRMIs) divided by the entire population at risk and reported as a percentage. 14 The ID was defined as new events (number of CRMIs) divided by the total person-time exposure to CrossFit exercises in hours and reported as the number of CRMIs per 1000 hours of CrossFit exposure. 18 Furthermore, 95% CIs were estimated for all measures to provide greater information about the uncertainty inherent in each calculation.
Logistic mixed models were developed to investigate the association of CRMIs with personal and training characteristics. The dichotomous CRMI variable for each time point’s measure was used as the dependent variable, and a time-lag technique was applied to ensure that the time-dependent predictors (ie, independent follow-up training variables in the model) happened in the biweekly period before the CRMI report (ie, onset). 14,20,35 A study identification code for each participant, the CrossFit training box, and year of data collection (ie, 2016 or 2017) were included as random effects to account for the repeated nature of the follow-up data and possible CrossFit box and time-period cluster effects. There were 2 models constructed: (1) a full model including all a priori established predictors deemed by us to be relevant for the CRMI risk analysis and (2) a final model using backward variable selection and the Bayesian information criterion to remove or maintain the variables in the model. Results were presented as odds ratios (ORs) and their 95% CIs. All analyses were conducted in Excel (Excel for Mac 2011, Version 14.7.3; Microsoft) and R 3.5.0 (R Foundation for Statistical Computing).
Results
Participants and Response Rate
A total of 800 baseline questionnaires were physically distributed to 13 CrossFit boxes in the selected city, where coaches had been familiarized with the study design and had agreed to participate. Of those 800 paper baseline questionnaires, 515 were filled out and returned by the same number of participants (64.4%). Of the 515 who returned the baseline questionnaire, 63 (12.2%) participants did not meet the eligibility criteria (46 [8.9%] returned questionnaires with incomplete data, and 17 [3.3%] already had injuries at baseline). The remaining 452 (87.8%) of the baseline responders who signed the informed consent form and met all eligibility criteria were included in this study. From the 452 participants, 46 were excluded from final analyses (dropout rate of 10.2%): 39 (8.6%) because they did not return a single follow-up questionnaire and 7 (1.5%) because they withdrew consent during the study. Therefore, the final sample included in the analyses was composed of 406 CrossFit athletes (78.8% of those who filled out the informed consent form). The response rate of the 406 participants was, on average, 68.1% (IQR, 54.9%-83.9%), meaning that each participant returned about 4 of 6 biweekly follow-up questionnaires, on average. The recruitment process, application of inclusion/exclusion criteria, and makeup of the final sample size are detailed in Figure 1.
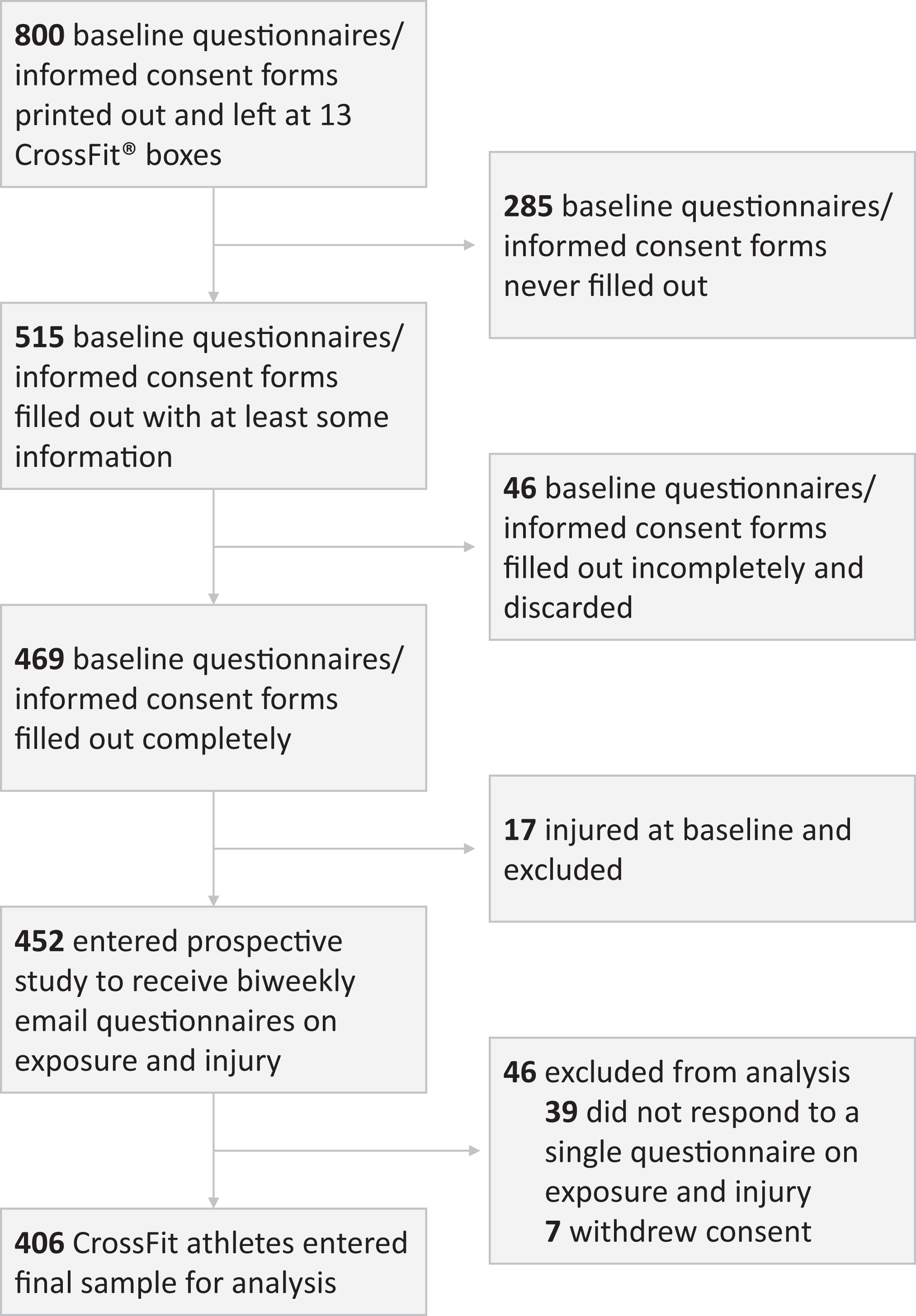
Flow diagram of recruitment, inclusion/exclusion, and final sample composition.
The sex distribution was balanced in our sample: 198 men (48.8%) and 208 women (51.2%). Participants reported a mean age of 32.1 years (95% CI, 31.4-32.8), a mean weight of 74.3 kg (95% CI, 72.9-75.7), and a mean height of 1.7 m (95% CI, 1.7-1.7). The median experience exercising at a CrossFit box was 1.0 year (IQR, 0.5-1.8). A breakdown of all baseline results can be found in Table 1.
Baseline Characteristics of CrossFit Athletes (N = 406) a

a IQR, interquartile range.
CrossFit Exposure
The mean exposure to CrossFit was 3.9 days per week (95% CI, 3.8-4.0) (Table 2). Most participants (51.5% [95% CI, 46.7%-56.4%]) had a scaled training load, followed by alternating Rx and scaled (27.1% [95% CI, 22.8%-31.5%]), while the lowest proportion exercised consistently with an Rx training load (21.3% [95% CI, 17.3%-25.3%]). Each CrossFit training session is supposed to last approximately 1 hour. The total person-time exposure to CrossFit was 13,041 sessions, equivalent to approximately 13,041 hours.
CrossFit Exposure and CrossFit-Related Musculoskeletal Injuries During Follow-up a

a Results were obtained from mixed models, except for “missed CrossFit sessions.” Rx, prescribed.
b The total number of CrossFit-related musculoskeletal injuries was 247, and the estimated total person-time exposure to CrossFit was 13,041 hours.
CRMI Incidence and Severity
A total of 133 of the 406 participants analyzed reported at least 1 CRMI during this 12-week prospective study. Therefore, the IP of CRMIs was 32.8% (95% CI, 28.4%-37.5%) (Table 2). There were 247 unique and new CRMIs reported during this study over a total estimated person-time exposure to CrossFit of 13,041 hours. Therefore, the estimated ID was 18.9 (95% CI, 16.6-21.3) CRMIs per 1000 hours. These CRMIs presented a mean pain level of 5.0 (95% CI, 4.7-5.3) on a 0-to-10 NRS, and 40.2% (95% CI, 32.8%-47.6%) of the CRMIs required medical attention (Table 2). Shoulders (19.0%; n = 47), the lumbar spine (15.0%; n = 37), and knees (11.7%; n = 29) were the most affected body locations (Figure 2). Muscle injuries (45.3%; n = 112), joint pain (24.7%; n = 61), and tendinopathies (13.0%; n = 32) were the most frequent types of CRMIs (Figure 3).

Anatomic sites most affected by CrossFit-related musculoskeletal injuries.

Most common types of CrossFit-related musculoskeletal injuries.
CRMI Association Analysis
The analysis associating CRMIs with personal and training characteristics is presented in Table 3. The final model yielded alternating Rx and scaled training loads (OR, 3.5 [95% CI, 1.7-7.3]) and previous injuries (OR, 3.2 [95% CI, 1.4-7.7]) as risk factors for a CRMI, while a 1-year increase in CrossFit experience (OR, 0.7 [95% CI, 0.5-1.0]) was found to be a protective factor against CRMIs. The associations of CRMIs with the other characteristics investigated were not statistically significant.
Association Between CrossFit-Related Musculoskeletal Injuries and Personal and Training Characteristics a

a Data are shown as odds ratio (95% CI). Results were obtained from logistic mixed models. Dashes signify that variables were not included in the final model. Rx, prescribed.
b Statistically significant.
Discussion
CRMI Incidence
The IP reported in our study (ie, 32.8%) lies within the range of those in previous reports: similar to the IP reported by Feito et al 9 (30.5%), higher than that in Weisenthal et al 38 (19.4%) and Montalvo et al 27 (26.0%), but lower than that in Mehrab et al 26 (56.1%) and Hak et al 17 (73.5%). Different study designs, methods, source populations, and/or contexts may explain these discrepancies. For instance, the data in the previously mentioned studies were collected retrospectively, which, according to the literature, may bias interpretations and conclusions surrounding incidence. 18,37 Another possibility is differences between boxes and styles of training. While CrossFit boxes are not franchises per se, boxes are affiliates in a confederation, providing the same branded fitness regimen. However, all boxes receive the same training course, and there is no evidence that there are marked differences between Brazilian and American boxes in terms of how they are run or the implications for these findings.
The ID found in our study (18.9 CRMIs per 1000 hours [95% CI, 16.6-21.3]) was almost 10 times higher than most previous reports (all per 1000 hours of exposure): 2.4, 2.3, and 2.1. 12,27,28 We hypothesized that this discrepancy might be explained by differences in the methods and by the definition of injury used. We used a longitudinal surveillance method with repeated measures that should have reduced the probability of underreporting minor or overuse CRMIs by minimizing recall bias. Given that prospective studies are typically more sensitive, studies using similar approaches have also found higher sports injury rates. 6,21,22 For example, Clarsen et al 6 reported that a surveillance system based on a longitudinal and repeated prospective measures design was able to capture more than 10 times as many sports injuries as traditional methods. In addition, we suggested a more inclusive CRMI definition (ie, any musculoskeletal injury or pain that prevented an athlete from exercising for at least 1 day) compared with the ones used by Weisenthal et al 38 and Mehrab et al 26 (ie, >7 missed days, training adaptation for >2 weeks, or a need for medical attention). We believe that identifying a higher number of minor or overuse injuries may be advantageous for secondary sports injury prevention, as it may create a possibility for early identification, thereby reducing the risk of an injury progressing.
Risk and Protective Factors for a CRMI
In this study, alternating between Rx and scaled training loads and previous injuries were found to be risk factors for a CRMI. We suggest that alternating training load intensities—in this case, switching between Rx and scaled workouts—could be explained by a lack of skills in maintaining Rx intensities or a lack of awareness of the athletes’ limitations. CrossFit experience may mitigate the first argument, and indeed, we saw that more CrossFit experience reduced the odds of sustaining CRMIs. Regarding the second argument, recognizing limitations and adjusting exercises accordingly are not simple endeavors, as both athletes and coaches must not only adapt weight loads, but also dynamically adapt, vary, and increase the intensity, frequency, and duration of workouts to achieve athletes’ goals.
Interestingly, while alternating training loads was identified as a risk factor for CRMIs, athletes training consistently with Rx or scaled workouts were not significantly different in terms of the CRMI risk in this study. It is likely that alternating training loads, especially increasing from scaled to Rx, increases the number of spikes (ie, acute increases) in the training load, while maintaining the training load category may result in more gradual progress within that specific category. Evidence has shown that spikes in the training load may indeed increase the risk of sports injuries, 23,25 which may partly explain why alternating training loads can result in a higher CRMI risk. Most CrossFit novices initiate their training with scaled (or even lower) training loads. We are not suggesting that they should not aim to progress to Rx training loads but rather that they should pay extra attention during the transition period in terms of injury prevention.
There is strong evidence that previous injuries increase the risk of future injuries in several sports. 1,13,14,33 Our results suggested that CrossFit is no exception: in our study, reporting a previous injury was associated with about 3-fold higher odds of sustaining a CRMI. This estimate is consistent with those reported by Chachula et al 5 and Moran et al. 28 There are 3 possible hypotheses for this finding: (1) scar tissue, (2) inappropriate acute/chronic load balance recovery, or (3) diagnostic/treatment factors. Several authors have argued that scar tissue can contribute to future muscular imbalance, a reduction in flexibility, and mechanical or functional instability. 11 Others have hypothesized that athletes may inadequately balance acute and chronic loads because of time spent away from exercise programs. 4,30 We also hypothesize that several of the previous injuries reported in our study could have remained undiagnosed and untreated until the participants reported them in our online surveillance system. In this case, certain CRMIs measured during this study could have been relapses or sequelae of previous injuries.
We found that a 1-year increase in CrossFit experience reduced the odds of sustaining a CRMI by approximately half. Our results contradicted the findings of Montalvo et al, 27 who found that more CrossFit experience (in years) was associated with higher odds of sustaining a CRMI. However, the study of Montalvo et al 27 was retrospective, which could have introduced bias in their analysis. It seems reasonable to assume that more experienced athletes manage loads and the injury risk better than inexperienced ones. 19 This should, however, be confirmed with data, as it is also entirely possible that CrossFit athletes who have been injured or who are prone to injuries have already dropped out by 1 year. Therefore, the discrepancy found between our study and the literature in this regard may provide an opportunity for future studies.
Strengths
The main strengths and novelties of this study included (1) a prospective and repeated measures design and analysis and (2) collecting and monitoring CrossFit-specific characteristics. This study’s prospective nature and repeated measures provided an opportunity to collect and monitor data with a lower risk of bias, such as recall bias, an issue reported in a recent systematic review on the topic. 7 Investigating CrossFit-specific characteristics, such as CrossFit experience, training load (ie, Rx and scaled), preventive exercises, use of protective equipment, coaching variation, and participation in competitions, is relevant and important to better describe, report, understand, and explain the CrossFit practice and its association with the CRMI risk.
Limitations
The limitations of this study were mainly related to the use of a convenience sample and the self-reported nature of the study. A random selection from the source population is the recommended method for selecting a study sample. However, epidemiological studies, such as ours, may face recruitment challenges that make the proper execution of these studies all but impossible. We did not have control over or access to the entire CrossFit population in our city. Therefore, drawing a random sample from this entire population would not be possible. Our strategy to overcome this issue and reduce the probability of having a nonrepresentative sample was to invite all CrossFit boxes we could contact and include and monitor the highest number of participants possible using an online tool. We do not have reason to believe that our sample was not representative of the CrossFit population in our city, but we are aware that our study could have been affected by this possible selection bias. Additionally, given that we left the printed baseline questionnaires/informed consent forms out in the boxes for athletes to choose at will, we recognize that there may have been response bias caused by those who decided to participate having different characteristics from those who decided not to participate. Self-reported data may be prone to detection bias, especially when these data include information on health conditions, such as sports injuries. Therefore, another limitation of this study was the self-reported method employed to collect the data: there was no medical assessment to diagnose the CRMIs officially. Because of the large geographic area coupled with a short period of repeated measures, in-person visits by health care professionals was not possible with our resources. Our strategy to minimize this bias as much as possible was to develop a multipronged strategy to classify the injured athletes. For instance, athletes were questioned about their CRMIs and also asked to describe how many days of training were missed to corroborate that the injury actually led to missed training. Also, the researchers responsible for cleaning the data checked each response, cross-checking the CRMI information with the type and body region reported, to identify possible inconsistencies. Finally, we recognize that 12 weeks may be suboptimal to measure CRMIs; now that we have identified the variables that most affect the CRMI incidence, we intend to implement a future study with these variables and much longer follow-up times. A longer study duration may also allow us to draw temporal conclusions around our current finding that more CrossFit experience is associated with a lower risk. This longer study period could clarify if injuries decrease in the same athlete over time or if those who sustain more CRMIs abandon the exercise altogether.
Implications for Practice
Maintaining a physically active lifestyle is beneficial for health. We believe that the popularity of CrossFit creates an opportunity to engage people in physical fitness or keep them physically active, helping to achieve health benefits. However, no intervention comes without risks, and we hope that the results of this study may help the community better understand the musculoskeletal risk associated with CrossFit. We do not believe that this risk surpasses the health benefits that can be achieved with CrossFit, but a better understanding of the risks associated with CrossFit may help to implement a safer exercise program. In addition, we believe that specific information on CrossFit characteristics, a novel aspect of this study, may be useful for future endeavors in developing and implementing tailored CRMI prevention strategies.
Before concluding, we wish to further contextualize this study and its motivations. This study was conducted by orthopaedic surgeons, many of whom are enthusiastic participants in CrossFit and began to see higher injury rates in both their daily clinical and exercise practice than those rates reported in the literature. This study was, therefore, designed to better understand the reality of CrossFit athletes in Brazil and not to evaluate the exercise program or make a value judgment on its philosophy. We believe that CrossFit provides an important and interesting set of functional exercises, as well as a community setting in which to exercise with like-minded people interested in maintaining a healthy lifestyle. We also believe that orthopaedic surgeons and physical therapists should have access to clear and transparent data on CRMIs to better advise their patients and provide preventive counseling. This study should, therefore, be interpreted in this light: as an objective presentation of the true injury experience of CrossFit athletes in several boxes of the São Paulo greater metropolitan area in Brazil.
Conclusion
In an urban Latin American population, about 1 in 3 CrossFit athletes sustained CRMIs in a 12-week training period. The estimated ID was 18.9 CRMIs per 1000 hours of CrossFit exposure (95% CI, 16.6-21.3). CRMIs presented, on average, low to mild severity in terms of pain and training time loss. CrossFit participants with alternating Rx and scaled training loads had 3.5-fold higher odds of sustaining CRMIs than those training with scaled loads. Similarly, those with previous injuries had 3.2-fold higher odds of sustaining CRMIs. On the other hand, the odds of sustaining a CRMI by those who have practiced CrossFit for at least 1 year were about half that of novice athletes.
Footnotes
Acknowledgment
The authors thank Elena Atkinson for her assistance in translating, editing, and formatting this work for publication.
Final revision submitted November 11, 2019; accepted December 3, 2019.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Federal University of São Paulo (reference No. CAAE 1.753.942).