
Abstract
Background:
Lack of uniformity in reported outcomes makes comparisons between acromioclavicular joint (ACJ) injury studies challenging. Knowledge of common outcome measures and standardization will help orthopaedic surgeons report and compare outcomes more consistently.
Purpose:
To identify the most commonly reported outcome measures for ACJ injuries.
Study Design:
Systematic review.
Methods:
A systematic review was performed to identify all English-language original articles assessing any type of management of ACJ injuries (acute and chronic) in PubMed and Scopus from 2007 to 2017. Review articles, meta-analyses, studies with less than 5 patients, pediatric studies, technique articles, and biomechanical studies were excluded. The 100 top orthopaedic journals in the English literature were selected for review. Included studies were assessed for patient characteristics and the use of outcome variables, including range of motion (ROM), strength, patient-reported outcomes (PROs), satisfaction, return to work, return to sport, and complications.
Results:
A total of 605 unique articles were identified; 92 met the inclusion criteria. The average number of ACJ injuries per study was 37, with a mean weighted patient age of 36 years (range, 20.1-57.3 years). The mean follow-up was 36 months (range, 5-290 months). Acute injuries were reported in 59% of studies. ROM and strength measurements were reported in 22.8% and 5.4% of studies. Sixteen different PRO instruments were used. The most commonly reported measures were Constant score (75%), visual analog scale for pain (VAS-pain; 33%) score, American Shoulder and Elbow Surgeons (ASES) score (21%), Simple Shoulder Test (SST) score (19%), and University of California Los Angeles (UCLA; 17%) shoulder score. An average of 2.5 outcome measures per study were reported. The use of 4 or more outcome scores was associated with publication in higher–impact factor journals.
Conclusion:
Inconsistent reporting of multiple outcome measures is present in the ACJ injury literature. The best scoring system for assessing ACJ injury and treatment has not yet been agreed upon. Until improved scoring systems come into general use, we recommend that future literature on ACJ injuries use at least 4 outcome scores and include the commonly used outcome measures (Constant, VAS-pain, ASES, and SST scores) to enable future comparison of patient outcomes across publications.
Keywords
Outcome measures used to evaluate the management of acromioclavicular joint (ACJ) injuries are not consistently reported in the literature. The lack of uniformity in reported outcomes and the abundance of techniques described make comparing studies difficult. 12,14,21 ACJ injures are not the only diagnosis with this problem; as Gerber 10 stated, “The lack of a universally accepted, standardized system of assessing the overall value, or functional state, of a normal, diseased, or operated joint is one of the most important factors preventing progress in clinical orthopaedic research.” During the past 30 years, the methodology of measuring orthopaedic procedure outcomes has changed dramatically, with a focus on patient- and physician-derived outcome scores. Over 40 different outcome measures have been identified for shoulder pathology. 11 Often, the sensitivity, validity, and reproducibility have not been evaluated for a specific outcome score in the setting of specific shoulder diagnoses. 11,17 In addition, shoulder outcome measures used to evaluate similar disorders have varied and have demonstrated low interrater reliability and low correlations between different outcomes. 3,18,19
The uses of health-related quality of life (HRQOL) and patient-reported outcomes (PROs) have increased and are being promoted for the evaluation of the effectiveness of treatment in orthopaedics. 2,9,20 These outcome metrics are often reported in the literature as a measure of clinical outcome. There are a multitude of outcome measures available to assess the treatment of ACJ injuries and other shoulder disorders, including the Constant score, Simple Shoulder Test (SST) score, Disabilities of the Arm, Shoulder and Hand (DASH) score, American Shoulder and Elbow Surgeons (ASES) score, and University of California Los Angeles (UCLA) shoulder score, among many others. Within the orthopaedic literature, the 36-Item Short Form Health Survey (SF-36) and 12-Item Short Form Health Survey (SF-12) are the most frequently used and validated HRQOL assessment tools. 26,27
The optimal outcome measure (or measures) used to evaluate ACJ injuries and to assess the efficacy of treatment remains uncertain. There is no current gold standard assessment for shoulder injuries or for ACJ injuries, making cross-study comparisons and meta-analyses difficult. 5,21 The development of questionnaires and shoulder scoring outcome measures that are condition specific and normalized for age and sex that represent both the patients’ and clinicians’ perspectives would be beneficial. 8,25 This is particularly important in the ACJ literature, given the myriad techniques and differing indications in the treatment of these injuries. 4,7,14,16,23
The aim of this study was to evaluate and identify the most commonly reported outcome measures used in the management of ACJ injuries (both nonoperative and operative) in the recent literature. A secondary goal of this study was to recommend a guideline to report outcomes for future studies, including patient-reported and objective outcome measures, to assist in the advancement of orthopaedic literature in relation to the management of ACJ dislocations.
Methods
A systematic review was performed to include all published studies in the English-language literature evaluating ACJ injuries between January 1, 2007, and March 31, 2017. A targeted search was performed using key search terms. The 2 publication databases searched were Scopus and PubMed. The 100 top orthopaedic and sports medicine journals were selected for review based on the SCImago ranking system from 2016.
Inclusion/Exclusion Criteria
Studies were included if they reported on the treatment of acute or chronic ACJ dislocations, including nonoperative management or any form of surgical stabilization. Exclusion criteria were as follows: biomechanical studies, studies with patients younger than 16 years, studies with less than 5 patients, studies where the primary injuries were distal clavicle fractures, case studies, pure radiographic or anatomic studies, review articles (systematic review/meta-analysis), non–English language publications, surgical technique articles that did not report on outcomes, editorials, studies focusing on revision surgeries, and articles focused on only a single complication.
Data Collection
All included study data were collected on a web-based platform (Microsoft Excel via Google Docs). No attempt was made to contact the individual study authors, as the goal of this study was to evaluate the current published literature. Duplicate studies were removed. All articles were screened via title or abstract evaluation by the research team, and determination of possible inclusion or definite exclusion was performed. When articles were found to be appropriate for the study based on the title or abstract review, they underwent a full-text review.
All included studies were reviewed by a minimum of 2 authors, with 1 being a senior author (J.J.K., B.S.S., K.W.F., and T.W.W.). Characteristic article data included the following: impact factor of the journal in which it was published, level of evidence (LOE), country of study, number of ACJ separations, number of total patients, mean length of follow-up, minimum length of follow-up, patient age, sex, smoking status, retrospective or prospective study, isolated ACJ injuries versus mixed studies (ie, including fractures also), chronicity of injury, ACJ separation grade, and types of treatment used.
Outcomes Evaluated
Any outcome measure or score used in a study was recorded. Other common outcomes aside from shoulder function scoring measures evaluated were patient satisfaction, return to activities of daily living (ADL), return to work, return to activity or sports, revision surgery rate, acromioclavicular subluxation rate, and complication rate.
Shoulder range of motion (ROM) was recorded when an article reported flexion, abduction, external rotation, or internal rotation ROM measures. Measures of strength were recorded if the study included forward flexion, abduction, external rotation, or internal rotation measures. A study was considered to have a strength measurement only when a quantitative force assessment was reported.
Bias
Bias was not assessed in the individual studies, as the goal of this study was to assess the outcome measures used in the published literature. Only the top 100 orthopaedic journals were included to remove any bias from the lowest level studies.
Subanalyses
The average number of outcomes measured, as well as the percentage of each outcome, was determined based on all studies. Characteristic data including mean age and follow-up were assessed using weighted means with the number of patients in each study. Several other variables were compared, including journal impact factor (<1.5 vs ≥1.5), LOE (1-3 vs 4), and total number of outcome scores used (<4 vs ≥4). The cutoff for impact factor of 1.5 was used, as the higher level journals tended to have a SCImago impact factor above 1.5. The Fisher exact test for categorical variables was used for univariate analysis, and an unpaired Student t test was used for continuous variables. The alpha level for statistical significance was set to 0.05.
Results
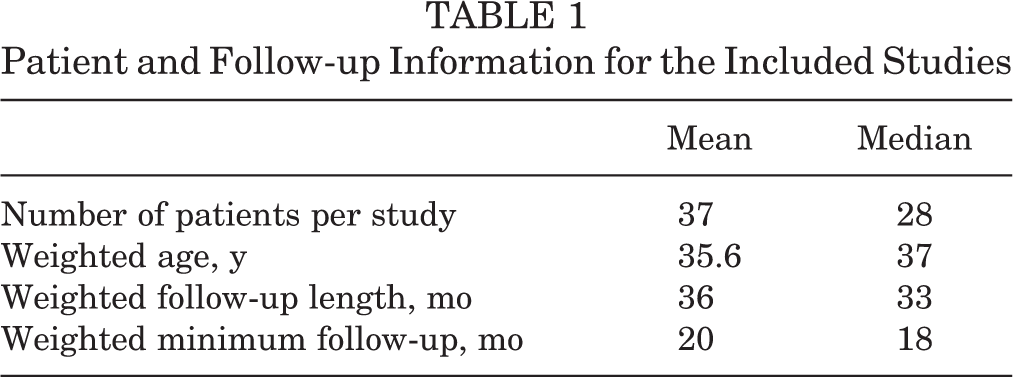
From the initial literature search of 919 articles, 92 studies reporting on 3453 patients were included (Figure 1). The mean number of ACJ dislocations per study was 37 (range, 6-154), with a mean weighted patient age of 35.6 years (range, 20.1-57.3 years). Female patients accounted for 2.8% of all patients studied. The average weighted follow-up was 36 months (range, 5-290 months), with an average weighted minimum follow-up of 20 months (range, 0.5-252 months). Characteristics of study patients are outlined in Table 1. Studies of isolated ACJ dislocations comprised 80% of all articles reviewed.

Flowchart of included articles and articles reviewed.
Patient and Follow-up Information for the Included Studies
Patient-Reported Outcomes
A total of 16 different outcome scores used for functional shoulder assessment were identified (Table 2). On average, 2.5 outcome measures were used per study. The Constant (or normalized Constant) score was the most commonly used outcome measure reported (75%), followed by the ASES score (21%) and SST score (19%). The visual analog scale for pain (VAS-pain) was used in 33% of studies and far exceeded any other pain outcome score reported (3%).
Reporting of Outcome Measures a

a ACJI, acromioclavicular joint instability score; ASES, American Shoulder and Elbow Surgeons score; DASH, Disabilities of the Arm, Shoulder and Hand; QuickDASH, shortened 11-item form of DASH score; SANE, Single Assessment Numeric Evaluation; SF-12/SF-36, 12-Item/36-Item Short Form Health Survey; SPADI, Shoulder Pain and Disability Index; SST, Simple Shoulder Test; SSV, subjective shoulder value; UCLA, University of California Los Angeles; VAS-pain, visual analog scale for pain; WOSI, Western Ontario Shoulder Instability Index.
Patient-reported surveys on general health, such as the SF-12 and SF-36, were found in only 2% of studies.
ROM and Strength
Isolated reporting on shoulder ROM was infrequent, observed in only 22.8% of articles (Table 3). Forward flexion was the most commonly reported measurement (16.3%), followed by abduction (12%) and external rotation (12%).
Range of Motion and Strength Measurement Reporting a

a ROM, range of motion.
Strength reporting was even scarcer in the literature and was documented in only 5.4% of studies (Table 3). Forward flexion/abduction and external rotation/internal rotation strength reporting did not significantly vary and were each reported in 3.3% to 2.2% of articles, respectively.
Other Outcomes
Patient satisfaction was reported in 42% of studies. Additional quality-of-life outcomes included return to ADL (15%), return to work (40%), return to activity or sport (46%), and time to return to play (25%). Complications were included in 79% of papers, along with acromioclavicular subluxation or loss of fixation (87%) and revision surgery rate (51%).
Level of Evidence
When comparing those studies with LOE of 1-3 versus 4, there was a statistically significant difference between the average number of outcome scores (3.2 to 2.3, respectively; P = .01) as well as the average number of shoulders studied (56.8 to 29.8, respectively; P < .001). There was no statistically significant difference between the mean patient follow-up and the mean patient age.
Journal Impact Factor
In comparing articles in journals with an impact factor <1.5 to those with an impact factor ≥1.5, there was a significant difference in the average number of outcomes scores used (2.14 to 2.88, respectively; P = .016). No significant difference was found between these 2 groups with regard to the average number of shoulders assessed, the mean patient follow-up, the mean patient age, or the LOE (Table 4).
Influence of Journal Impact Factor a

a Levels of evidence (LOEs) for the included studies ranged from 1 to 4; an LOE of 1 indicates higher quality methodology used. A larger impact factor indicates a more influential journal.
Number of Outcome Scores Used
No statistically significant difference was present between articles that used <3 outcome scores and those with ≥3 with regard to journal impact factor (1.5 to 1.9; P = .06). However, when comparing studies that used <4 outcome scores to those that included ≥4, a statistically significant difference was identified (1.5 to 2.17; P = .001) (Table 5). Of the included studies, 25% reported results from ≤1 PRO (Figure 2).

Number of outcome measures used to evaluate acromioclavicular joint injury versus the number of studies reporting them.
Comparison of Number of Outcome Scores Used a

a Levels of evidence (LOEs) for the included studies ranged from 1 to 4; an LOE of 1 indicates higher quality methodology used. A larger impact factor indicates a more influential journal.
Discussion
This study highlights the inconsistent use of various outcome measurements for ACJ injuries as reported in the current literature. In the 92 reviewed articles, 16 different outcome scores were reported. Not surprisingly, this issue with heterogeneity also exists in other studies on shoulder pathology, including rotator cuff tears 15 and superior labral tears. 22 Without the use of consistent PROs, it is difficult for orthopaedic surgeons to generalize study results or make evidence-based decisions regarding management of patients with ACJ injuries. 5,13,14,21,24
The Constant score was the most commonly reported outcome measure (75% of all studies), followed by the ASES score (21%) and SST score (19%). Similarly, 1 meta-analysis of type III ACJ injuries found that the Constant score was the most commonly used score in 63% of the 22 studies included. 14 The VAS-pain score (33% of all studies) easily exceeded any other pain outcome measure (3%). An average of 2.5 outcome scores was reported per ACJ injury study. Similar to studies on other shoulder pathology, where ≤1 PRO was reported in 13% of rotator cuff studies 15 and 25% of superior labral tear studies, 22 we found that 25% of studies on ACJ injuries reported ≤1 PRO.
The validity and reliability of several shoulder outcome scores has been examined, including that of the Constant and ASES scores for multiple shoulder pathologies. 27 This 2014 review found that the SF-36 and SF-12 are the most commonly used and proven generalized outcome scores in the orthopaedic literature, although the Constant, ASES, and SST scores are very acceptable for use. Computer-adaptive testing and the recently released PROMIS (Patient-Reported Outcomes Measurement Information System) database may become powerful evaluation tools in the future. 27 However, these remain unvalidated for the evaluation of ACJ injuries.
Several reviews 5,21 have reported difficulty comparing results because of a lack of consistent outcome measures used. When attempting to evaluate outcomes between techniques for acute high-grade ACJ dislocations, 1 meta-analysis 5 stated that many studies did not use validated scoring measures, which made comparison difficult. One systematic review 14 of type III ACJ separations found that the lack of validated outcome measures, the use of varying surgical techniques, and the lower LOE seen in the included studies contributed to the difficulty in making treatment recommendations and assessing outcomes. Another systematic review 13 of type III ACJ separations found that objective shoulder function was only reported in 4 of the 8 studies, and each study used a different outcome measure, making it impossible to combine the results. Another systematic review 21 on acute versus delayed surgical reconstruction for ACJ dislocations found that a contradictory conclusion could be drawn if a different functional outcome score was compared in 2 of the 8 included studies. These systematic reviews and meta-analyses highlight the importance of consistently reported outcome measures to allow for comparison between studies on ACJ dislocations.
Continuing to improve and develop ideal outcome measures has been the focus of several studies. Barwood et al 1 have recently created a new questionnaire called the Specific AC Score to assess acromioclavicular pathology. Questionnaire components were created from previous surveys, an expert panel, and patient feedback. The Cronbach α was high (>0.90), with acceptable internal consistency (α > 0.70), satisfactory correlation, and excellent responsiveness. Intraclass correlation of 0.89 reflected a high degree of reliability as well. 1 Charles et al 6 focused on a younger, more active patient cohort when creating the Nottingham Clavicle Score, which encompasses ACJ, sternoclavicular joint, and clavicle injuries. Their new outcome score was compared with the Constant score, Oxford Shoulder score, Imatani score, and EQ-5D, demonstrating significant correlations with each measure both preoperatively and postoperatively. The Nottingham Clavicle Score had the largest effect size (1.92) and a high internal consistency (Cronbach α > 0.87). 6
When evaluating the quality of studies, there was a statistically significant difference between studies with an LOE of 1-3 versus 4 in terms of average number of outcome scores used and number of patients studied. This discrepancy in outcome scores was also present in studies published in journals with an impact factor of ≥1.5 versus <1.5. These findings suggest that higher quality articles and higher impact journals use more PRO measures when reporting their results, indicating better data. This study shows that the use of ≥4 PRO scores was associated with higher impact journals, which suggests a target for authors to increase their chances of study acceptance. It may also aid in establishing more generalizable and standardized results, particularly if set outcome measures are agreed upon.
Limitations of this study include fundamental issues with any systematic review and inability to identify a single best outcome measure. Although a high use of the Constant score was found (75% of all studies), this does not inherently imply that it is the best outcome measure for evaluating ACJ injuries. More specific outcome tools being developed, such as the Nottingham Clavicle Score, aim to address this problem. We attempted to capture all relevant papers for ACJ injury using broad search criteria and the use of 2 commonly used databases, although the possibility exists that studies were missed. While all studies in full-text were reviewed by at least 2 authors including 1 senior author (J.J.K., B.S.S., K.W.F., and T.W.W.), there may be inconsistencies with data extraction, as not all authors reviewed each study individually. In addition, publication bias likely exists, with the literature favoring those studies with significant findings over those with equivocal results.
Strengths of this study include the high number of manuscripts reviewed using broad and inclusive search terms. Extensive data points and all reported outcomes were recorded to aid in recommendations for future studies and to describe the current literature. To our knowledge, this is the first study to systematically assess and describe the most common outcome scores used for ACJ injuries.
These findings support the heterogeneous nature of shoulder outcome scores and highlight issues encountered with ACJ dislocation studies. We recommend the use of at least 4 outcome scores for improved data reporting and the implementation of common and validated shoulder outcome scores such as the Constant, VAS-pain, ASES, and SST scores (in descending order of being commonly reported). This will allow for better cross-study comparison and generalizability of results across ACJ reconstruction surgical techniques. Increasing the reporting of other relevant outcomes such as complication rates, revision surgery, patient satisfaction, and return to work, ADL, or sports will further help guide orthopaedic surgeons on safe and effective treatment for ACJ injuries. Given the difficulty of randomized controlled trials, standardizing outcome measure reporting will improve comparison between ACJ injury studies as well as between surgical techniques, which may help orthopaedic surgeons improve the treatment algorithm for these difficult injuries.
Reported outcomes for ACJ injuries remain inconsistent across the literature. This review of the current literature shows that studies published in higher impact journals and studies with higher LOEs use 4 or more PROs. Despite the fact that the best scoring system for assessing ACJ injury and treatment has not yet been agreed upon, we recommend the use of at least 4 outcome scores (Constant, ASES, SST, and VAS-pain scores, which are the most commonly used legacy scores) based on this study. To help compare and improve findings, we encourage future studies to include common older scoring systems in addition to the developing outcome scores created recently. Given the high initial measures of validity, the Specific AC Score and the Nottingham Clavicle Score are recommended to be used and extensively analyzed. Including other outcomes such as complication rates, revision surgery, patient satisfaction, and return to work, ADL, or sport will help researchers compare outcomes among techniques. Standardization of outcome measures will allow for improved assessment of patient outcomes for ACJ injuries and help guide patient care.
Until improved scoring systems come into general use, we recommend that future literature on ACJ injuries use at least 4 outcome scores and include the commonly utilized outcome measures (Constant, VAS-pain, ASES, and SST scores) to enable future comparison of patient outcomes across publications.
Footnotes
Final revision submitted September 14, 2019; accepted September 28, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: The University of Florida Department of Orthopaedics and Rehabilitation receives research support from Exactech. B.S.S. has received educational support from Arthrex, speaking fees from DJO, royalties and consulting fees from Exectech, and hospitality payments from Zimmer Biomet. T.W.W. has received royalties from Exactech and Wolters Kluwer Health Lippincott Williams & Wilkins and consulting fees from Exactech. K.W.F. has received royalties from Arthrex and Exactech; consulting fees from Arthrex, Exactech, Flexion, and Medshape; speaking fees from CGG Medical; and honoraria from Arthrosurface. J.J.K. has received educational support from Arthrex, consulting fees from Exactech, and hospitality payments from Integra Lifesciences. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.