
Abstract
Background:
Anterior cruciate ligament (ACL) reconstruction performed with growth factors and activated platelets has been suggested to accelerate tendon ligamentization, leading to earlier return to daily activities and sports.
Hypotheses:
Platelet-rich fibrin (PRF) will result in improved graft maturation and healing as evaluated by magnetic resonance imaging (MRI) in patients undergoing hamstring ACL reconstruction. Hemostatic and analgesic properties of PRF will lead to less postoperative blood loss and pain.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 44 patients with isolated ACL injuries who underwent arthroscopic all-inside anatomic single-bundle ACL reconstruction with semitendinosus tendon graft were enrolled. Group 1 included 23 patients who had PRF sprayed to the surface of the graft; group 2 included 21 patients for whom no PRF was used. Patients were discharged after 24 hours and examined for hemarthrosis that needed to be aspirated. MRI was performed at the fifth postoperative month. A blinded radiologist evaluated graft maturation according to its signal intensity and the presence of synovial fluid at the tunnel-graft interface.
Results:
PRF-treated grafts demonstrated lower MRI signal intensity and less fluid in the graft-tunnel interface as compared with controls for the entire length of the graft. The mean full-length MRI signal intensities were 9.19 versus 16.59 (P = .047) for groups 1 and 2, respectively. Subgroup analysis of the semitendinosus grafts demonstrated a signal intensity of 11.57 versus 23.98 (P = .044) for the proximal third, 9.53 versus 13.83 (P = .237) for the midbody, and 6.48 versus 11.98 (P = .087) for the distal third. Synovial fluid at the graft-tunnel interface was detected in 1 patient in group 1 (4.3%) and 3 patients in group 2 (14.3%; P < .001). Patients in group 1 had significantly less hemarthrosis that needed to be aspirated (P = .003), while postoperative analgesia requirements were similar in both groups (P = .08). No clinical benefit of PRF could be demonstrated in clinical outcomes.
Conclusion:
Application of PRF led to superior graft integration and maturation in the proximal third of the ACL graft. There was no significant difference in MRI signal intensity in the midbody or distal tibial graft. Application of PRF also resulted in significantly lower rates of postoperative hemarthrosis that needed to be aspirated.
Keywords
Anterior cruciate ligament (ACL) reconstruction with autologous hamstring tendons is a proven method to restore the normal biomechanics and stability of the knee. 13,33 The primary goal of ACL reconstruction is to create a stable knee with good biomechanical properties. A successful outcome depends on the healing quality of the reconstructed graft. 15 The 3 phases of the autograft maturation process are inflammation, proliferation (reparation), and remodeling. 21,24 Growth factors—including platelet-derived growth factor (PDGF), transforming growth factor beta (TGF-ß), insulin-like growth factor, fibroblast growth factor, and vascular endothelial growth factor (VEGF)—have been reported to be present in every step of the healing process, with the ability to activate the membrane receptors in integrins while enhancing the production of components of collagen matrices. 23,34
Activated platelets release about 30 bioactive molecules, which are composed mainly of growth factors and cytokines that promote tissue regeneration and soft tissue maturation by stimulating mesenchymal cells and macrophages with osteoblasts. 11,23 Activated platelets with the aforementioned capabilities are able to provide bone regeneration and soft tissue maturation. 29 There has been increasing popularity in the usage of growth factors and activated platelets at ACL reconstruction, with the possible hypothesis to accelerate tendon ligamentization, leading to earlier return to daily activities and sports. 11,16 Platelet-rich fibrin (PRF) produced by the Vivostat system (Vivostat A/S) concentrates the platelets to approximately 7 times the platelet level of the donor’s blood. This high number of platelets is combined with a concentration of fibrin of approximately 7- to 10-times baseline value. PRF has been reported to promote tissue regeneration by utilizing the aforementioned growth factors and reducing the amount of matrix metalloproteinase 9 (MMP-9), which is a potent agent that delays wound healing and a potential inhibitor of ligamentization. 1,6 PRF also increases psoriasin gene (S100 calcium binding protein A7) expression in vitro, which is responsible for angiogenesis, wound healing, and immunomodulation. 5
Platelet-rich plasma and other growth factors, including VEGF and PDGF, have been used to modulate pain and provide analgesia with enhancement of the graft healing and ligamentization of ACL reconstruction. 12,22 Although PRF has been reported to be an effective adjunct in the treatment of osteochondral lesions of the talus, 8,9,14 no study has been performed on the effect on ACL graft maturation. The aim of this study was to evaluate the theoretical positive effects of PRF with regard to graft maturation and healing, with its hemostatic effect on postoperative hemarthrosis and analgesic effect on early postoperative pain in patients undergoing ACL reconstruction with autologous semitendinosus tendon graft. Our first hypothesis was that PRF would result in improved graft maturation and healing, as evaluated by magnetic resonance imaging (MRI), in patients undergoing hamstring ACL reconstruction. Our second hypothesis was that the hemostatic and analgesic properties of PRF would lead to less postoperative blood loss and pain.
Methods
Institutional review board approval for the study was obtained, and all participants provided informed consent. Patients with acute total isolated ACL rupture were eligible to be enrolled in the study. The exclusion criteria were a history of rheumatologic, metabolic, or malignant disorder; any previous ACL or other surgical procedure in the same joint; accompanying posterior cruciate ligament (PCL) and/or posterolateral corner injuries; and meniscal injury requiring repair or excision.
A total of 44 patients were enrolled in the study. All patients underwent surgery within 3 weeks of their initial injury (mean, 12.4 days; range, 4-21) and after receiving preoperative rehabilitation. Patients were deemed ready for surgery when they had full active extension and 120° to 140° of painless flexion without an apparent effusion. All patients underwent anatomic (tunnel locations in the center of the footprint of the torn ligament) single-bundle, all-inside ACL reconstruction with a single autologous quadrupled semitendinosus tendon graft with the same tunnel position and diameter by 1 senior surgeon (T.B.). 7,19 Femoral and tibial fixations were performed by using 2 TightRopes (Arthrex). Randomization of the patients was performed using dedicated software.
Group 1 included 23 patients (5 females, 18 males) who had PRF application using the Vivostat system during surgery. Group 2 was the control group and included 21 patients (4 females, 17 males) who did not receive any PRF application (Table 1). In group 1, blood (120 mL) was drawn in the premedication room to prepare the PRF before the induction of anesthesia and antibiotic prophylaxis. The Vivostat device is a closed system that consists of a preparation unit and a processor unit. The blood is placed in this automated device, and after approximately 30 minutes, an autologous PRF solution is ready to use. The PRF solution polymerizes immediately upon application by a simple pH change at the tip of the spray pen. At the end of the ACL reconstruction, knees in group 1 were emptied of arthroscopic fluid, and PRF (5-6 mL) was sprayed by a dedicated application device (Figure 1) in the Vivostat system over the graft body, inside the femoral tunnel, at both tendon-tunnel interfaces, and to areas where bleeding was expected (eg, posterior to the PCL, intercondylar notch) as well as any bleeding site observed in the setting of dry arthroscopy (Figure 2).

Platelet-rich fibrin delivery application device.
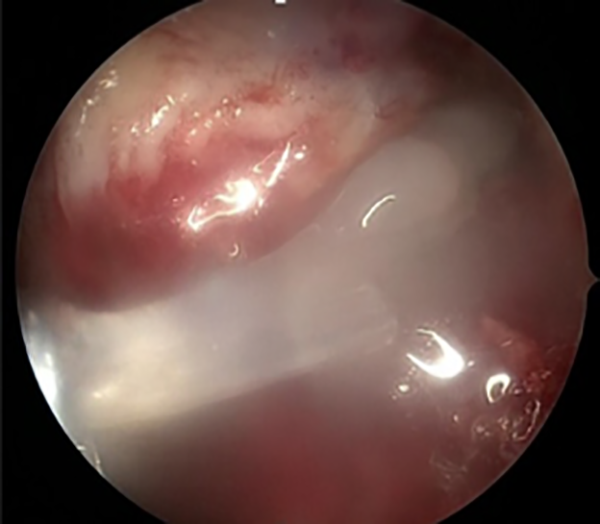
Application of platelet-rich fibrin on the surface of the graft in the setting of dry arthroscopy.
Patient Demographic Data a
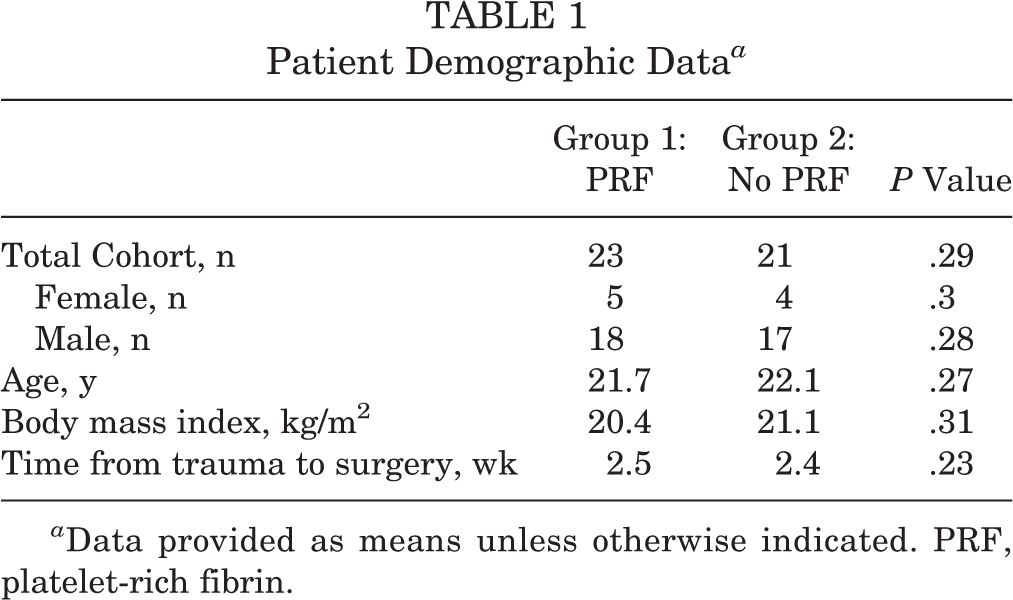
a Data provided as means unless otherwise indicated. PRF, platelet-rich fibrin.
All other aspects of surgery and rehabilitation were similar in groups 1 and 2. No tourniquet was used nor were any drains placed. No external braces were used postoperatively. Partial weightbearing as tolerated with 2 Canadian crutches, full extension, and a maximum 90° of flexion were allowed on the same day as surgery. All patients received patient-controlled analgesia (PCA) pumps after surgery. Our PCA (Abbott Laboratories) protocol was composed of droperidol (5 mg) and morphine (1 mg/mL) in 0.9% normal saline (100 mL). Initially, the machine was programmed to deliver a continuous dose of 0.015 mL/kg/h and a bolus dose of 0.02 mL/kg/h, which was then adjusted by PCA nurses to maintain patient satisfaction and an acceptable pain level. Patients were given nonsteroidal anti-inflammatory drugs (acemetacin, 60 mg) twice a day for 10 days. None of the patients were professional athletes, and the groups were comparable with regard to their demographic data in terms of number, age, and sex (Table 1).
All patients were observed in the hospital on the night of the surgical procedure and evaluated the next day. Patients were discharged after 24 hours and examined for any hemarthrosis requiring aspiration during discharge as well as at the seventh postoperative day. Hemarthrosis requiring aspiration was defined as significant hemarthrosis restricting knee range of motion and having a positive balloting patella during the physical examination. The amount of intravenous PCA drug used was noted for all patients. All patients had the same postoperative rehabilitation protocol in 1 center. Deep venous thrombosis prophylaxis was performed with low–molecular weight heparin subcutaneously for 10 days. All patients had an MRI of the involved knee at the end of postoperative fifth month, in the same radiology center with the same device (GE Explorer; GE Healthcare). Evaluation of the graft was performed at 5 months, as previous studies have shown that it takes 4 to 6 months for ACL grafts to complete the proliferation phase and begin the ligamentization phase, where the graft’s structural and biomechanical characteristics become similar to those of an intact ACL. 15 A blinded radiologist (U.T.) evaluated the graft’s maturation according to its signal intensity and the presence of synovial fluid at the tunnel-graft interface on the MRI scans. Signal intensity measurements were performed for the patellar tendon (PT), quadriceps tendon (QT), PCL, and reconstructed graft’s proximal and distal thirds and midbody. Signal-noise ratio was used for the expression of measurements. On the sagittal (proton density, T1) image that best showed the ACL graft, 1 region of interest (ROI) was taken as the pitch-black region (as the noise) on the images, while other ROIs were defined as 3 points on ACL grafts (proximal, midbody, distal) and 1 point in the midportion of the PCL, PT, and QT (Figure 3). Signal-noise ratio was defined as the signal of the ROI divided by the noise of the pitch-black region.
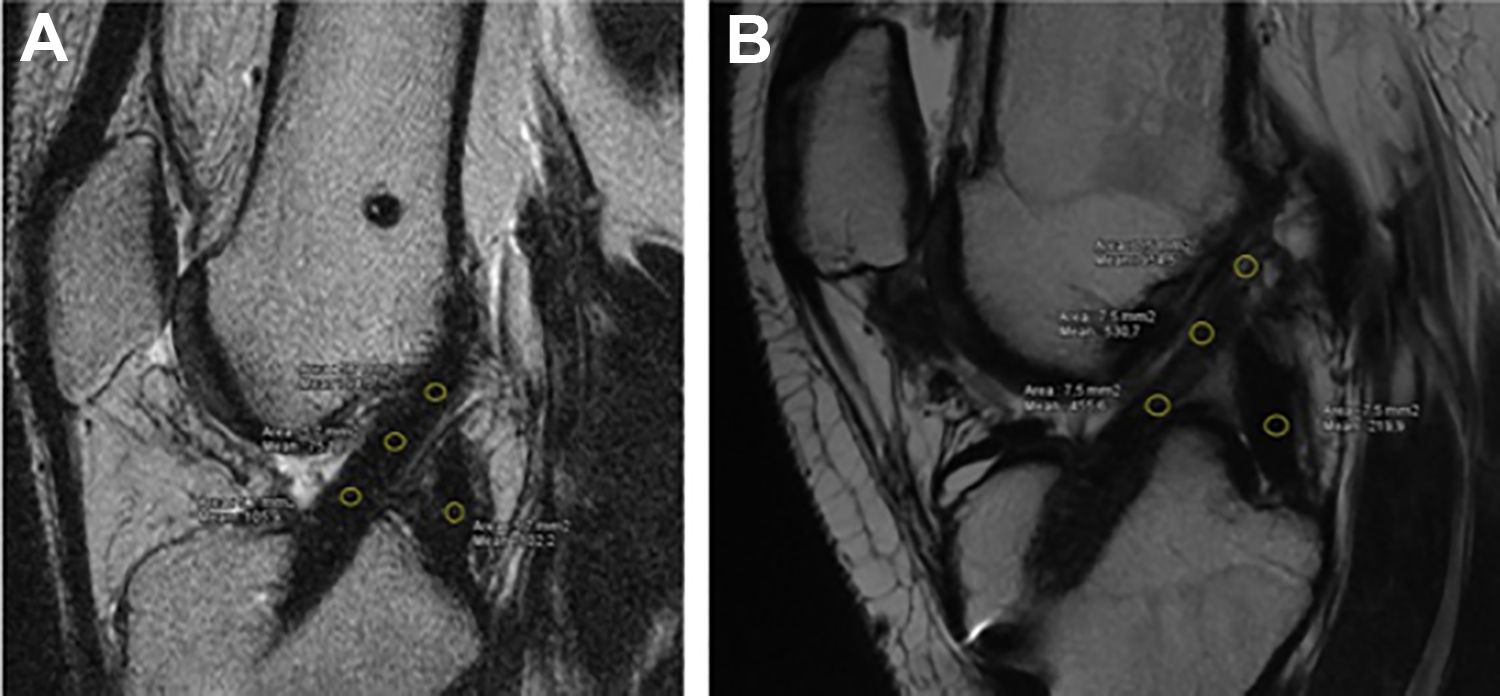
Evaluation of the graft’s maturation according to signal intensity and the presence of synovial fluid at the tunnel-graft interface on the magnetic resonance image taken at the fifth postoperative month. (A) Patient from group 1. (B) Patient from group 2.
Patients were recalled for clinical examination at the end of the first postoperative year. Knee range of motion, Tegner-Lysholm, and International Knee Documentation Committee (IKDC) scores were calculated and compared.
For the statistical analysis, SPSS software (Version 22.0; IBM) was used. For quantitative variables between groups, the Student t test was used. Data were expressed as mean ± SD. The chi-square test and Fisher exact test were used for the analysis of categorical variables where appropriate. A P value <.05 was considered statistically significant.
Results
No patients were lost to follow-up for the clinical examination at 12 months, and all patients had an MRI examination at the end of 5 months. Mean operating room time was 69 minutes in the PRF group and 62 minutes in the non-PRF group (P = .3). In group 1, one patient had a hemarthrosis that needed to be aspirated at 24 hours following surgery and another at the end of the first postoperative week (total 2 patients, 8.7%). In group 2, four patients needed an aspiration at 24 hours and 4 more at the end of the first postoperative week (total 8 patients, 38%). The mean amount of fluid that was aspirated was approximately 40 mL. This lower rate of aspiration in the PRF group had high statistical significance (P = .003).
No significant differences in postoperative analgesia requirements were detected between the study and control groups. PCA durations were 10 hours for group 1 and 11 hours for group 2 (P = .08). The total volume of narcotic drugs was also similar: 156.7 mL for group 1 and 154.2 mL for group 2 (P = .27).
The reference points used in signal intensity measurements (ie, PT, QT, and PCL) were comparable for groups 1 and 2 (Table 2). PRF-treated grafts (group 1) demonstrated lower MRI signal intensity when compared with controls (group 2) for the entire length of the graft (Table 3). This difference reached statistical significance only for the mean values of the entire graft and the proximal third, while no statistical difference could be observed for values in the midbody and distal third. No adverse effects were seen on MRI in the PRF group.
Signal Intensities of Reference Points a

a PCL, posterior cruciate ligament; PRF, platelet-rich fibrin; PT, patellar tendon; QT, quadriceps tendon.
b Significance set at P < .05.
Radiographic Results: Semitendinosus Graft a

a PRF, platelet-rich fibrin.
b Boldface values indicate statistical significance (P < .05).
Synovial fluid between the graft and the bone tunnel was seen in 1 patient in group 1 (4.3%) and 3 patients in group 2 (14.3%; P < .001). This difference was highly significant. No statistically significant difference was detected with regard to clinical outcome measures calculated at the end of the first postoperative year. For group 1 versus group 2, the mean knee range of motion was 129° versus 126° (P = .27), the mean IKDC scores were 87.1 versus 86.8 (P = .3), and the mean Tegner-Lysholm scores were 96.1 versus 95 (P = .32), respectively.
Discussion
The most important finding of this study was that PRF treatment of ACL grafts during anatomic single-bundle ACL reconstruction resulted in better MRI characteristics and earlier maturity of the proximal third of the graft as compared with controls. This, however, did not lead to better clinical outcomes, with both groups achieving similar function and stability at 1 year.
ACL reconstruction with the semitendinosus graft has been reported to be safe and reliable, resulting in excellent knee stability if performed with the correct surgical technique and if solid bone-graft integration occurs. 10,25 The biomechanical properties and stability of the graft are closely related to the stage of ligamentization, with an initial decrease in strength attributed to cell death, followed by an increase in strength with cell proliferation and remodeling. The exact duration of this process is unclear. Most of the ligamentization occurs at 4 to 6 months after the surgery; however, structural changes have been reported to occur years after the reconstruction. 10,25,26 Integration and ligamentization are considered to be a process in which production of type I collagen by fibroblasts secures the integration, and the appearance of Sharpey fibers strengthens the ligamentization and provides a safe integration of the graft within the bone tunnels. Finally, the graft’s biomechanical and structural properties resemble that of an intact ACL. 15,31,34 –36
A recent concept is to biologically augment the integration process of the ACL graft with platelet-derived growth factors, including TGF-ß, PDGF, and VEGF. These growth factors have been shown to exert positive effects on soft tissue proliferation, neovascularization, healing, and regeneration. 3,4,10,17,27,30
Nevertheless, there are a limited number of studies in the literature with regard to the use of growth factors for ACL reconstruction. Most studies focused on the effect of growth factors on the ligamentization process of the grafts. In a rabbit model, Anderson et al 2 demonstrated the augmenting properties of osteoinductive growth factors on tendon healing, while Yoshikawa et al 36 underlined that the addition of exogenous VEGF to semitendinosus grafts during ACL reconstruction in sheep might promote angiogenesis of the ACL graft and decrease the stiffness of the grafted tendon.
Evaluation of the maturation, integration, and ligamentization of the grafts used for ACL reconstruction is another topic of debate. Uchio et al 31 conducted an MRI study of 64 patients 2 years after ACL reconstruction, with second-look arthroscopies and histopathological examination. They reported that high-intensity signal on MRI might predict late integration of the grafts in the bone tunnels, leading to postreconstruction instability. In contrast, Li et al, 18 in their study of 38 patients, concluded that MRI-based graft maturity was unable to yield accurate data to predict clinical and functional outcomes, and they underlined that it should not be used as an objective test to determine the appropriate time to return to sports activities after ACL reconstruction.
Studies on MRI evaluation of the ligamentization and integration process of the ACL grafts augmented with platelet-rich plasma or autologous platelet concentrate (APC) have reported significant differences between treatment and control groups. Figueroa et al 11 reported better graft integration in the APC group (97.4% vs 94.7%) as compared with controls at 6 months, based on the evaluation of signal pattern on MRI and the presence of synovial fluid at the graft-tunnel interface. In addition, they found a higher proportion of patients with hypointense grafts in the APC-treated group versus controls (63.2% vs 42.1%). Although no statistically significant difference with regard to graft maturation and ligamentization could be demonstrated, the group with APC had superior clinical results. Orrego et al 24 conducted a similar MRI study with 4 groups (control, APC, bone plug, APC + bone plug) where the grafts were evaluated at 3 and 6 months postoperatively. They found no statistically significant difference with regard to graft maturation and tunnel widening, although the group treated with platelet concentrate had better results. The results of these 2 studies were noted to support each other.
However, there are several studies reporting a significant benefit of growth factors on the ligamentization and integration of semitendinosus grafts. Ventura et al 32 augmented 10 ACL reconstructions using semitendinosus gracilis graft by adding intratunnel APC, and they compared these with 10 controls at 6 months using a computed tomography scan. The group with APC augmentation demonstrated significantly faster ligamentization as compared with controls. In a prospective study where intratunnel APC was applied to 50 knees, Radice et al 25 obtained serial MRI scans every 3 months from the third to ninth postoperative month. They noted that APC had significant enhancement properties with regard to graft remodeling and reduced the time until normal maturation by 49.4%.
Sanchez et al 26 evaluated the morphology of ACL grafts treated with platelet-rich plasma preparation rich in growth factors (PRGF) with second-look arthroscopies and reported excellent outcomes in 57.1% of the PRGF group, while only 33.3% of the controls had similar results. PRGF-treated grafts had a significantly better maturity index, and histologically evident, newly formed connective tissue enveloping the graft was present in 77.3%, as compared with 40% of controls.
PRF utilized by the Vivostat system has been shown to cause a sustained release and protection against degradation of endogenous fibrogenic factors, facilitating enhanced wound healing. 20 A study conducted by Agren et al 1 demonstrated that PRF applied by the Vivostat system was able to reduce MMP-9 by 139-fold while concentrating the presence of a variety of growth factors that enhance tissue regeneration by 1.6- to 75-fold. It has also been shown that the nonactivated platelets prepared and applied by Vivostat PRF stimulated wound healing far more effectively than activated platelets utilized by most other platelet-rich plasma products by enhancing fibroblast differentiation and stimulating the contractile function. 28
Vivostat was shown to be helpful in the treatment of talar osteochondral lesions by Giannini et al 14 and Buda et al 9 and to be effective in the treatment of osteochondral lesions in mild hemophilic ankle arthropathy by delaying the ankle arthrodesis. 8
This is the first study on the application of autologous PRF produced by the Vivostat device to ACL autografts. We used dry arthroscopy to be sure that PRF stays on the surface of the graft after being sprayed with the dedicated applicator of the Vivostat system. We performed MRI scans to evaluate the ligamentization and integration of the semitendinosus grafts. Our results confirmed that application of PRF was able to yield superior results as compared with controls at the proximal portion inside the femoral tunnel, but there was no significant difference in MRI signal in the midportion or distal aspect of the grafts. It was also shown that the group with PRF had significantly less synovial fluid at the tunnel-graft interface. These results indicate that PRF applied by the Vivostat system may be able to yield better ligamentization and integration of the ACL grafts. We believe that the fibrin matrix is able to maintain the platelets longer in position, making it possible to deliver the maximum amount of growth factors to the graft surface.
The hemostatic effect of PRF was another point to be underlined. Buda et al 8 showed that the clotting factors contained in the autologous PRF might regulate and control the intra- and postoperative bleeding. We demonstrated that PRF application to the graft and bleeding points during dry arthroscopy resulted in significantly less hemarthrosis that needed to be aspirated at the end of the first 24 hours and the first postoperative week.
It should be noted that to evaluate whether the PRF also had a hemostatic effect, we aspirated the effusion/hematoma in patients with ++ or +++ balloting patella, knowing that it would likely resolve in 2 to 3 weeks according to the literature and our previous clinical experience. No increase in analgesic requirements were observed after PRF application.
While this study showed significantly superior MRI findings in the context of ligamentization and maturation in the proximal part of the reconstructed ACL grafts treated with PRF, no significant difference in clinical outcome parameters versus controls could be observed. In brief, better ligamentization did not lead to superior clinical outcomes or better knee stability. However, PRF augmentation can result in earlier return to sport or activities of daily living if earlier maturation of the graft can be achieved.
The main strength of this study was that it was undertaken comparatively, where the groups were randomized by computer and the radiographic evaluation was performed by a blinded senior musculoskeletal radiologist. The main weaknesses were as follows: (1) few patients were retrospectively evaluated, (2) ligamentization and integration of the grafts were evaluated by T2 mapping MRI at only a single time point, (3) quantification and typing of growth factors and quantification of hematoma size were not performed, and (4) no histological analysis was performed because it was not found to be ethical in the study design. Additionally, we evaluated signal intensity of the graft at only 1 time point (5 months), and it is not known whether and/or when these differences will resolve over time.
Conclusion
This study concludes that the application of autologous PRF during ACL reconstruction in the setting of dry arthroscopy leads to better MRI maturation characteristics in the proximal third of the graft as compared with controls at 5 months. This effect is significantly higher in the proximal third of the graft. Better maturation in MRI does not lead to better clinical outcomes or a reduction in analgesic usage. The hemostatic effect of PRF is beneficial, resulting in less postoperative hematoma.
Footnotes
Final revision submitted September 25, 2019; accepted September 28, 2019.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Halic University Institutional Review Board.