
Abstract
Background:
Previous studies have evaluated the effect of distance to high-volume centers on outcomes after joint replacement. However, there is limited evidence on whether this distance has an effect on outcomes after undergoing hip arthroscopic surgery for femoroacetabular impingement syndrome (FAIS).
Purpose:
To determine whether increased distance from a patient’s home to his or her primary orthopaedic clinic has an influence on the ability to achieve the minimal clinically important difference (MCID) on outcome measures after surgery for FAIS.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective cohort analysis was performed on patients undergoing surgery for FAIS by a single surgeon from January 2012 through January 2017. A total of 692 patients were identified and split into 2 groups: driving distance of <50 miles from our institution (referral group) and driving distance of <50 miles from our institution (local group). Preoperative and 2-year postoperative scores on patient-reported outcome measures (PROMs), including the Hip Outcome Score Activities of Daily Living and Sport-Specific subscales, International Hip Outcome Tool–12, and modified Harris Hip Score, were assessed. Patients achieving the MCID on any included PROM were analyzed using a chi-square analysis. Logistic regression was performed to determine whether driving distance and other demographic variables of interest had an effect on achieving the MCID. Study data were analyzed using PatientIQ, a cloud-based research and analytics platform for health care.
Results:
There were 647 patients who completed 2-year follow-up and were included in the analysis. Of these patients, 116 (17.9%) were identified as being ≥50 miles from their orthopaedic provider, and 531 (82.1%) were identified as having a driving distance of <50 miles. A total of 100 patients (86.2%) in the referral group reached the MCID, and 476 patients (89.6%) in the local group reached the MCID. There was no statistically significant difference in reaching the MCID on any of the included PROMs between the 2 groups (P = .364). The same result held when controlling for a number of factors including age, body mass index, and adjusted gross income with logistic regression.
Conclusion:
When controlling for a number of factors including age, body mass index, and adjusted gross income, distance to a high-volume hip arthroscopic surgery center did not have an effect on postoperative outcome scores or achieving the MCID 2 years after undergoing surgery for FAIS.
Keywords
Health care delivery in the United States is continuously shifting toward a value-centric over volume-centric platform. 1,13 As this shift occurs, it is important to identify areas in health care fields that present an obstacle to reaching high levels of quality of care and successful outcomes for patients. A proposed model for streamlining and improving both quality of care and patient outcomes is the establishment of centers of excellence (COEs), where certain fields, procedures, and protocols are refined and combined to create a favorable environment for success for patients and providers alike. 31 Specific to the field of hip preservation surgery and hip arthroscopic surgery, there is evidence that hip arthroscopic surgery is associated with a steep learning curve and that outcomes are better when surgery is performed at high-volume centers and by high-volume surgeons. 24
Adopting this model presents challenges including increased travel distance for orthopaedic care by patients who may not have access to COEs in their region or state, which may negatively affect patient outcomes. In the oncological surgery literature, patients traveling farther for oncological surgery demonstrated a decrease in 90-day and 5-year mortality rates in a phenomenon deemed “travel distance bias,” which suggests that patients with increased travel distances are predisposed to improved outcomes. 34 However, the reverse of this phenomenon, deemed “reverse travel distance bias,” has been demonstrated in general surgery literature, with patients treated closer to home having less of a risk for complications and better outcomes than predicted. 8 The impact of travel distance on orthopaedic surgery outcomes is a growing area in need of investigation, as very few studies have examined the effect of distance traveled on patient outcomes. Most studies have focused on identifying outcomes in high-volume hospitals and compared them with outcomes at low-volume hospitals. Dy et al 7 evaluated over 2 million patients who underwent total hip arthroplasty or total knee arthroplasty (TKA) over a 15-year period and determined that the complication risk was higher if patients went to a local low-volume hospital. Other studies have indicated that complication and revision rates in TKA are similar in patients undergoing surgical treatment at regional or high-volume institutions. 22 Travel distance to high-volume institutions has been shown to not have an effect on the risk for complications in patients undergoing total joint replacement 29 ; however, to our knowledge, none has examined the effect of distance traveled to a high-volume institution on outcomes in the sports medicine specialty.
The primary purpose of this investigation was to determine the effect of increasing travel distances on achieving the minimal clinically important difference (MCID) on functional outcome measures after surgery for femoroacetabular impingement syndrome (FAIS). Treatment for FAIS represents a high-volume elective hip preservation procedure with protocols that are well-defined at our institution. It was hypothesized that increasing travel distances would significantly decrease the probability of a patient reaching the MCID on applicable patient-reported outcome measures (PROMs) after surgery for FAIS.
Methods
This study was approved by the institutional review board at the institution where the study took place, and no funding was received. Prospectively gathered data on all patients undergoing hip arthroscopic surgery for the treatment of FAIS from January 2012 to January 2017 by a single fellowship-trained surgeon (S.J.N.) were collected and analyzed. Inclusion criteria were patients with a clinical and radiographic diagnosis of symptomatic FAIS 12 who failed nonoperative treatment (ie, nonsteroidal anti-inflammatory drugs, physical therapy, avoidance of activities, hip injections), underwent primary hip arthroscopic surgery, and had a minimum 2-year follow-up. Exclusion criteria were patients without geographic demographic information (postal code or city of residency at the time of surgery), those with a history of concomitant ipsilateral or contralateral hip surgery, and patients undergoing hip surgery for concomitant abnormalities. General exclusions for surgery in our practice are evidence of osteoarthritis (Tönnis grade >1) or a history of pediatric hip abnormalities (slipped capital femoral epiphysis, Perthes disease, developmental hip dysplasia).
Surgical Technique
All hip arthroscopic procedures were performed by a single fellowship-trained hip surgeon at a high-volume academic hospital using a technique that has been well-described in the literature. 10,14,32 Briefly, standard anterolateral and midanterior portals were established under traction with the aid of fluoroscopic guidance. A 2-cm interportal capsulotomy site was created, and abnormalities were addressed in the central compartment. Depending on intra-articular findings, central compartment procedures included acetabuloplasty, labral repair, or labral debridement. Next, after traction release, the interportal capsulotomy site was extended inferiorly at the midpoint to create a T-capsulotomy site for access to the peripheral compartment. The medial and lateral leaflets of the iliofemoral ligament were retracted with sutures for increased visualization. Cam morphology was meticulously resected until an adequate femoral head-neck offset was achieved. Upon completion, a dynamic examination of the operative leg was performed to confirm an appropriate resolution of impingement. The capsule was then repaired using a suture shuttling system, and plication was performed depending on the degree of capsular laxity.
Postoperative Rehabilitation
All patients were started on a physical rehabilitation program on postoperative day 1 as previously described. 18,21 Patients went through a 4-phase rehabilitation protocol that lasted a mean of 16 to 18 weeks. Regardless of distance, access to postoperative physical therapy was established at the time of surgical clearance. Physical therapists were given the rehabilitation protocol, and patients were instructed to follow the postsurgical rehabilitation process.
Functional Outcome Evaluation
All patients in the study completed postoperative hip-specific PROMs, including the Hip Outcome Score–Activities of Daily Living (HOS-ADL) 23 and Hip Outcome Score–Sport-Specific (HOS-SS) subscales, the modified Harris Hip Score (mHHS), 2,15 and the International Hip Outcome Tool–12 (iHOT-12) 27 at a minimum of 2 years. In addition, all patients graded their pain level using a 0- to 100-mm visual analog scale at 2 years postoperatively.
To quantify the clinical significance of outcome achievement on the HOS-SS, HOS-ADL, mHHS, and iHOT-12, we applied the principles of the MCID as defined for functional PROMs. Prior work has proposed that the MCID be considered a minimum target for outcome improvement. 26 The HOS-ADL, HOS-SS, mHHS, and iHOT-12 threshold scores for achieving the MCID were determined using a distribution-based method by calculating the 0.5 standard deviation of the change in outcome scores over the 2-year time period, as described in the literature. 17,20,27,30 Patients were considered to have reached the MCID if they achieved this outcome endpoint on any of the administered questionnaires.
Assessment of Geographic Location
Because of the large metropolitan area where our institution is located, we assumed that any patient within 50 miles of the institution would have access to adequate physical therapy that followed the recommended rehabilitation protocol and that patients would be able to travel for postoperative follow-up. Thus, 50 miles was chosen, as this is approximately the distance cutoff between suburban and urban areas within our metropolitan area. As such, Google Maps application programming interface was utilized to systematically fetch travel distances between the patients’ postal codes and our institution. The group of patients who were <50 miles from the high-volume hospital where the senior author (S.J.N.) practices were labeled the local group, while patients who were ≥50 miles were labeled the referral group. Furthermore, for each postal code, published statistics from the US Internal Revenue Service were used to determine the average adjusted gross income (AGI) to determine whether income was an effect modifier on the association between geographic location and achieving the MCID. The year of the AGI corresponded to the 2-year follow-up date. For example, the 2014 AGI was calculated for those who underwent surgery in 2012. Of note, to prevent possible skewness in the results, patients living farther than the states bordering Illinois were dropped from the analysis (n = 22).
Statistical Analysis
All data were screened to determine whether they met parametric statistical assumptions before analysis. Descriptive statistics for all continuous variables are reported as the mean and standard deviation, and frequency statistics are reported for all noncontinuous variables. The paired-samples t test was used to compare preoperative and 2-year postoperative patient-reported outcome scores in patients with FAIS. The independent t test was performed to compare preoperative and postoperative functional scores between the 2 distance groups. Logistic regression was used to determine whether distance traveled has an effect on achieving the MCID. Common confounders of patient outcomes including age, sex, and body mass index (BMI) were included in the analysis as well as mean AGI. The Hosmer-Lemeshow goodness-of-fit test was used to verify that the model was not improperly specified. The Pearson goodness-of-fit statistic was computed to quantify the similarity of quantities for each grouping yielded by the model. This statistic follows a chi-square distribution. A low P value, implying dissimilarities in the groupings, indicates a poor fit.
Study data were analyzed using PatientIQ (https://www.patientiq.io), a cloud-based research and analytics platform for health care. The PatientIQ platform was designed to integrate disparate data sources, such as data residing in the electronic health record, and provide a real-time data exploration interface and advanced statistics engine. In addition, the platform also offers capabilities to capture data directly from patients, clinical staff, and researchers at various preoperative and postoperative time points using workflows specific to a given diagnosis and/or procedure. Using this integrated approach has allowed our group to explore predictors of achieving the MCID while leveraging a largely automated advanced statistical modeling platform.
Results
A total of 647 patients met the inclusion criteria and were included in the final analysis (Figure 1). The mean age and BMI of the entire study cohort were 34.6 ± 12.6 years and 25.0 ± 4.6 kg/m2, respectively. The mean distance from the hip arthroscopic surgery provider was 38.2 miles, with the majority (82.1%) identified as having a driving distance of <50 miles at the time of surgery. A comparison of demographics including age, BMI, and sex demonstrated no statistically significant difference between patients in the local and referral groups (Table 1). A comparison of the AGI between the 2 groups demonstrated that patients in the local group lived in geographic areas with significantly higher incomes than those in the referral group (112.1 ± 80.9 vs 65.7 ± 16.9 per US$1000, respectively; P < .001).

Flowchart of patients meeting inclusion and exclusion criteria. FAIS, femoroacetabular impingement syndrome; MCID, minimal clinically important difference.
Patient Demographics a

a Data are reported as mean ± SD or n (%). AGI, adjusted gross income; BMI, body mass index.
Comparison of Preoperative and Postoperative Outcome Scores
The paired t test of preoperative and postoperative functional outcomes demonstrated a significant improvement in all outcome and pain scores over the 2-year period in all patients (P < .001 for all) (Table 2). A comparison of preoperative scores between the local and referral groups demonstrated that those traveling a greater distance had significantly lower scores on the HOS-ADL (66.0 ± 18.1 vs 60.4 ± 19.0, respectively; P = .004), mHHS (58.9 ± 13.9 vs 53.9 ± 15.5, respectively; P = .001), and iHOT-12 (38.8 ± 18.0 vs 31.0 ± 15.2, respectively; P < .001). However, an analysis of 2-year outcome scores demonstrated no significant difference between the groups (P > .05 for all) (Table 3).
Overall Preoperative and 2-Year Postoperative Functional Scores a

a Data are reported as mean ± SD. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sport-Specific; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Preoperative and 2-Year Postoperative Functional Scores by Distance Group a

a Data are reported as mean ± SD. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sport-Specific; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Analysis of Achieving the MCID
The HOS-ADL, HOS-SS, mHHS, and iHOT-12 threshold scores for achieving the MCID were 9.6, 13.9, 9.2, and 13.6, respectively. The numbers of patients achieving the MCID are summarized in Table 4. Briefly, there was no statistically significant difference between groups in the proportion of patients achieving the threshold score for any of the PROMs (P > .05 for all). A total of 476 patients (89.6%) in the local group and 100 patients (86.2%) in the referral group achieved MCID by reaching at least 1 PRO score threshold. The chi-square analysis demonstrated that there was no statistically significant difference in the rates of achieving the MCID between the 2 groups (P = .364).
Chi-Square Analysis of Patients Who Achieved the MCID by Distance Group a

a Data are reported as n (%). HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sport-Specific; iHOT-12, International Hip Outcome Tool–12; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score.
Logistic Regression
An exploratory analysis demonstrated that the distributions of age, sex, and BMI between both groups of patients were not identical, suggesting that a chi-square analysis alone may not be sufficient in identifying an effect attributable to distance (Table 1). Overall, patients in the referral group tended to exhibit higher variances in age at surgery and BMI. The proportion of female patients in the referral group was also higher. Mean AGI had a high variance, and there appeared to be outliers in the local group. As a result, mean AGI was grouped into categories as well to diminish outlier influence.
The results of logistic regression are summarized in Table 5. Briefly, female sex (odds ratio [OR], 1.784 [95% CI, 1.055-3.017]; P = .030) was associated with achieving the MCID, while age 22 to 50 years (OR, 0.274 [95% CI, 0.105-0.714]; P = .008) and age >50 years (OR, 0.287 [95% CI, 0.092-0.892]; P = .031) were associated with not achieving the MCID. The binary variable for driving distance had a negative coefficient, indicating that patients traveling at least 50 miles from the high-volume home institution were less likely to achieve the MCID, holding other variables constant. However, this association was not statistically significant (P = .203). Mean AGI variables were weakly associated with achieving the MCID; however, they did not show statistical significance (range, P = .080-.369). The Pearson goodness-of-fit statistic demonstrated a chi-square statistic of 4.67 and a P value of .792, indicating that the model had a good fit.
Logistic Regression Analysis of Variables for Achieving Any MCID a
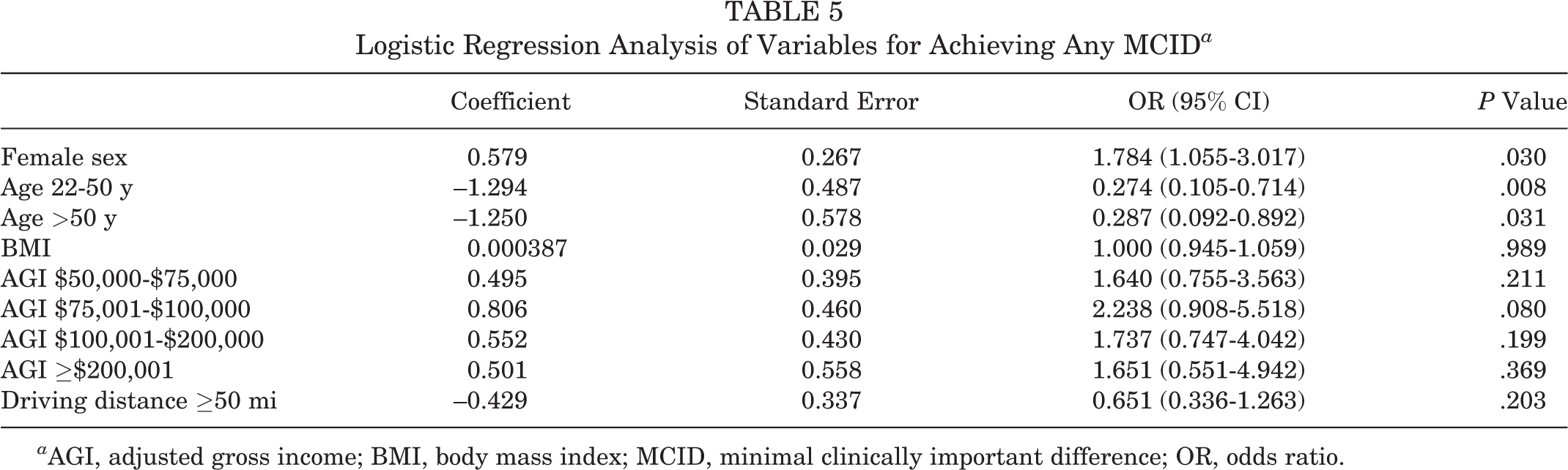
a AGI, adjusted gross income; BMI, body mass index; MCID, minimal clinically important difference; OR, odds ratio.
Discussion
The primary findings of this study are that patients who underwent hip arthroscopic surgery and were in close proximity to the high-volume hospital where the procedure took place had similar 2-year functional outcome scores and achieved the MCID at similar rates compared with patients who traveled farther to undergo hip arthroscopic surgery for FAIS. Of note, patients who traveled ≥50 miles for their care had lower preoperative HOS-ADL, mHHS, and iHOT-12 scores; however, there was no statistically significant difference in postoperative outcome scores. These findings suggest that travel distance does not significantly influence outcomes after hip arthroscopic surgery for FAIS. Moreover, patients traveling farther distances appear to have lower baseline functional status.
With the development of COEs and other high-volume institutions for orthopaedic surgery, a number of studies have examined whether undergoing surgery at these centers and subsequent follow-up affects outcomes. A National Institutes of Health study used the National Inpatient Survey to quantify trends in total hip arthroplasty and TKA with respect to shifts in surgical volume and complications. Over a 12-year period, the authors determined that patients were electing to have both procedures performed at higher volume hospitals, which manifested in lower complication rates. 19 Similar findings have been found in large studies across the world. In a study using a German health care database, the risk of revision was calculated among 45,165 TKA procedures performed over a 1-year time frame. The authors identified an increased risk of revision surgery in patients undergoing TKA in hospitals where fewer than 145 arthroplasty procedures were performed per year. 16 Studies have also analyzed the financial impact of undergoing total joint arthroplasty and have indicated that hospitals that perform fewer than 100 cases per year have higher hospital-specific charges as well as higher Medicare inpatient payments. 5 In the field of shoulder arthroscopic surgery, similar findings have been reported, with higher surgical complications, lengths of stay, and costs associated with low-volume surgeons and institutions. 35
Specific to the field of hip preservation surgery, prior evidence has shown that there is a relationship between surgeon volume and outcomes after hip arthroscopic surgery. Mehta et al 24 noted that surgeons performing a low volume of hip arthroscopic procedures (<97 in total career) had the highest risk for failed hip arthroscopic surgery and revision hip surgery. The prior study by Mehta et al, combined with the findings of our investigation, supports the argument for a COE for hip arthroscopic surgery. We posit that patients traveling increased distances to undergo surgery at these centers do not have an increased risk for complications but rather experience improved outcomes as a result of surgery being performed by a high-volume arthroscopic surgeon. It is worth noting that in the study by Mehta et al, the highest volume stratum (and the stratum with the lowest risk of failure) consisted of more than 519 career hip arthroscopic procedures. In the senior author’s practice, 500 to 600 hip arthroscopic procedures are performed annually, with well-reported excellent clinical outcomes. 3,6,9,33
Recent studies have examined the effect of referral or distance bias on outcomes at high-volume tertiary centers in patients undergoing TKA. Maradit Kremers et al 22 grouped 22,614 primary TKA procedures based on patients’ home postal codes and distance from the hospital where the initial procedure took place. Compared with local patients, those who traveled to the center were younger, had lower BMIs, were likely to have inflammatory arthritis or neoplasms as surgical indications, and had prior surgery on the same knee. However, the risk of complications, revision, and postsurgical knee instability was the same across all distance groups. 22 The authors described 2 types of referral bias: (1) if referred patients are sicker than their local counterparts, they will have worse outcomes; and (2) if referred patients are disproportionately healthier, their postoperative morbidity and mortality will be lower. 22 Previous studies have demonstrated that these biases are typically consistent, particularly within the general surgery specialty. 4,8,25,36 Although the current study demonstrated that patients in the referral group had lower preoperative functional scores, there was no significant difference in outcome scores or rates of achieving the MCID. 29 To ensure that patients undergo proper postoperative rehabilitation, the senior author provides patients with written instructions to bring to their physical therapist and provides the program on the practice’s website as well. We believe that both of these provide physical therapists sufficient access to standardized postoperative therapy for all of our patients with FAIS.
While a number of prior studies in the field of orthopaedic surgery and hip arthroscopic surgery have evaluated predictors of postoperative outcomes, the literature is scarce when describing factors associated with baseline functional scores. In the current study, patients traveling farther distances appeared to have a lower baseline functional status. While no single cause likely exists, we believe that this may be because of a longer pain duration, mental anxiety associated with exhausting nonsurgical options or being referred to nonlocal specialists, and demographics such as a higher BMI, or a lower financial status. However, it should be noted that despite lower preoperative score differences observed between the local and referral groups, there was no statistical difference in postoperative scores or rates of achieving the MCID.
Although the concept of COEs is generally well-accepted and established, little attention has been paid to the associated patient-facing costs of receiving care at a COE. Within orthopaedic surgery, there is increasing emphasis on the provision of care at COEs, with high-volume surgeons and institutions demonstrating improved outcomes and a lower risk for complications. 22 There is an opportunity in future studies to further investigate the cost-benefit for patients in undergoing procedures at COEs. Patients traveling longer distances may incur higher travel costs and be faced with indirect costs from missed work days and lost productivity.
Of note, the analysis demonstrated that adolescents (<22 years of age) fared better than patients aged 22 to 50 and >50 years, which is consistent with prior findings in the literature. Nwachukwu et al 28 evaluated the rates of achieving the MCID in patients aged ≤18 years and demonstrated that they had higher rates of achieving the MCID at 1 year compared with adults in previously published studies. Other studies have demonstrated that this patient group achieves higher PROM scores at 2 years compared with older patients matched by sex. 11
Limitations
There are a number of limitations that should be addressed. First, we did not subdivide patients into rural and urban areas, which may have affected postoperative outcome scores. While a 50-mile radius is roughly the perimeter of the metropolitan area of our institution, including surrounding suburbs, it is not a validated distance, and there are large ranges of AGI both within and outside the radius that may influence access to postoperative care and, indirectly, functional outcomes. Second, while the primary surgeon in this case series performs 500 to 600 surgical procedures annually, there is not yet a defined measure for a COE in hip preservation surgery. Third, the majority of patients within the 50-mile metropolitan radius of our area are likely to have better access to physical therapy and medical treatment than those within 50 miles of other metropolitan areas, so the findings may not be generalizable. Last, the study does not answer the question of whether patients fare better when referred to a large-volume COE in hip preservation located in a metropolitan area versus low-volume centers or those located in rural areas.
Conclusion
When controlling for a number of factors including age, BMI, and AGI, distance to a high-volume hip arthroscopic surgery center did not have an effect on postoperative functional outcome scores or achieving the MCID 2 years after undergoing treatment for FAIS.
Footnotes
Final revision submitted October 4, 2019; accepted October 18, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.U.N. has received educational support from Smith & Nephew and hospitality payments from Stryker, Wright Medical, and Zimmer Biomet. A.J.S. has received research support from Bauerfeind, has received consulting fees from Smith & Nephew, and has stock/stock options in Johnson & Johnson. S.J.N. has received research support from AlloSource, Arthrex, Athletico, DJO, Elite Orthopaedics, Linvatec, MioMed, Smith & Nephew, and Stryker; educational support from Elite Orthopaedics; consulting fees from Ossur and Stryker; and royalties from Ossur and Springer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Rush University Medical Center Institutional Review Board (No. 12022108-IRB01-CR06).