
Abstract
Background:
Tunnel placement is important for outcomes after acromioclavicular (AC) joint reconstruction, yet little has been written on sex-based differences in optimal tunnel positioning.
Hypothesis:
No sex-based or anatomic differences will be found in ideal tunnel position based on radiographic measurements.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The records of 2382 patients were retrospectively examined for clavicle radiographs over a 20-year period. A random set of radiographs were reviewed until 200 radiographs from each sex met inclusion criteria per a priori power analysis. Anteroposterior clavicle radiographs were used to collect (1) length from lateral clavicle to lateral coracoid (LCLC), (2) length from lateral clavicle to medial coracoid (LCMC), (3) clavicle length (CL), and (4) clavicular depth at the midcoracoid (MCCD). The Student t test was used to compare differences between male and female patients. The Pearson correlation coefficient was used to measure linear correlations. Variables with a P < .1 were included in a multiple regression model.
Results:
The cohort included 200 men and 200 women. LCLC and LCMC were significantly greater for men than for women (P < .0001). Clavicle length was significantly correlated with LCLC (r = 0.63; P < .0001) and LCMC (r = 0.74; P < .0001). MCCD was significantly correlated with LCLC (r = 0.32; P < .0001) and LCMC (r = 0.43; P < .0001). The approximate placement for the trapezoid tunnel was found to be 22.1 mm in women and 26.6 mm in men. The approximate placement for the conoid tunnel was found to be 40 mm in women and 46.6 mm in men. The ratios (LCLC:CL and LCMC:CL) were also significantly different between female and male patients. The LCLC:CL was 0.144 in women and 0.154 in men (P < .0001). The LCMC:CL was 0.261 in women and 0.271 in men (P < .0006).
Conclusion:
Significant sex-based differences are found in the position of the coracoid relative to the lateral edge of the clavicle. Coracoid position relative to the lateral edge of the clavicle is correlated with anatomic parameters, most strongly with clavicle length.
Keywords
Acromioclavicular (AC) joint dislocation is a common injury, most frequently sustained in high-speed vehicle collisions and direct contact sports, where nearly half of all shoulder trauma involves the AC joint. 17,19 Treatment is typically nonoperative for lower grade injuries; however, patients with higher grade dislocations with complete rupture of the coracoclavicular (CC) ligaments and significant displacement may benefit from surgical reconstruction. 19,25 A variety of surgical techniques have been described, including coracoclavicular screws, hook plates, Endobutton coracoclavicular fixations, and the Weaver-Dunn procedure. 19,20,22 Recent studies of anatomic ligament reconstruction of the CC ligaments after AC joint dislocation using tendon graft have demonstrated advantages. 4,5,17,20,25 This reconstructive technique involves passing an autograft or allograft tendon around the coracoid, through 2 clavicular bone tunnels, to re-create the conoid and trapezoid ligaments, with or without supplemental fixation. 4,20,25 For accurate intraoperative placement of bone tunnels, identifying the precise attachments of these ligaments is essential, as both medialization and lateralization of the tunnels have been shown to be associated with a higher rate of early failure of the reconstruction. 3,4,25
Prior studies have assessed the location of the conoid and trapezoid ligaments anatomically in cadaveric specimens and noted differences in the measured distances from the lateral clavicle to the ligamentous origins in different populations based on race and sex. 17,26 Both studies found that although there are absolute differences in distance, the ratio of the ligamentous origins to the size of the clavicle is constant. 17,26 Recommendations for placement of the conoid tunnel at 45 mm and the trapezoid tunnel at 30 mm from the lateral clavicle are often misquoted as absolute distances instead of ratios. 17 Patients with smaller clavicles may be at greater risk for medialization of tunnel placement if absolute numbers are widely used. This study aimed to identify whether there are sex-based or anatomic differences in ideal tunnel placement for CC ligament reconstruction based on plain radiographs. Our null hypothesis was that there would be no sex-based or anatomic differences in the position of the coracoid relative to the lateral edge of the clavicle based on radiographic measurements.
Methods
After institutional review board approval was granted, a retrospective review was conducted for all patients who received plain radiographic imaging of a clavicle at 2 urban academic institutions over a 20-year period from January 1998 to December 2018. Patients were identified through billing records for Current Procedural Terminology code 73000 (diagnostic imaging, clavicle). Exclusion criteria included age younger than 18 years or older than 44 years, open physes, presence of acute clavicle fracture or evidence of prior clavicle fracture, prior open reduction and internal fixation of the clavicle, any indwelling hardware, AC or sternoclavicular dislocation, or tumor affecting the clavicle. The age range was chosen to most appropriately represent patients who typically sustain these injuries. A random set of radiographs were reviewed until 200 radiographs from each sex met inclusion criteria per a priori power analysis. Patient sex, age, and height at the time of radiographic imaging were recorded.
Radiographs were measured through use of a picture archiving and communication system (PACS) (Centricity; Partners Healthcare). The accuracy of the PACS ruler was established by measuring an anatomic landmark with a known distance, which was found to be accurate within 0.1 mm. 16 Anteroposterior radiographs were used for measurements. We measured 4 distances: (1) length of the lateral clavicle to the lateral coracoid (LCLC), (2) length of the lateral clavicle to the medial coracoid (LCMC), (3) total clavicle length (CL), and (4) depth of the clavicle at the midcoracoid (MCCD). LCLC was measured from the center of the lateral-most edge of the clavicle to the center of the clavicle at the line tangential to the lateral-most edge of the coracoid, and most closely represents the trapezoid tunnel, at the center of the trapezoidal tuberosity. 11 LCMC was measured similarly, using a line tangential to the medial-most edge of the coracoid, and most closely represents the conoid tunnel, at the center of the conoid tuberosity. 11 CL was determined by measuring the distance between the center of the medial margin of the clavicle to the center of the lateral margin of the clavicle. MCCD was measured from the superior edge to the inferior edge of the clavicle along a vertical line at the midcoracoid (Figure 1). The base of the coracoid was used in all measurements. All measurements were made by a single observer (K.A.B.). The intraclass correlation coefficients between duplicate measurements in 20 random patients were used to assess intraobserver reliability. Coracoid width (CW) was calculated from the difference between the LCLC and LCMC.
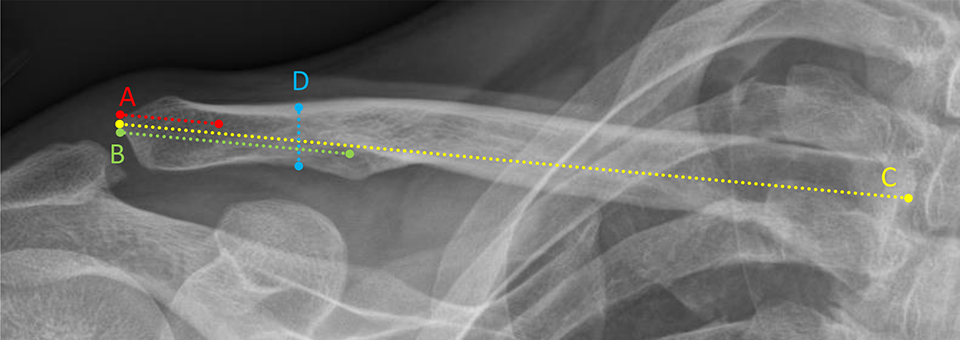
Measurements of the clavicle: (A) length of the lateral clavicle to the lateral coracoid, (B) length of the lateral clavicle to the medial coracoid, (C) clavicle length, and (D) depth of the clavicle at the midcoracoid.
Statistical Analysis
Descriptive statistics were calculated for the study cohort. The Student t test was used to compare differences in LCLC and LCMC between male and female patients. The Pearson correlation coefficient was used to measure linear correlation between LCLC and LCMC and continuous variables. Variables that met the inclusion criterion of a P < .1 in the bivariate analysis were included in the multivariable analysis. Multiple regression analysis was performed to find variables independently associated with LCLC and LCMC. The standard significance criterion of α = 0.05 and standard power criterion of (1-β) = 0.80 were used for all statistical tests. An a priori power analysis was performed. Assuming a mean LCMC of 40 ± 5 mm 17 and a 5% difference between sexes, a sample size of 98 patients in each group yields 80% power to detect a significant difference.
Results
Billing records identified 2382 patients who received clavicle radiographs between 1998 and 2018. Of those, 165 were excluded for age younger than 18 years or older than 44 years, 208 were excluded for open physes, 642 were excluded for presence of acute or evidence of prior clavicle fracture, 255 were excluded for prior open reduction and internal fixation of the clavicle or any indwelling hardware, 93 were excluded for dislocation at the AC or sternoclavicular joint, 22 were excluded for tumor affecting the clavicle, and the remaining 597 were excluded due to poor imaging or lack of available imaging. Radiographs were reviewed consecutively from the billing-generated list, and once 200 radiographs from each sex met inclusion criteria, enrollment was completed.
Mean age of the cohort was 28.6 years. The mean patient height was 169.2 cm. The mean CL was 162.7 mm, MCCD was 12.4 mm, LCLC was 24.3 mm, LCMC was 43.3 mm, and CW was 19.0 mm. The intraclass correlation coefficients for LCLC, LCMC, CL, and MCCD were 91.6%, 96.6%, 95.3%, and 88.2%, respectively, indicating excellent intraobserver reliability.
Within the female group, the mean patient height was 162.0 cm. Based on measurements of the 200 radiographs of the female group, the mean CL was 153.1 mm, MCCD was 11.1 mm, and CW was 17.9 mm. The mean LCLC was 22.1 mm and the mean LCMC was 40.0 mm, indicating the approximate placement of the tunnels for the trapezoid and conoid ligaments, respectively.
Within the male group, the mean patient height was 176.4 cm. Based on measurements of the 200 radiographs of the male group, the mean CL was 172.2 mm, MCCD was 13.7 mm, and CW was 20.0 mm. The mean LCLC was 26.6 mm and the mean LCMC was 46.6 mm, indicating the approximate placement of the tunnels for the trapezoid and conoid ligaments, respectively.
The ▵ (Male – Female) for CL was 19.1 mm, for MCCD 2.6 mm, for CW 2.1 mm, for LCLC 4.5 mm, and for LCMC 6.6 mm (Table 1). Sex was found to be significantly associated with differences in LCLC and LCMC: Male patients had significantly greater LCLC (P < .0001) and significantly greater LCMC (P < .0001). The ratios (LCLC:CL and LCMC:CL) were also significantly different between female and male patients. The LCLC:CL was 0.144 in female patients and 0.154 in male patients (P < .0001). The LCMC:CL was 0.261 in female patients and 0.271 in male patients (P < .0006).
Sex-Based Differences in Mean Anatomic Parameters in Coracoclavicular Ligament Reconstruction a

a CL, clavicle length; CW, coracoid width; LCLC, length of the lateral clavicle to the lateral coracoid; LCMC, length of the lateral clavicle to the medial coracoid; MCCD, depth of the clavicle at the mid-coracoid.
b Values are expressed as mean ± SD.
Patient height was significantly correlated with LCLC (r = 0.28; P < .0001) and LCMC (r = 0.36; P < .0001). CL was significantly correlated with LCLC (r = 0.63; P < .0001) and LCMC (r = 0.74; P < .0001). MCCD was significantly correlated with LCLC (r = 0.32; P < .0001) and LCMC (r = 0.43; P < .0001).
Sex, patient height, CL, and MCCD were included in the multivariable analysis. Multiple regression analysis showed that sex (P = .005), CL (P < .0001), and MCCD (P < .01) were significantly associated with LCLC. Sex (P = .04) and CL (P < .0001) were significantly associated with LCMC. MCCD was not independently associated with LCMC. Patient height was not independently associated with either LCLC or LCMC.
Discussion
This study demonstrated significant differences in measurements of the clavicle and coracoid position in men and women. AC joint dislocation is a common injury that occurs in active people, and patients with higher grade injuries may benefit from surgical management. 19,20 Many different types of surgeries have been described to treat this condition. Earlier techniques that relied on AC ligament transfer have been associated with recurrent subluxation-dislocation and hardware breakage. 22,23 Given the failures seen with nonanatomic reconstructions, Fukuda et al 9 postulated in 1986 that “if maximum strength of healing after an injury to the AC joint is the goal, all ligaments should be allowed to participate in the healing process.” Subsequent techniques have shifted to CC ligament reconstruction in an effort to more effectively restore anatomic alignment and function. 6,12
Cadaveric studies evaluating the restraining forces on the AC joint demonstrate that the AC ligament is the primary restraint to anterior and posterior displacement. 21 Sectioning of the CC ligaments, especially the conoid, results in superior displacement of the clavicle (or inferior displacement of the scapulohumeral complex relative to the clavicle), 21 and Fukuda et al 9 and Lee et al 14 demonstrated the importance of the CC ligaments in limiting superior and posterior AC joint displacement. Reconstruction of the CC ligaments has thus become an important part of the surgical treatment of high-grade AC joint dislocation.
Recent data suggest that CC ligament reconstruction with tendon graft secured via bone tunnels leads to more favorable outcomes with higher grade AC joint injuries. 2,15,17 The use of tendon graft for reconstruction was first reported by Jones et al, 13 who used an autogenous semitendinosus tendon graft to reconstruct the AC joint. Mazzocca et al 15 incorporated these prior works to first describe an anatomic AC joint reconstruction in 2004. Appropriate tunnel placement has been demonstrated to be important for patient outcomes. Geaney et al 10 showed that when tunnels were placed too laterally in cadaveric models, graft pullout strength was decreased. Further, several studies have demonstrated increased failures with medialization of the tunnels. 5,8,16 Despite the publications by Mazzocca et al 15 and Rios et al 17 noting that placement measurements are not meant to be absolutes, the absolute numbers of 45 and 30 (15 mm away) are widely publicized on online sites and would be expected to lead to medialization in patients with shorter clavicle lengths. 1,24
Cadaveric studies have provided improved knowledge of osteological characteristics and optimal tunnel placement. Rios et al 17 evaluated 19 fresh-frozen cadaveric clavicles with intact CC ligaments and an additional 120 dry clavicles and demonstrated that male and female specimens had significant differences in lengths, sizes, and widths but similar ratios of the ligamentous origins to total clavicle length. The investigators recommended a 5-mm oblique bone tunnel placed 40 to 45 mm from the lateral edge of the clavicle (for conoid tunnel) with the trapezoid tunnel placed 15 mm anterolateral to the conoid tunnel, but they noted that measurements should be taken intraoperatively. 17 More recently, Shibata et al 18 evaluated 25 cadaveric clavicles (17 male, 8 female) and confirmed that although the anatomic differences in coracoid position based on radiographic evaluation were different between the sexes, the ratio to total clavicle length was constant.
Our study goals were to assess sex-based and anatomic differences in ideal tunnel placement based on radiographic evaluation. We identified that LCLC and LCMC were significantly different among female and male patients. Our numbers are quite similar to those of prior osteology studies and confirm those osteological results via radiographic evaluation. 17,18 Local anatomic parameters such as CL and MCCD were significantly associated with LCLC and LCMC and may affect surgical planning by treating providers. Although patient height was significant in the bivariate analysis, this variable was not significant in multivariable analysis. Local osteological features and sex were shown to be the factors significantly associated with LCLC and LCMC.
Several studies have demonstrated increased failure rates with a medialized clavicular bone tunnel position in AC ligament reconstruction. 4,7 Cook et al 4 demonstrated early radiographic failure in a young military population (sex was not specified) with a conoid tunnel ratio of greater than 0.3 and recommended placing the conoid tunnel at 25% of the total clavicular length. Eisenstein et al 7 reviewed 38 male patients in whom 20 radiographic failures were noted; the investigators recommended that optimal tunnel placement would be between 20% and 25% of total clavicular length. Both studies demonstrate the importance of anatomic bone tunnel placement with AC joint reconstruction to avoid failure. Preoperative measurements of total clavicular length are necessary to anatomically place the conoid ligament at 20% to 25% and the trapezoid ligament at less than 16% of the total clavicular length. 4 Medialization of the clavicular bone tunnel position led to early failure in both studies with most, if not all, male patients.
Both LCLC and LCMC were found to have a strong positive correlation with CL, indicating that clavicle length is an important predictor of the anatomic location and width of the coracoid. As we have demonstrated, women are more likely to have shorter clavicle lengths, LCLC, and LCMC. Further clinical studies are indicated.
This study has several limitations. First, the radiographs were obtained retrospectively by billing records. Although the patients’ ages were chosen to most appropriately reflect the patient population who typically sustain these injuries, the patients in this study were not from a group of patients who have sustained this injury. Second, measurements were taken from a single radiograph, and therefore slight changes in orientation, projection, or magnification in radiographic technique could lead to differences in measurements. Although this limits the accuracy of our measurements, this scenario is true to life and clinical practice. While one might expect differences in radiographic technique to regress our results toward the mean, significant differences were identified in all explanatory variables in the bivariate analysis. Our study does not speak to the relative utilities of other radiographic views, such as the Zanca view. Third, given that these were not radiographs of surgical patients, we do not have clinical outcomes to know the success of using these measurements for tunnel placement. Fourth, our study used radiographs to make measurements rather than computed tomography scan, which may be more accurate but is also costlier. All patients will likely have had plain radiographs, which provide an inexpensive preoperative method for planning tunnel placement.
Strengths of the study include high intraobserver reliability: A single examiner performed all measurements and demonstrated consistency. All measurements were performed through use of the same electronic radiographic system in a reproducible and concise manner. The large sample size at 2 institutions allows for improved generalizability of our results.
Surgeons should be aware that there are significant sex-based differences in the position of the coracoid relative to the lateral edge of the clavicle. Coracoid position relative to the lateral edge of the clavicle is also correlated with anatomic parameters, including patient height and clavicular length. Preoperative planning by measuring the individual patient’s anticipated tunnel distances may aid in avoiding tunnel malpositioning. The contralateral clavicle radiograph may serve as a useful template for measurement. Further studies are necessary to correlate these parameters with CC bone tunnel positions and clinical results.
Footnotes
Final revision submitted September 24, 2019; accepted September 27, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.G.M. has received consulting fees from Smith & Nephew, educational support from Kairos Surgical, speaking fees from Arthrex, and hospitality payments from Nuvasive. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Partners HealthCare system (protocol #2010P002462).