
Abstract
Background:
Posterior shoulder instability is associated with nonspecific symptoms, including pain, subluxation, and functional impairment, which complicate its diagnosis and management. Owing to the rarity of the condition, there are no present decision tools for its diagnosis and treatment.
Purpose:
To investigate demographic, lesional, and surgical factors that influence functional outcomes in patients treated for posterior shoulder instability.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
We analyzed the clinical and radiographic records of 150 patients treated surgically for isolated posterior shoulder instability at 10 centers between 2000 and 2015, of which 144 were eligible for inclusion: 114 men (79%) and 30 women (21%) (mean ± SD age, 28.7 ± 9.6 years). The mean time between onset of symptoms and surgery was 66 ± 75 months. Shoulder instability was of traumatic origin in 115 patients (80%). The primary treatment was bone-block procedures for 65 patients (45%), posterior Bankart repair for 67 (47%), and capsular plication for 12 (8%). Patients were assessed with the Constant and Walch-Duplay scores at a mean follow-up of 51 ± 32 months (range, 12-159 months). Uni- and multivariable regression analyses were performed to determine associations between clinical scores and sex, age, traumatic origin, type of lesion, type of procedure, and follow-up.
Results:
At final follow-up, subluxations or dislocations recurred in 24 patients (17%). The overall Constant score was 86.2 ± 14.5, with a pain component of 12.6 ± 3.5. The Walch-Duplay score was 79.8 ± 24.2. Multivariable regressions revealed that the presence of a glenoid cartilage lesion was the only factor associated with worse Constant score (beta = –10; P = .013) and Walch-Duplay score (beta = –16.7; P = .024) across all subcomponents.
Conclusion:
The only factor that jeopardized functional outcomes of posterior instability surgery was the presence of glenoid cartilage lesions. Knowing that shoulders with glenoid cartilage lesions are at greater risk of residual pain or instability could help manage patient expectation and justify faster intervention before lesions deteriorate.
Posterior shoulder instability is a rare injury, accounting for 2% to 10% of all shoulder instabilities, 3,5,6,15,21,24,34,39 and is often associated with bidirectional or multidirectional instability. 42,45,46 Its causes are multifactorial, including bony and soft tissue abnormalities, repetitive injuries, and traumatic dislocations. 45
Posterior shoulder instability, especially in patients with atraumatic lesions, engenders multiple nonspecific symptoms, including pain, subluxation, and functional impairment, which complicate its diagnosis and management. 4,13,38,39,45 Conservative treatment of posterior shoulder instability has low success rates, 12,23,37,38,45 especially in patients with traumatic lesions. 32,39 When conservative treatment fails, surgery is recommended to grant long-term stability, prevent pain, and enable return to previous activity levels. 10,12,13,26,33,38 Glenoid fractures and bone loss are frequently treated by bone-block procedures, while labral tears are commonly treated by the Bankart procedure. 1,6,9,25,26,28 The choice of surgical technique is critical and requires meticulous analysis of numerous preoperative imaging and clinical findings.
Unlike that for anterior instability, 2 there is no present decision tool for the diagnosis and treatment of posterior shoulder instability, probably because of the relative rarity of the condition. The purpose of the present study was therefore to investigate the demographic, lesional, and surgical factors that influence functional outcomes in patients undergoing surgery for posterior shoulder instability. The hypothesis was that functional outcomes would be better for patients treated with bone-block procedures.
Methods
We reviewed the clinical and radiographic records of 150 patients who underwent surgery for posterior shoulder instability at 10 centers between January 2000 and December 2015. The inclusion criteria were a minimum follow-up of 1 year and the presence of at least 1 of the following preoperative lesions: posterior glenoid erosion, posterior glenoid fracture, reverse Hill-Sachs, or posterior labral lesion. Six patients had none of the aforementioned lesions and were therefore excluded, leaving 144 eligible patients. The cohort comprised 114 men (79%) and 30 women (21%) aged 28.7 ± 9.6 years (mean ± SD; range, 13-58 years; median, 27 years) at index surgery. Shoulder instability was of traumatic origin in 115 patients (80%). The institutional review board of the ethical committee of the Hôpital Privé Jean Mermoz and the Centre Orthopédique Santy approved the study, which was conducted in accordance with the rules and regulations of ethics and privacy of the national regulatory body.
Preoperative Assessment
A standardized form was used across all centers to collect the following information: patient age, sex, dominant arm, and cause of instability (traumatic vs atraumatic). All patients were evaluated preoperatively with radiographs and either computed tomography arthrography or magnetic resonance arthrography to evaluate bony and/or soft tissue lesions. Cartilage lesions were defined as alterations of the cartilage surface without bony defects, corresponding to grades 1 to 4 of the classification of the International Cartilage Repair Society. 7 A glenoid erosion was defined as a bony erosion of the posteroinferior aspect of the glenoid without bone fragments. A labral lesion was defined radiographically as a posteroinferior tear of the labrum and clinically confirmed by the Kim test. 22 Of the 144 patients, 111 (77%) had posterior labral lesions, 63 (44%) had posterior glenoid erosions, 37 (26%) had reverse Hill-Sachs lesions, 20 (14%) had cartilage lesions at the posterior part of the glenoid, 14 (10%) had glenoid fractures, and 10 (7%) had cartilage lesions at the humeral head.
Surgical Technique
All preoperative lesions were confirmed intraoperatively. Open bone-block procedures, as described by Levigne et al, 27 were the primary treatment for shoulders that presented bony defects at the posterior aspect of the glenoid and were performed in 65 shoulders (45%) without preoperative arthroscopic evaluation. The bone blocks were harvested from the acromion for 9 shoulders (13.8%) and the iliac crest for 56 shoulders (86.2%). Arthroscopic or open posterior labral repair (Bankart) was the primary treatment for shoulders that presented posterior labrum tears and was performed in 67 shoulders (47%). Arthroscopic or open capsular plication was performed in isolation for 12 shoulders (8%). Bankart repairs and capsular plications were performed with a mean 3 suture anchors (range, 1-7), which were bioresorbable in 85% of cases. Of the 37 shoulders with reverse Hill-Sachs lesions, adjuvant remplissage with the subscapularis tendon was necessary in 6 shoulders (16.2%).
Postoperative Rehabilitation
Patients were immobilized in neutral rotation for 6 weeks and started range of motion exercises at 3 weeks. Bone-block osteointegration was verified radiographically at 3 months, and if confirmed, bench pressing and return to sport were allowed.
Postoperative Assessment
Patients were examined postoperatively at a mean follow-up of 51 ± 32 months (median, 46 months; range, 12-159 months) for routine clinical assessment with the Constant score 11 and Walch-Duplay score. 19 Recurrence of instability was defined as a manifestation of 1 or more episodes of subluxation and/or dislocation during the follow-up period.
Statistical Analyses
Descriptive analyses were performed for continuous and categorical variables. Shapiro-Wilk tests were used to assess the normality of distributions. Univariable linear regressions were performed to determine associations between 3 outcomes (overall Constant score, pain component of the Constant score, and Walch-Duplay score) and 14 independent variables (age, time from symptoms to surgery, follow-up, sex, arm dominance, traumatic origin, glenoid erosion, glenoid fracture, reverse Hill-Sachs, labral lesion, glenoid cartilage lesion, bone-block procedure, Bankart procedure, capsular plication). Considering the recommendations of Harrell, 20 who advised a minimum of 10 participants per variable for adequate power with any multivariable linear regression, we selected the 10 most pertinent variables for the latter, based on clinical experience. Statistical analyses were performed with R v 3.3.3 (R Foundation for Statistical Computing). P values <.05 were considered statistically significant.
Results
The overall Constant score was 86.2 ± 14.5 (range, 29-100; median, 89.2) with a pain component of 12.6 ± 3.5 (range, 0-15; median, 15). The Walch-Duplay score was 79.8 ± 24.2 (range, 0-100; median, 90). A total of 24 patients (17%) experienced recurrence of instability with 1 or more episodes of subluxation (15.3%) and/or dislocation (4.2%) during their follow-up period.
Univariable regressions revealed that the overall Constant score was significantly associated with age (beta = –0.3; P = .010), glenoid cartilage lesion (beta = –13.7; P < .001), and capsular plication (beta = 10.1; P = .011) (Table 1). Multivariable regressions revealed that the overall Constant score was associated only with glenoid cartilage lesion (beta = –10; P = .013). Univariable regressions revealed that Constant score pain was significantly associated with none of the variables, but multivariable regressions revealed it to be significantly associated with glenoid cartilage lesion (Table 2).
Linear Regression Analysis of Postoperative Overall Constant Score (0-100) Associated With Patient Characteristics a
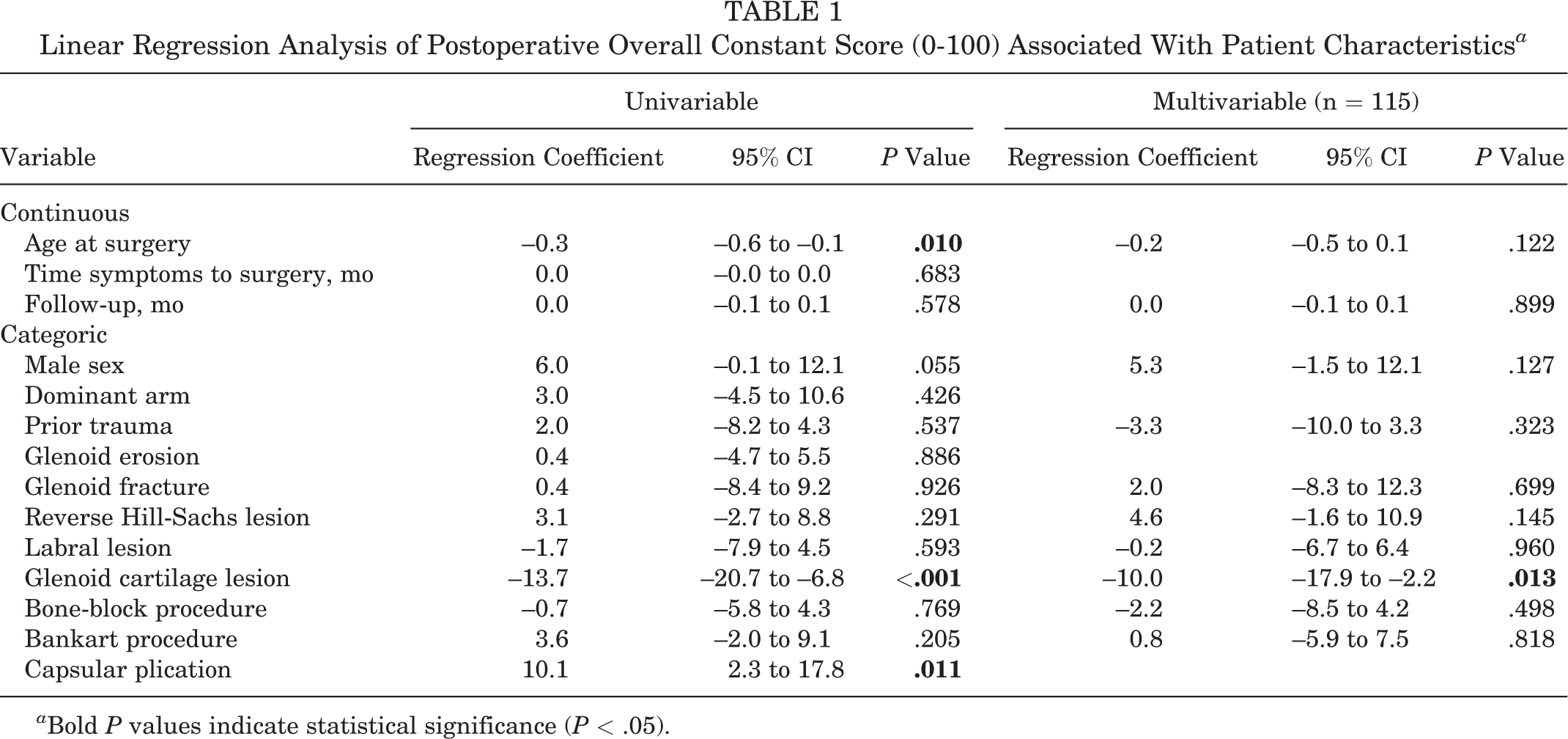
a Bold P values indicate statistical significance (P < .05).
Linear Regression Analysis of Postoperative Pain Component of Constant Score (0-15) Associated With Patient Characteristics a

a Bold P value indicates statistical significance (P < .05).
Uni- and multivariable regressions revealed that the Walch-Duplay score was significantly associated with only glenoid cartilage lesion (beta = –16.6; P = .001 and beta = –16.0; P = .007 [respectively]) (Table 3).
Linear Regression Analysis of Postoperative Walch-Duplay Score (0-100) Associated With Patient Characteristics a
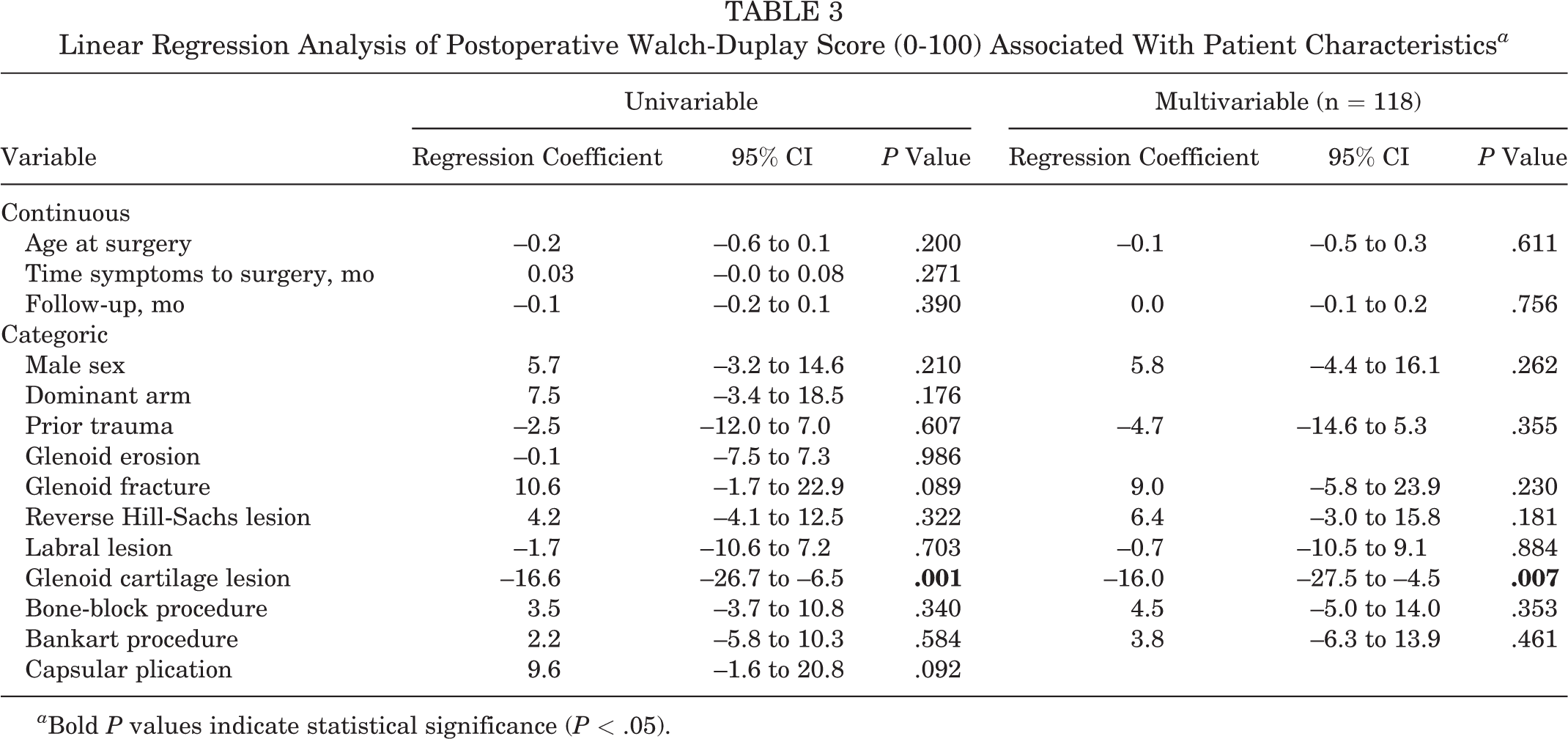
a Bold P values indicate statistical significance (P < .05).
Glenoid cartilage lesions also seemed to be associated with older age, glenoid erosion, and longer follow-up, as well as worse Constant score and Walch-Duplay score across all subcomponents (pain, mobility, activity/sport/function, strength) (Table 4).
Descriptive Data Stratified by Glenoid Cartilage Lesion a

a Bold P values indicate statistical significance (P < .05).
Discussion
The purpose of this study was to investigate the demographic, lesional, and surgical factors that influenced functional outcomes in patients who underwent surgery for posterior shoulder instability. Our principal finding was that the presence of glenoid cartilage lesions jeopardized functional outcomes, which reduced the Constant score and Walch-Duplay score by 10 and 16 points, respectively. Our secondary finding was that, contrary to our expectations, none of the demographic or surgical factors considered had a significant influence on functional outcomes. Our findings therefore refute our hypothesis that functional outcomes would be better for patients treated with bone-block procedures.
The management of shoulder instability requires precise assessment and recognition of concomitant pathologies. While surgeons have a well-established decision tool for the diagnosis and treatment of anterior shoulder instability, 2 there is no such a tool for posterior shoulder instability. Our findings cannot be used to draw comprehensive guidelines when dealing with posterior shoulder instability. Nonetheless, the consistent deleterious effects of glenoid cartilage lesions on all outcomes enable us to make diagnostic and therapeutic recommendations.
The etiology of posterior shoulder instability is often multifactorial, with possible concomitant labral, glenoid, posterior capsular, or rotator cuff lesions, which are challenging to identify radiographically. 13,29 This is true of cartilage lesions, which are not visible on conventional magnetic resonance images or computed tomography. As our first recommendation, we suggest that the radiographic protocol for patients with posterior shoulder instability include contrast-enhanced imaging, such as computed tomography arthrography or magnetic resonance arthrography, 35,38,42 which provides the most sensitive examination of the posterior capsulolabral complex. 43 This would ensure earlier and accurate detection of glenoid cartilage lesions, which are otherwise often found incidentally 8,14,31,36 and may be confused with posterior omarthrosis.
A minimum of 6 months of conservative management is generally prescribed as initial treatment for shoulder instability, before surgery is considered. 41,43 Surprisingly, the time from symptoms to surgery did not significantly affect clinical scores, but patients with cartilage lesions were older (median, 33 years) than patients with no cartilage lesions (median, 26 years). However, as glenoid cartilage lesions are degenerative by nature, 14 our second recommendation is therefore to consider rapid surgical intervention even for shoulders with minor glenoid cartilage lesions, before they deteriorate and engender irreversible effects. Please note that further studies are required to confirm this recommendation, as patients with severe injuries could also have concomitant cartilage lesions at the time of injury. By the same token, surgeons should manage patient expectations by informing those with glenoid cartilage lesions about the risks of worse functional outcomes and adapting rehabilitation programs and return to sports accordingly.
Contrary to our hypothesis, none of the demographic or surgical factors considered had a significant influence on functional outcomes at follow-up of 5 years. To our knowledge, this is the first study of shoulder posterior instability to include a comprehensive investigation of radiographic factors in nonathletic patients and to identify glenoid cartilage lesion as a functional risk factor. This finding corroborates the conclusions from previous studies on posterior shoulder instability that cartilage damage is associated with poorer outcomes. 18 Studies assessing the clinical outcomes of arthroscopic repairs in athletes with posterior instability suggested that excessive retroversion, 17,30 glenoid dysplasia, 17 and increased capsular area were associated with recurrence of instability, 17 although a later study found that the presence of glenoid dysplasia did not influence clinical outcomes or revision rates. 16 In their review article of shoulder instability in contact athletes, DeLong and Bradley 13 enumerated preoperative clinical factors predictive of poor response to surgery, including hyperlaxity and multidirectional and voluntary instability. Given the multicentric retrospective design of this study, we could not include these clinical variables in our analysis.
The present study presents a number of additional limitations typical of retrospective cohort series: (1) Pre- and postoperative sport/activity levels, which could influence the severity of the pathology and the outcomes, were not reported; however, a previous study showed that athletic and nonathletic patients had similar functional postoperative outcomes. 6 (2) The extent or severity of glenoid cartilage lesions was not quantified or recorded. (3) We did not record preoperative clinical scores, and it is possible that patients with glenoid lesions could have worse preoperative scores. (4) Multivariable analysis of recurrence of instability could not be performed because of an insufficient number of events. (5) There was a very low proportion of isolated capsular plication. Furthermore, contrary to anterior shoulder instability, 44 there is no accepted minimal amount of bone loss required to perform bone-block procedures for posterior instability. As a result, the amount of bone loss deemed necessary for bone-block procedures was left to surgeons’ discretion. In the present series from France, the proportion of bone-block procedures is considerably higher than what is reported in the United States 40 and may no longer represent common practice. The strengths of this study include a sizable cohort of a rare pathology, a substantial collection of postoperative clinical scores, and the multicentric study design, which dilutes center and surgeon effect on patient selection and operation.
Conclusion
A 17% recurrence rate was seen in patients undergoing surgical treatment for posterior instability. None of the demographic or surgical factors considered had a significant influence on functional outcomes. The only factor reported that jeopardized functional outcomes of posterior instability surgery was the presence of glenoid cartilage lesions.
Footnotes
Acknowledgment
The authors are grateful to Hugo Bothorel, Aude Michelet, and Mo Saffarini for their support with data management, statistical analysis, and manuscript redaction.
Final revision submitted September 5, 2019; accepted September 16, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.M. receives consulting fees from Stryker, Wright-Tornier, and Zimmer-Biomet. A.G. receives consulting fees from Arthrex, ConMed, and Wright Medical and royalties from FH and Wright Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hôpital Privé Jean Mermoz and the Centre Orthopédique Santy (study 2018-04).