
Abstract
Background:
Treatment of the subscapularis in reverse total shoulder arthroplasty (RTSA) is a controversial topic, with conflicting evidence regarding outcomes after repair.
Purpose/Hypothesis:
The purpose of this study was to report clinical and sonographic outcomes of a through-implant double-row suture technique for subscapularis repair in RTSA and to compare clinical outcomes and range of motion (ROM) between patients with an intact subscapularis tendon repair versus those whose tendon repair was not intact. The authors hypothesized that the novel repair technique would find more than 80% of tendons intact on ultrasound, with significant improvement in clinical outcome scores and ROM. The authors also hypothesized that patients with an intact subscapularis tendon repair would have better clinical outcomes compared with those with a nonintact tendon repair.
Study Design:
Case series; Level of evidence, 4.
Methods:
The study included all patients who underwent RTSA by 1 of 2 surgeons between August 2016 and March 2017 with the through-implant double-row suture technique for subscapularis repair. Subscapularis tendon integrity was assessed postoperatively via ultrasound at minimum 1-year follow-up. American Shoulder and Elbow Surgeons (ASES), Single Assessment Numeric Evaluation (SANE), and pain visual analog scale (VAS) scores were recorded at the final follow-up visit in addition to ROM measures.
Results:
A total of 48 patients (31 males, 17 females; mean age, 68.9 ± 7.4 years; mean follow-up, 13.8 ± 2.1 months) were included. On ultrasound, the subscapularis was intact in 83.3% of patients. Regarding preoperative versus postoperative outcome scores, the ASES score (mean ± SD) significantly improved from 38.3 ± 14.7 to 81.9 ± 13.6, the SANE score significantly improved from 29.8 ± 24.2 to 75.5 ± 21.0, and the VAS pain score significantly improved from 5.9 ± 2.1 to 1.2 ± 1.6 (P < .001 for all). Forward flexion and external rotation significantly improved. No significant difference existed in clinical outcome scores or ROM between patients with intact versus torn subscapularis tendons based on ultrasound.
Conclusion:
Subscapularis repair using a stem-based double-row repair technique during RTSA demonstrated an overall healing rate of 83.3%, as evidenced by ultrasound examination at short-term follow-up. Integrity of subscapularis repair did not affect clinical outcome or ROM.
Keywords
Repair of the subscapularis tendon is a controversial topic in reverse total shoulder arthroplasty (RTSA), as the effects of this repair on clinical outcomes are not well defined. 7,17 Early clinical and biomechanical evidence suggested that repair of the subscapularis tendon reduced the likelihood of postoperative dislocations. 5,9,18 Although subscapularis repair may increase implant stability, recent literature suggests that subscapularis repair may lead to alterations in shoulder biomechanics that are disadvantageous, increasing the workload of the deltoid and posterior rotator cuff and potentially limiting range of motion (ROM) postoperatively. 14 Despite these biomechanical findings, conflicting findings have been reported regarding the effect of subscapularis repair on clinical outcomes, regardless of which type of prosthesis is used. 6,13,17 Furthermore, the majority of studies that have evaluated the effect of subscapularis repair on function after RTSA have not assessed subscapularis tendon integrity after the repair. As such, results may differ depending on the status of the repaired subscapularis tendon.
When the decision to repair the subscapularis is made, very little is known regarding optimal repair technique and outcomes after repair based on repair integrity, as only 2 studies to date in the literature have examined subscapularis repair integrity postoperatively. 7,8 Stem-based repair of the subscapularis has shown promising biomechanical sonographic and clinical results in anatomic total shoulder arthroplasty. 15,16 A similar technique has been developed for reverse shoulder arthroplasty. 15 The technique allows the vector of subscapularis muscle contraction to remain in a more anatomic position, creating dynamic compression of the tendon over the lesser tuberosity of the humerus. This is achieved by using a stem-based double-row repair to the metaphyseal cup and stem. The clinical outcomes and effects of this repair technique on ROM are unknown.
The purpose of this study was to report the clinical and sonographic outcomes of a through-implant double-row suture technique for subscapularis repair in RTSA. A secondary purpose was to compare the clinical outcomes and ROM between patients with an intact subscapularis tendon repair versus those whose tendon repair was not intact. Drawing on our experience, we hypothesized that with the novel repair technique we would find more than 80% of subscapularis tendons intact on ultrasound, with significant improvement in clinical outcome scores and ROM. We also hypothesized that patients with an intact subscapularis tendon repair would have better clinical outcomes compared with those with a nonintact tendon repair.
Methods
All patients with a repairable subscapularis undergoing RTSA by 1 of 2 surgeons (R.G., E.S.L.) were eligible for inclusion in this institutional review board–approved study; both surgeons used the same through-implant double-row suture technique for subscapularis repair. This was a prospective, consecutive series of patients, and all surgical procedures were performed by a fellowship-trained surgeon between August 2016 and March 2017. A total of 48 patients met the inclusion criteria and were enrolled in the study (Figure 1). Patients were excluded if they were undergoing RTSA for prior failed arthroplasty, had a history of prior subscapularis repair, or refused to obtain an ultrasound at minimum 1-year follow-up. A 1-year follow-up period was chosen because most complications, including subscapularis issues, occur early in the postoperative period or at long-term follow-up, and most gains in ROM occur at 6 to 12 months postoperatively; as well, the 1-year follow-up maximized the number of patients eligible for inclusion. 1,21
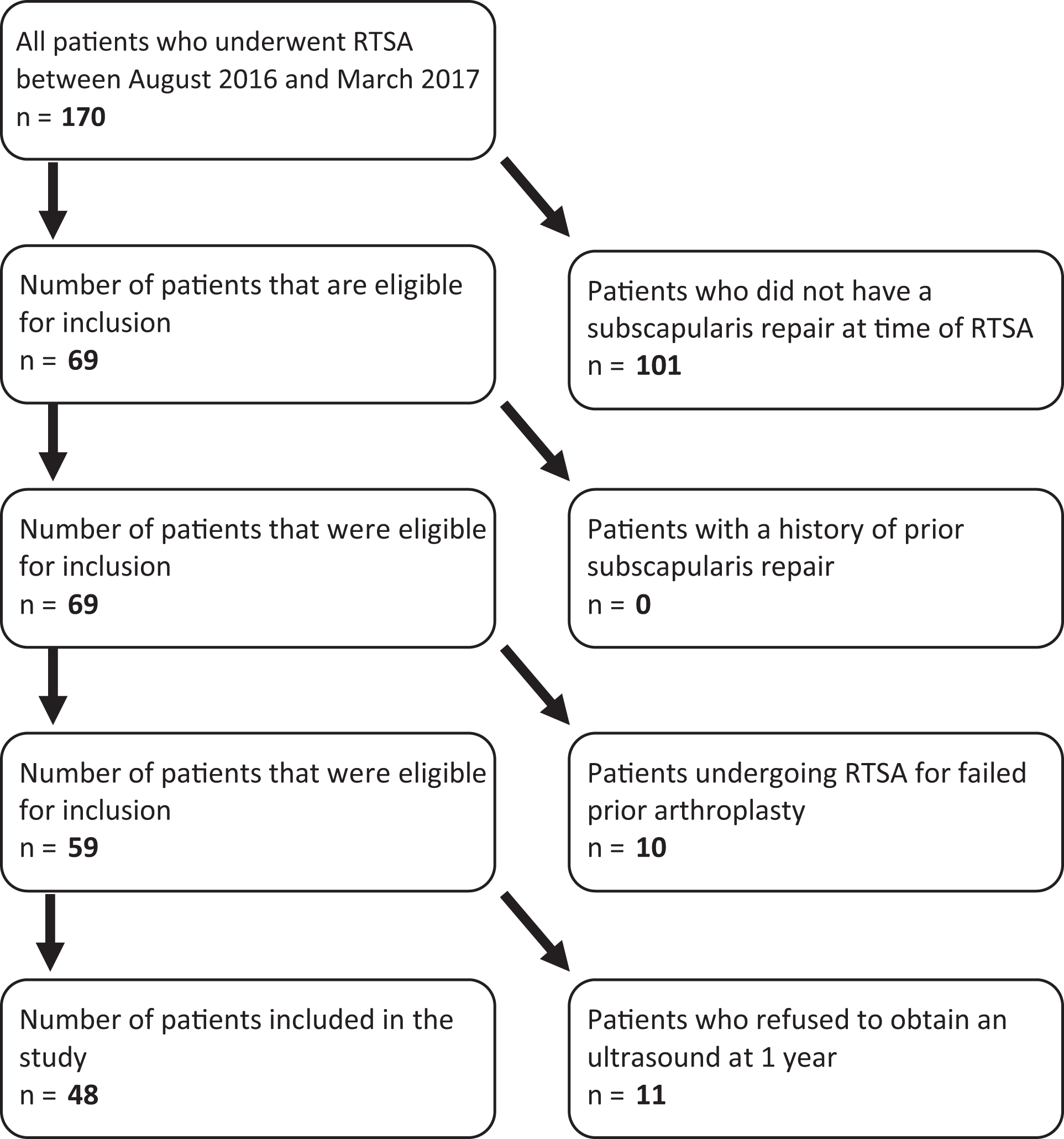
Flowchart of the patients eligible for inclusion. RTSA, reverse total shoulder arthroplasty.
The Univers Reverse Apex Surgical Technique (Arthrex) was used for all patients. This technique involves through-implant transosseous passage of sutures and a double-row repair allowing dynamic compression of the subscapularis tendon over the lesser tuberosity (Figure 2). The implant is designed with fenestrated holes for suture passage allowing for fixation points at the medial and lateral aspect of the lesser tuberosity. The neck shaft angle can be set at 135° or 155°. All patients in this study received an implant with a neck shaft angle of 135°. Intraoperative ROM was assessed after repair, and at least 40° of external rotation at 0° of abduction was present in all patients.

Illustrations demonstrating through-implant technique with double-row repair of subscapularis tendon. (A) High-tensile sutures are placed through the suture cup portion of the humeral stem before the stem is inserted into the humerus. (B) The high-tensile sutures are shuttled through the humerus and through the subscapularis. (C) Final double-row suture bridge construct after the sutures have been tied down.
Postoperative care was uniform throughout the cohort and consisted of a sling for the first 4 weeks. Passive shoulder motion was allowed immediately in the postoperative period, but shoulder extension past neutral and external rotation past 20° at 1 week and past 40° at 2 weeks was avoided to allow the subscapularis to heal. All study participants completed preoperative and postoperative outcome assessments, including the American Shoulder and Elbow Surgeons (ASES) Shoulder Score, the Single Assessment Numeric Evaluation (SANE) index, and a visual analog scale (VAS) for pain. Each clinical outcome score was recorded both preoperatively and at final follow-up. ROM including forward flexion, internal rotation, and external rotation at the side was also recorded preoperatively and at final follow-up. Internal rotation was measured by the spinal level the patient was able to reach on his or her back, and this level was then equated with a numerical value, as has been previously reported. 19
Ultrasound evaluation of the subscapularis tendon repair was performed at 1-year follow-up for each patient, and tendon repair status was divided into 2 categories: intact and not intact. The subscapularis was classified as intact if fibers of the subscapularis tendon remained intact to the repair site. A tendon was classified as not intact if the tendon had pulled away from the repair site and was not in continuity. Ultrasound examinations were performed by the surgeon in the office setting.
Statistical Analysis
Quantitative data were recorded as means and standard deviations, and categorical data were recorded as counts and percentages. Because of the small sample sizes and the possibility that normal tests may not be appropriate, nonparametric procedures were used to test the hypotheses regarding the key outcomes, as follows: The paired-samples Wilcoxon signed-rank test was used to compare preoperative versus postoperative outcome measures when considering all 48 patients, and the Mann-Whitney U test was used to compare the 2 patient groups, those with intact and not intact subscapularis, for the main outcomes. Statistical significance was taken as P < .05. The primary analysis entailed multiple hypothesis testing of outcome data arising from individual patients; however, correction by the Bonferroni method would not have removed significance from any findings. Statistical analysis was completed by use of SPSS 17.0 (IBM Corp).
Results
The participants were 31 male and 17 female patients with a mean ± SD age at the time of surgery of 68.9 ± 7.4 years (range, 47-83 years). There were 27 right and 21 left shoulders. The dominant arm underwent surgery in 58.3% of patients. The mean follow-up period was 13.8 ± 2.1 months (range, 12-18 months). No patient sustained a prosthetic dislocation during follow-up.
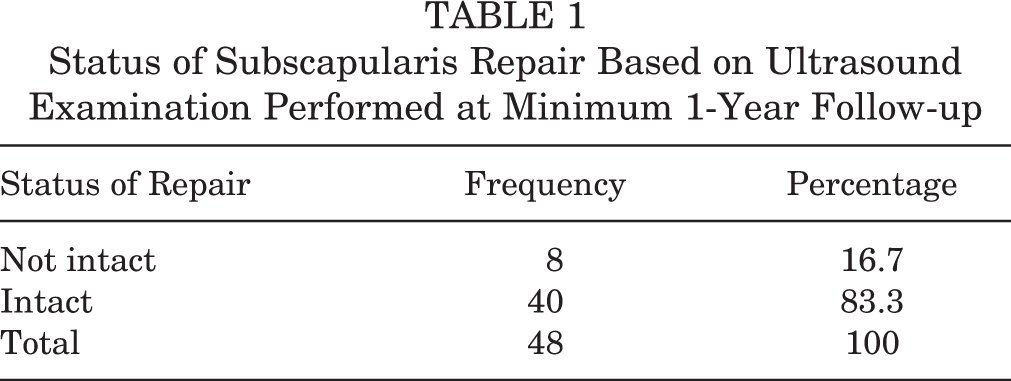
On ultrasound, the subscapularis was intact in 83.3% of patients (Table 1). The subscapularis was noted to be thin intraoperatively in 4 patients and was intact in all 4 patients on follow-up ultrasound. Regarding preoperative versus postoperative outcome scores, the ASES score significantly improved from 38.3 ± 14.7 to 81.9 ± 13.6 (P < .001), the SANE score significantly improved from 29.8 ± 24.2 to 75.5 ± 21.0 (P < .001), and the VAS score significantly improved from 5.9 ± 2.1 to 1.2 ± 1.6 (P < .001) (all P values in this paragraph determined by paired-samples Wilcoxon signed-rank test). Significant improvement was seen in forward flexion, from 101.8° ± 31.3° to 142.2° ± 13.0° (P < .001), and in external rotation at the side, from 25.7° ± 13.1° to 40.1° ± 9.4° (P < .001). Internal rotation did not differ significantly between preoperative and postoperative assessments (P = .091). Tables 2 and 3 demonstrate the mean improvements in clinical outcome scores and ROM from pre- to postoperatively.
Status of Subscapularis Repair Based on Ultrasound Examination Performed at Minimum 1-Year Follow-up
Preoperative to Postoperative Differences in Clinical Outcome Scores After Subscapularis Repair in Reverse Total Shoulder Arthroplasty

Preoperative to Postoperative Differences in Range of Motion After Subscapularis Repair in Reverse Total Shoulder Arthroplasty

a Values are expressed in degrees as mean ± SD.
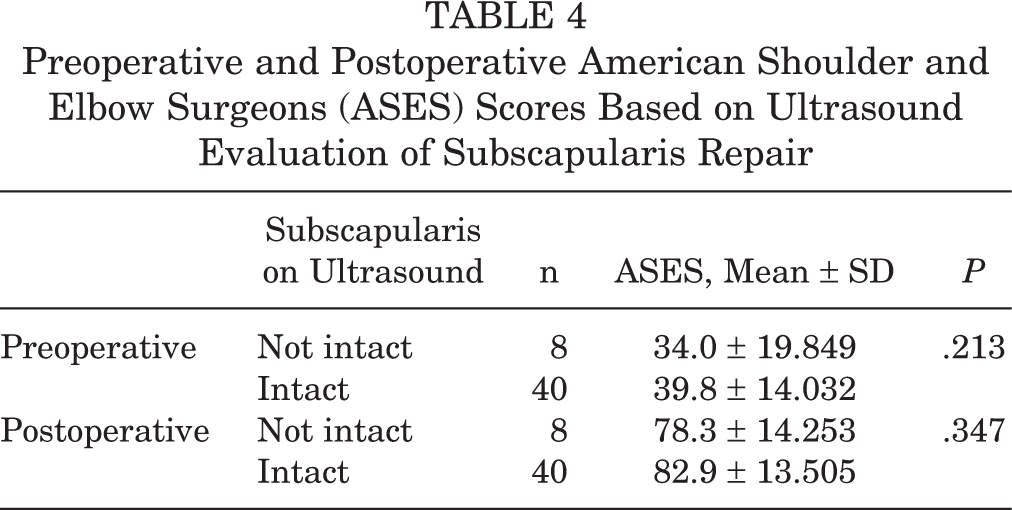
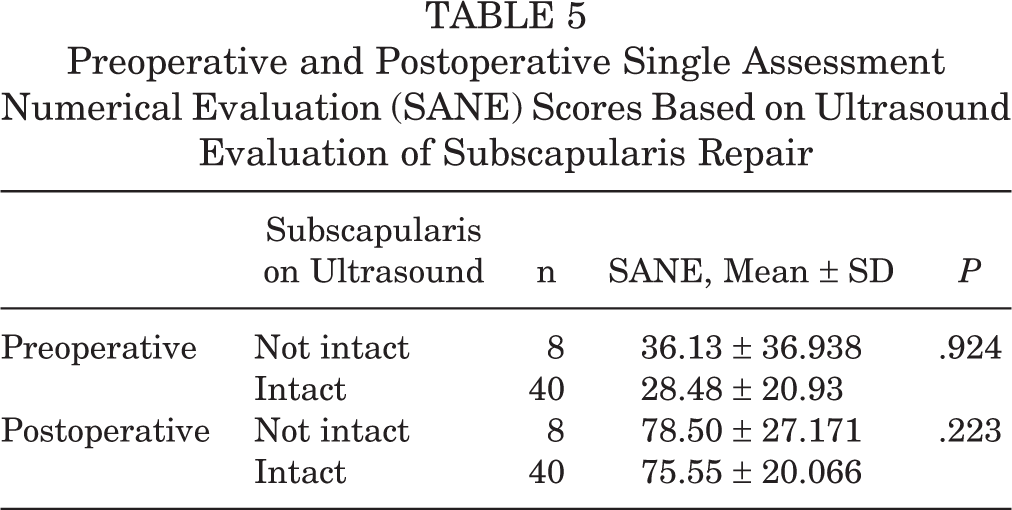
When we compared patients who had an intact subscapularis on ultrasound versus those in whom the subscapularis was not intact, patients with an intact subscapularis had a higher postoperative ASES score (82.9 vs 78.3), but this did not reach statistical significance (P = .347; Mann-Whitney U test) (Table 4). No significant difference existed in SANE or VAS scores between patients with an intact versus nonintact subscapularis repair (Tables 5 and 6). No significant difference in forward flexion, external rotation, or internal rotation existed between patients with an intact subscapularis repair versus a nonintact repair (Tables 7- 9).
Preoperative and Postoperative American Shoulder and Elbow Surgeons (ASES) Scores Based on Ultrasound Evaluation of Subscapularis Repair
Preoperative and Postoperative Single Assessment Numerical Evaluation (SANE) Scores Based on Ultrasound Evaluation of Subscapularis Repair
Preoperative and Postoperative Visual Analog Scale (VAS) Scores Based on Ultrasound Evaluation of Subscapularis Repair

Preoperative and Postoperative Forward Flexion Based on Ultrasound Evaluation of Subscapularis Repair
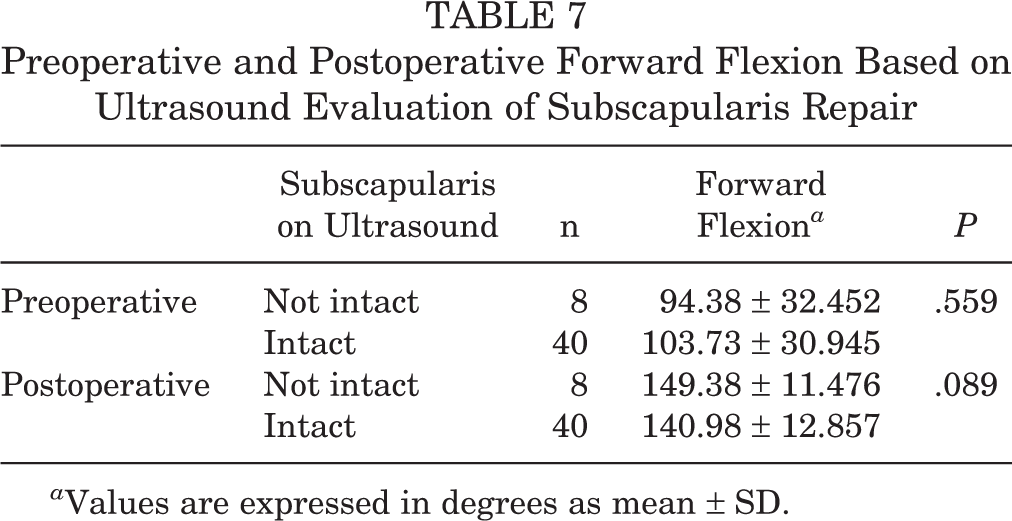
a Values are expressed in degrees as mean ± SD.
Preoperative and Postoperative External Rotation Based on Ultrasound Evaluation of Subscapularis Repair
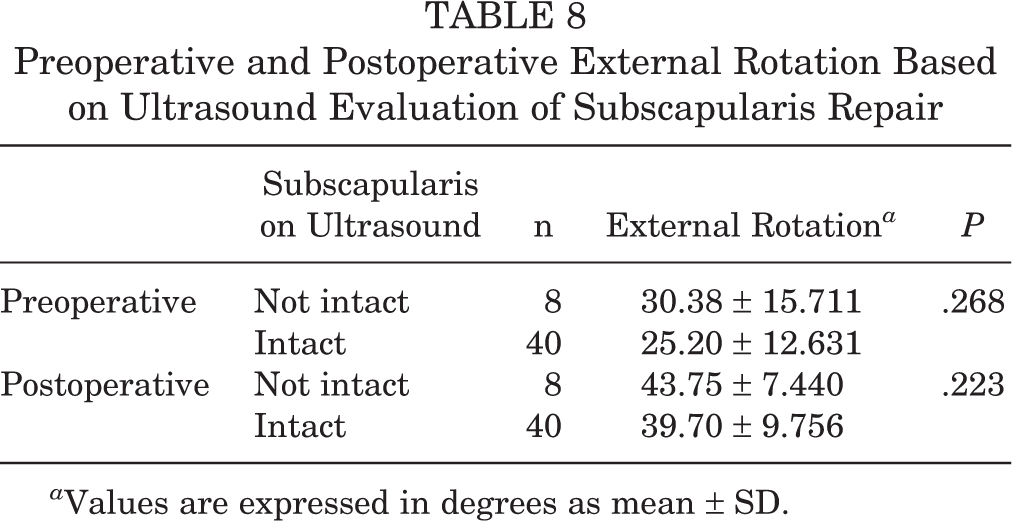
a Values are expressed in degrees as mean ± SD.
Preoperative and Postoperative Internal Rotation Based on Ultrasound Evaluation of Subscapularis Repair

Discussion
RTSA continues to increase in popularity, and several controversies regarding RTSA remain unresolved. One of these involves the ideal way to repair the subscapularis to maximize stability and function while at the same time minimizing deforming forces. Our hypotheses were both confirmed and refuted. The novel repair technique resulted in an intact tendon on ultrasound in more than 80% of patients, with significant improvements in clinical outcome scores, forward flexion, and external rotation after stem-based double-row subscapularis repair. However, internal rotation did not significantly improve from preoperative levels. Furthermore, although the not-intact group was small, no significant difference in clinical outcome scores or ROM existed between patients with an intact versus nonintact subscapularis repair.
Subscapularis repair in RTSA remains a controversial subject. 2,4,10,12 Many subscapularis repair techniques are used in practice, and debate exists as to the optimal technique. 3,16 The ideal technique would provide improvements in stability, strength, and ROM without altering the biomechanics of the joint. A biomechanical study by Lederman et al 16 compared 2 repair techniques in total shoulder arthroplasty with regard to subscapularis tendon displacement during cyclic loading and load to failure. The authors divided 20 matched pairs of cadaveric shoulders into a lesser tuberosity osteotomy and standard suture repair technique group and a through-implant double-row compression technique group, the same technique used in the current study for total shoulder arthroplasty. They then biomechanically tested the repair techniques to determine displacement of the subscapularis footprint, ultimate load to failure, and stiffness. The results demonstrated no difference in early tendon displacement with cyclic loading, similar displacement at 500 cycles, and similar load to failure between the through-implant double-row compression technique and the lesser tuberosity osteotomy technique. Although this indicates that the through-implant double-row repair technique used was biomechanically sound, these findings do not speak to clinical outcomes.
Multiple studies have attempted to elucidate the relationship between subscapularis repair in RTSA and postoperative outcomes and complications. Initial studies advocated for subscapularis repair in all instances of RTSA, pointing to increased instability and risk of dislocation without subscapularis repair. 5,9,11 Oh et al 18 performed a biomechanical study that evaluated subscapularis repair in RTSA and force required to dislocate the prosthesis; those investigators found that subscapularis repair led to increased force required to dislocate the humeral prosthesis anteriorly at multiple neck-shaft angles and multiple humeral rotational angles. Matthewson et al 17 published a 2019 systematic review of more than 1300 patients to examine the effect of subscapularis repair on dislocation rates in RTSA. The authors found significantly lower dislocation rates in patients who had a subscapularis repair compared with those who did not (odds ratio, 0.19; P < .001). No patient in the current study sustained a dislocation after the through-implant double-row subscapularis repair with a 135° implant. Unfortunately, most studies that reported on outcomes after RTSA with and without subscapularis repair did not assess healing of the subscapularis repair; therefore, it is unclear whether an intact subscapularis repair would have significantly improved function and stability compared with no repair or a failed repair. 13
Another potential benefit of a subscapularis repair in RTSA is improved ROM. Wall et al 20 performed a review of 240 RTSAs and found a statistically significant increase in internal rotation for those patients who underwent subscapularis repair compared with those who did not. The current study found a significant increase in forward flexion and external rotation after RTSA with subscapularis repair but no significant change in internal rotation. The improvement in external rotation indicates that the repair was not too tight. Furthermore, ROM did not differ significantly between patients with an intact and a nonintact subscapularis. Internal rotation strength was not measured, so it is possible the repaired subscapularis could provide additional strength, but this is unknown.
The most significant finding in this study was the healing rate of the subscapularis repair. Although many studies have reported results after subscapularis repair in RTSA, the majority of these studies have not reported sonographic healing rates at follow-up. This could be a significant source of bias in these studies, as the integrity of the subscapularis repair may be critical to the patient’s postoperative function. Only 2 studies in the literature 7,8 have examined whether the patients who underwent subscapularis repair at their index repair had an intact tendon during follow-up examination, and both of these studies used a reverse shoulder implant that has an onlay metaphysis and 145° to 155° neck shaft angle. A study by de Boer et al 7 examined integrity of repair with ultrasound in 25 patients who underwent repair after a tenotomy with tendon-tendon and tendon-bone suture fixation and found that 10 of the 25 (40%) were intact, with no difference in clinical outcome scores or ROM between intact and absent subscapularis tendon groups.
More recently, Dedy et al 8 examined 48 shoulders that underwent RTSA with subscapularis repair with transosseous sutures after a lesser tuberosity osteotomy and tenotomy. Ultrasound evaluation of these patients demonstrated that 23% of the subscapularis tendons were not healed at evaluation, 13% were intact, 33% were attenuated, and 31% were severely attenuated. This is higher than the 16.7% of shoulders that were not intact in the current study. Follow-up averaged 19 months (range, 4-132 months) in the study by Dedy et al. Furthermore, those authors found no difference in clinical or functional outcome measures between the healed and nonhealed groups, a finding that the present study corroborated. Hence, although evidence exists that subscapularis repair in RTSA may decrease rates of instability, the repair does not appear to provide a functional benefit, in either clinical outcomes or ROM, regardless of whether the subscapularis heals.
Limitations
Although clinical and sonographic outcomes were recorded, this study has several limitations. This was a prospective cohort of patients from 2 well-trained surgeons who are proficient in shoulder arthroplasty. Hence, the results may not be translatable to surgeons who perform a lower volume of shoulder arthroplasty. Furthermore, no control group was included for comparison of clinical and sonographic outcomes. Although the subscapularis was examined at the time of surgery, no preoperative sonographic assessment of the subscapularis tendon was performed. Finally, the number of patients in which the subscapularis repair was not intact was small. As such, this study may be underpowered to detect a difference in ROM and clinical outcomes between patients with an intact versus nonintact subscapularis.
Conclusion
Subscapularis repair using a stem-based double-row repair technique during RTSA demonstrated an overall healing rate of 83.3%, as evidenced by ultrasound examination at short-term follow-up. Integrity of subscapularis repair did not affect clinical outcomes or ROM.
Footnotes
Final revision submitted November 26, 2019; accepted December 3, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.J.E. has received educational support from Arthrex, Smith & Nephew, and DePuy and hospitality payments from Linvatec and Stryker. M.E.B. has received educational support from Arthrex and Smith & Nephew, grant support from Arthrex, and hospitality payments from Stryker. A.A.R. has received research support from Aesculap/B.Braun, Arthrex, Histogenics, Medipost, NuTech, OrthoSpace, Smith & Nephew, and Zimmer; consulting fees and speaking fees from Arthrex; and royalties from Arthrex, Saunders/Mosby-Elsevier, and SLACK and is a board or committee member for Atreon Orthopaedics. E.S.L. has received research support, consulting fees, speaking fees, and royalties from Arthrex. R.G. has received research support, consulting fees, speaking fees, and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Salus Institutional Review Board (protocol No. 608).