
Abstract
Background:
There has been a recent increase in the use of biologics in hip arthroscopy to assist in the management of femoroacetabular impingement (FAI).
Purpose:
To analyze the current use of biologics for the treatment of FAI and its associated lesions.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A search of the PubMed, Medline, and EMBASE databases was performed in March 2019 with use of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The criterion for inclusion was observational, published research articles studying the therapeutic use of biologics as an adjuvant therapy during arthroscopic surgery for FAI; treatments included bone marrow aspirate concentrate, mesenchymal stem cells (MSCs), platelet-rich plasma (PRP), hyaluronic acid, growth factors, and autologous chondrocyte implantation (ACI) or autologous matrix-induced chondrogenesis (AMIC).
Results:
There were 9 studies that met the inclusion criteria, and a total of 674 patients were included across all studies. FAI was studied in all articles. Further, 7 studies (78%) also analyzed chondral injuries, and 3 studies also analyzed labral tears (33%). ACI or AMIC was used in 56% of studies and showed superior functional outcomes at short- and midterm follow-up versus debridement or microfracture. PRP did not improve the outcome of labral repairs at short-term follow-up.
Conclusion:
The current literature regarding biologic adjuncts in hip arthroscopy is varied in quality, with only one level 1 study. The use of ACI/AMIC for medium-sized chondral lesions showed promising results in individual studies; however, these were of lower quality. To enable comparisons among future studies, investigators must ensure accuracy in the reporting of biologic preparations and formulations used and homogeneity in the type and severity of lesion treated.
Hip arthroscopy has shown great promise for the surgical management of both intra-articular and extra-articular hip lesions. 16,36 In particular, arthroscopy has been shown to be an effective treatment for femoroacetabular impingement (FAI) syndrome, which is a well-recognized cause of hip pain in the young, active population 15,36 and the most common abnormality treated by hip arthroscopy. 37 Other lesions that have been treated by hip arthroscopy include ligament teres tears, 4 psoas tendon tears, 44 and osteonecrosis of the femoral head. 37 Labral tears, chondral injuries, and osteoarthritis can often be secondary to FAI, 1,2 and it is possible to treat these during hip arthroscopy by surgical techniques and/or biologics treatments.
Biologics have become increasingly popular in orthopaedics and sports medicine over the past 20 years. 21 These agents aim to provide superior clinical outcomes by optimizing and accelerating musculoskeletal tissue healing. Current biologic treatments available include bone marrow aspirate concentrate, culture-expanded mesenchymal stem cells (MSCs) and stromal cells, autologous blood products (including platelet-rich plasma [PRP]), growth factors, hyaluronic acid, and autologous chondrocyte implantation (ACI) or autologous matrix-induced chondrogenesis (AMIC). Promising results have been shown in vitro with respect to bone 17 and cartilage regeneration. 28 Results in the clinical literature have been varied; however, encouraging results have been shown in a number of randomized controlled trials in the treatment of both lateral epicondylitis 13,27 and fracture healing. 14
Despite the recent popularization of biologics in the treatment of musculoskeletal conditions, there has been substantial heterogeneity in the reporting of the preparation, concentration, and delivery of these agents. Murray et al 32 presented the range of PRP concentrations in a recent review. The authors reported the concentration of PRP in current commercial systems to range from 1.7 to 9.3 times the platelet concentration of whole blood. Robinson et al 42 reported large variations in the source, concentration, and delivery methods of MSCs within the current orthopaedic literature.
The use of biologics in the treatment of hip joint abnormality has predominantly focused on the management of osteonecrosis of the femoral head, 38 often in conjunction with core decompression. A recent systematic review of treatment of osteonecrosis of the femoral head concluded that cell-based therapy was a safe treatment that provided improved clinical outcomes and reduced disease progression. 39 Many systematic reviews have analyzed the use of biologics in other aspects of orthopaedic surgery, including rotator cuff repair, 6,18 anterior cruciate ligament reconstruction, 9,45 and tendinopathy. 3,10,23,26,35 However, despite the increasing use of biologics in hip arthroscopy to treat FAI and its associated intra-articular abnormalities, no systematic reviews have analyzed all relevant studies.
The purpose of this study was to systematically review the current literature reporting the use of biologics in the management of FAI and its associated lesions and to compare the outcomes of these studies.
Methods
A search of PubMed, Medline, and EMBASE was performed in March 2019 in line with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. 29 The study was registered using the PROSPERO international prospective register of systematic reviews.
Titles and abstracts identified were independently reviewed by 2 authors (P.G.R., P.G.), and those studies not meeting the inclusion criteria were excluded before full-text review. When the relevance of an abstract was in doubt, the full text was subsequently reviewed. Unanimous consensus was met among the authors regarding the inclusion of proposed studies for full-text review. The studies selected for full-text review were then further evaluated against the inclusion and exclusion criteria. A search of the references was performed of the selected studies to ensure no other relevant studies were missed.
Search Terms and Criteria for Inclusion
The criteria for inclusion were observational published research articles (randomized controlled trials, cohort, cross-sectional, or case-control studies) and case series studying the therapeutic use of biologics as adjuvant therapy to arthroscopic surgery in the management of FAI; treatments included bone marrow aspirate concentrate, MSCs, PRP, hyaluronic acid, growth factors, and ACI or AMIC. Studies were excluded if they were technical or review articles, included synthetic bone matrices or bone substitutes, or were not published in the English language. For the biologic treatments studied in this review, 6 separate searches were performed in each database. The search terms were hip, femoroacetabular, impingement, arthroscopy, platelet rich plasma, mesenchymal stem cells, bone marrow aspirate, growth factors, hyaluronic acid, and chondrocyte implantation. Detailed search term combinations can be found in Appendix Table A1.
Data Extraction
The collected data from each study included the year of publication, study type, patient age, sex, body mass index, pathologic condition, type of surgery, size and severity of the chondral lesion, severity of arthritis, biologic treatment used, follow-up, outcomes, reoperation rate, conversion to total hip arthroplasty (THA), and the level of evidence.
Outcome Measures and Analysis
The primary objective was to report the variety of biologic treatments used and to compare clinical outcomes. Secondary objectives included reporting the spectrum of severity of the pathologic condition treated, establishing ideal biologic formulations for specific lesions, assessing complications, and analyzing the quality of the included studies. Data analysis was primarily in the form of reporting variables collected in the data extraction process, and efforts were made to consolidate data if they were comparable. A meta-analysis was not performed because of the heterogeneous nature of the data in each included paper.
Quality Assessment
All studies were quality assessed by 2 authors (P.G.R., P.G.) using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. The authors of the assessment tool discourage users from allocating a specific score to each study. We have not given a traditional “good,” “fair,” or “poor” rating to each study but have instead given a percentage to the number of applicable questions answered “yes.” If there was disagreement regarding the scoring of a study, consensus was met after discussion among both assessors.
Results
In the initial search of databases and reference lists, 1467 articles were identified. After initial screening of titles and abstracts, 28 articles met the inclusion criteria for review. On full-text screening, a further 19 studies were excluded (Figure 1). A final 9 studies met the inclusion criteria and are described in Table 1. The year of publication ranged from 2012 to 2016. The studies included 3 case series, 1 retrospective cohort study, 3 prospective cohort studies, and 2 randomized controlled trials. There were 3 high-level studies: 1 study was level 1 and 2 studies were level 2. A total of 674 patients were included across all studies. The mean patient age was 37.6 years (range, 16-60 years), and the overall mean ratio of male to female participants was 1 to 1.2. The mean length of follow-up was 34 months (range, 12-74 months). There were 2 studies that reported the mean body mass index, which was 25.5 (range, 25-26).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram demonstrating selection process for included studies.
Patient Demographics a
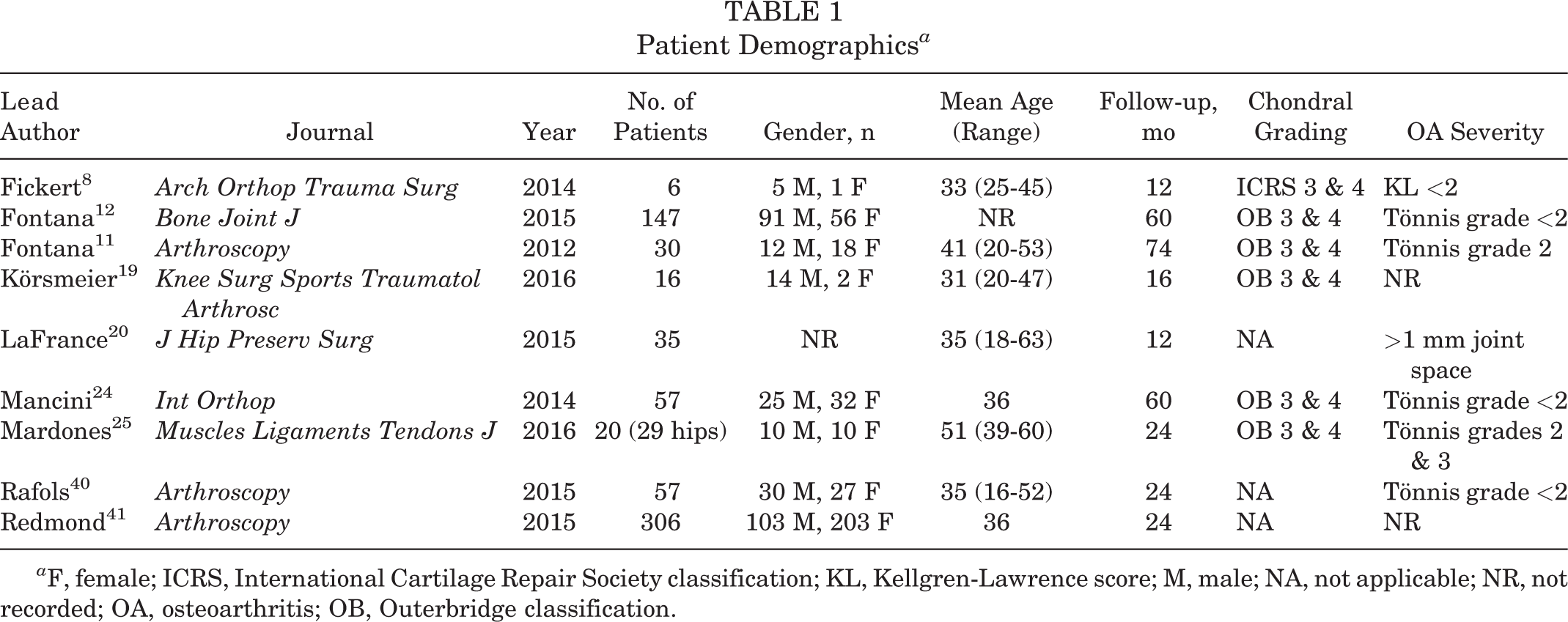
a F, female; ICRS, International Cartilage Repair Society classification; KL, Kellgren-Lawrence score; M, male; NA, not applicable; NR, not recorded; OA, osteoarthritis; OB, Outerbridge classification.
All studies used FAI as their minimum inclusion criterion, which included assessment with plain radiographs and magnetic resonance imaging (MRI). Biologic therapy was used in the adjuvant treatment of labral repairs in 3 studies (33%), chondral injuries in 8 studies (89%), and osteoarthritis in 1 study (11%). Of the studies examining chondral injuries, all reported injuries to the acetabulum, and 2 studies also examined femoral head defects (Table 2). ACI was used in 4 studies (44%), AMIC in 2 studies (22%), and PRP in 3 studies (33%). Bone marrow–derived MSCs (BM-MSCs) were used in 1 study (11%). Further, 1 study used both AMIC and ACI.
Study Design, Level of Evidence, Pathologic Condition, and Biologic Used in the Included Studies a

a ACI, autologous chondrocyte implantation; AMIC, autologous matrix-induced chondrogenesis; BM-MSC, bone marrow–derived mesenchymal stem cells; FAI, femoroacetabular impingement; LA, local anesthetic; LOE, level of evidence; MFx, microfracture; NA, not applicable; NR, not recorded; OA, osteoarthritis; PRP, platelet-rich plasma; RCT, randomized controlled trial.
Details of the surgical techniques used to treat FAI were described in 7 studies (78%). The mean proportion of patients receiving acetabuloplasty was 37.8% (range, 0%-100%), and the mean proportion receiving femoroplasty was 60.8% (range, 38%-100%). There were 5 studies (56%) that reported the method used to treat labral tears. Redmond et al 41 performed a randomized controlled trial comparing PRP versus placebo in 306 patients with labral tears. Labral repair was performed in 57% of patients, and 32% underwent labral debridement. This was the only study to report whether capsular closure or repair was performed.

Representation of the types of biologics used in the included studies. Note that Mancini and Fontana 24 used 2 biologics (AMIC vs ACI). ACI, autologous chondrocyte implantation; AMIC, autologous matrix-induced chondrogenesis; BM-MSC, bone marrow–derived mesenchymal stem cells; PRP, platelet-rich plasma (PRP).
Injury and Osteoarthritis Severity
The presence of hip osteoarthritis was reported in 8 of the included studies (89%). Tönnis grading was used in 5 studies (56%), and the Kellgren-Lawrence classification was used in 1 study (11%). A further study excluded patients with “severe osteoarthritis” but did not report how the investigators defined this. LaFrance et al 20 did not use a recognized classification but did exclude patients with less than 1 mm of joint space on anteroposterior or lateral hip radiographs. With regard to the severity of the osteoarthritis, 4 studies included patients with grade 2 or lower, on the Tönnis grading system, and 1 study included grades 2 and 3. The study using the Kellgren-Lawrence classification included grade 1 only.
Of the 8 studies reporting chondral injury, 4 studies (50%) reported the size of the lesions treated. The mean size was 3.4 cm2 (range, 2-8 cm2) (Table 2). The Outerbridge classification was used to grade the chondral lesions in 5 studies (56%), in which all studies included grades 3 or 4. One further study used the International Cartilage Repair Society score and included grades 3 and 4. Acetabular and femoral locations of the chondral injuries were reported in 2 studies (25%).
Details of Biologics Used
All studies performing ACI used a 3-dimensional technique. Körsmeier et al 19 and Fickert et al 8 used 3-dimensional spheroids cultured from chondrocytes that were harvested from the femoral head-neck junction (Chondrosphere; Co.Don AG). They were delivered without the requirement for a scaffold. Fontana et al 11 and Mancini and Fontana 24 used ACI with the chondrocytes isolated adjacent to the injury site and seeded onto a polymer scaffold composed of polylactic/polyglycolic acid and polydioxanone (Bioseed-C; Biotissue AG) before reimplantation.
The timing of delivery of chondrocytes varied among the 4 studies. Fickert et al 8 reported chondrocyte delivery 4 to 6 weeks after harvesting. Mancini and Fontana 24 reported a delivery of approximately 3 weeks after harvesting, whereas Fontana et al 11 reported a delivery time of 2 to 6 weeks postoperatively. Körsmeier et al 19 reported a delivery time of 5 to 10 weeks after harvest and described 95% cell viability at the time of surgery. No study using ACI reported the concentration of the chondrocytes delivered.
Fontana and de Girolamo 12 and Mancini and Fontana 24 both analyzed the use of AMIC. Both studies used a resorbable collagen I/III matrix (Chondroglide; Geistlich AG) in a single surgical technique. Rafols et al 40 and Redmond et al 41 both used PRP intraoperatively via percutaneous intra-articular injection after wound closure. Rafols et al used activated GPS III (Biomet), which is 7 to 8 times the whole blood concentration. Redmond et al used Arthrex ACP Double-Syringe system (Arthrex), which is 2 to 3 times the whole blood concentration. LaFrance et al 20 injected 5 mL of PRP prepared with Accelerate Concentrating System (Exactech Biologics) at the completion of the procedure after evacuation of joint fluid. The platelet concentration of this system is reported at 6 times the whole blood concentration.
Finally, Mardones et al 25 harvested BM-MSCs from the anterior superior iliac spine at the time of initial arthroscopy. Cells were then expanded to reach 20 × 106 cells and checked with immunotypification via flow cytometry for MSC markers. They were then injected once a week by radioscopic guidance at the fourth, fifth, and sixth week after harvesting.
Clinical Outcomes
The clinical outcomes of each study are described in Table 3.
Clinical Outcomes After Biologics Intervention in Hip Arthroscopy a

a ACI, autologous chondrocyte implantation; AMIC, autologous matrix-induced chondrogenesis; HOS, Hip Outcome Score; mHHS, modified Harris Hip Score; MRI, magnetic resonance imaging; NAHS, Nonarthritic Hip Score; PRP, platelet-rich plasma; SF-36, 36-Item Short Form Health Survey; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
Complications
There were 6 studies that reported reoperation rates or conversion to THA. Körsmeier et al 19 reported a reoperation rate of 12.5% at a mean follow-up of 16 months but no conversions to THA during this time. Capsular adhesions were removed in the reoperative cases, and both patients were satisfied after repeat arthroscopy. Redmond et al 41 reported a reoperation rate of 10.6% in the PRP group (reasons not reported) and 6.4% in the control group (P = .2) and a THA conversion rate of 2.9% in the PRP group and 5% in the control group (P = .4) during their 2-year follow-up. Fontana and de Girolamo 12 reported no conversions to THA in the AMIC cohort and a 7.8% conversion rate in the microfracture cohort at a mean follow-up of 38 months. No reoperations or conversions to THA were reported in the studies by Fickert et al, 8 Mancini and Fontana, 24 or Fontana et al 11 at 12-, 60-, and 74-month follow-up, respectively. Mardones et al 25 did not report any reoperations but reported a THA conversion rate of 13.8% at mean follow-up of 24 months. No complications were reported that were attributable to the delivery of the biologics.
Quality Assessment
The results of the quality assessment of included studies can be seen in Appendix Table A1. The mean percentage of successfully answered questions from the assessment tool was 67%. The level of evidence ranged from 1 to 4. The mode level was 3.
Discussion
The most significant findings were as follows: (1) a limited number of high-level articles have reported the use of biologics in the management of FAI; (2) variation existed in the timing of delivery and concentration of biologics used; (3) the use of ACI and AMIC appeared to deliver favorable results for medium-sized chondral defects at short-term to midterm follow-up compared with debridement or microfracture; and (4) the use of PRP appeared to be ineffective as adjuvant treatment of labral tears at short-term follow-up.
Chondral injuries within the hip joint have been historically problematic to treat. However, the introduction of hip arthroscopy has allowed a spectrum of treatment options to help manage these injuries. ACI has already been proven to be an effective treatment in the short to mid term for chondral lesions (>2 cm2) in the knee. 5,43 All the studies included in this review that used ACI to treat chondral injuries showed favorable patient-reported outcome scores when compared with preoperative scores and/or simple debridement or microfracture. Mancini and Fontana 24 evaluated patients up to 5 years in 3 studies analyzing the use of ACI or AMIC and showed maintained improvements in postoperative scores until final follow-up. Fontana and de Girolamo 12 compared AMIC with microfracture and noted that the microfracture cohort improved up to the 1-year follow-up but that results deteriorated from 1 to 5 years. However, this was not the case for the AMIC cohort, which showed maintained results. Furthermore, the authors stratified modified Harris Hip Scores into critical values according to treatment and chondral lesion size and found that defects larger than 4 cm2 correlated with a 2-fold incidence of low scoring in the microfracture group but did not correlate with low scoring in the AMIC cohort.
No study using adjuvant PRP to treat labral tears showed improvements in postoperative outcome measures versus well-matched, controlled cohorts. Redmond et al 41 also included other hip-related conditions, such as chondral lesions, gluteus medius tears, and ligament teres tears, whereas LaFrance et al 20 included patients who underwent psoas muscle release and/or microfracture, and therefore the 3 studies using PRP are not directly comparable. Furthermore, we noted significant differences in the PRP concentrations used. This variability in the delivered concentration of biologic formulations among studies in the current literature has already been emphasized by the authors of this study in previous reviews. 7,31,42 Murray et al 32 also highlighted the importance of selecting the correct formula of biologic most suited to the microenvironment being treated. The contrasting results in our review between PRP and ACI/AMIC may be due to delivery of subtherapeutic concentrations of PRP, mismatches between the microenvironment and the formulation, or both. Furthermore, no study routinely used postoperative interval arthroscopy to evaluate the macroscopic change in chondral lesion, and previous evidence has shown that PRP is relatively ineffective within the hip joint, particularly in cases of chondral lesions. 22
In our review, the study analyzing BM-MSCs was the most complete in reporting biologic preparation, classification, and concentration details. Details such as these have previously been recommended by an expert consensus as being pertinent to the interpretation of studies involving biologics, and minimal reporting guidelines have been established. 30 Mardones et al 25 did not compare their results of intra-articular injection of BM-MSCs to a control cohort but did show significant improvements from preoperative to postoperative functional scores at a mean follow-up of 24 months. Delivery of the cells was staggered at 3 intervals, 1 week apart. This timing of delivery has previously been shown to be effective in animal studies. 33
There were 2 studies that compared conversion rates with total hip replacement between a biologics cohort and a control cohort. Both studies reported higher rates of THA in the nonbiologics cohort. In contrast, Redmond et al 41 reported higher rates of reoperation in the biologics cohort but did not power their study to detect differences in either reoperation rate or conversion to THA. Fontana and de Girolamo 12 reported that all patients undergoing THA during their follow-up had recognized risk factors for the development of degenerative change, such as cam lesions with deep chondral lesions and lesions with a diameter greater than 4 cm2.
Other outcome measures used to determine effectiveness of biologic treatment were the postoperative presence of an effusion on MRI scanning and the appearance of the chondral lesion on second-look arthroscopy. Rafols et al 40 reported a lack of hip joint effusion in 36.7% of the PRP group compared with 21.1% of the placebo group at 6-month follow-up on MRI scanning. Körsmeier et al 19 performed arthroscopy on 2 patients at 5 and 8 months after ACI and reported hyaline-like cartilage in the area of previous implantation.
Elements of homogeneity were noted among the included studies in our review. In particular, these included a similar preoperative osteoarthritis status and similar severity of chondral injuries, with most studies using grade 3 or 4 on the Outerbridge classification. Despite this, marked differences were seen, such as variations in lesions, the treatment methods used (and reported), the concentration of PRP, the timing of delivery, the outcome measures used, the presence of a control group, and follow-up time points.
Limitations
This review must be interpreted with recognition of its limitations. Included were 3 low-level case series that simply compared pre- and postoperative outcome measures. Given the well-recognized placebo effect in orthopaedic surgery studies, these types of studies must be interpreted with caution. 46 Furthermore, only one level 1, randomized controlled trial was included in our review, and it did not report mid- to long-term follow-up. Average follow-up in this review was 20.9 months, and therefore overall failure rates and conversion to THA may be underestimated.
A variety of lesions were treated within each study, and some studies did not clearly report the exact surgical interventions performed alongside the use of the biologic agent. These details are important to include if the true efficacy of the biologic intervention is to be determined. The severity of osteoarthritis and the classification systems used to measure it varied between studies, with 1 study including patients with Tönnis grade 3 osteoarthritis. Furthermore, it is recognized that advancing age limits the function of stem cells. 34 All studies in this review included patients with a mean age older than 30 years, and 2 studies included patients with a mean age older than 40. There was paucity in the reporting of biologic preparation and concentration between studies. When these aspects were reported, variation was seen in the concentration used and timing of delivery. Finally, a relatively small number of studies were included in this review, and 3 of the studies were performed in a single center, with possible crossover in patients among those studies. Despite these limitations, the current review accurately outlines the current state of the existing literature in this area.
Conclusion
The current literature regarding biologic adjuncts in hip arthroscopy is varied in quality, with only one level 1 study. The use of ACI or AMIC for medium-sized chondral lesions showed promising results in individual studies; however, these studies were of lower quality. To enable comparisons among future studies, investigators must ensure accuracy in the reporting of the biologic preparations and formulations used and homogeneity in the type and severity of pathologic condition treated.
Footnotes
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Appendix
Search Term Combinations

| Search | Search Terms |
|---|---|
| 1 | (“hip”[MeSH Terms] OR “hip”[All Fields]) “femoroacetabular”[All Fields] OR “impingement”[All Fields] OR (“arthroscopy”[MeSH Terms] OR “arthroscopy”[All Fields]) AND (“platelet-rich plasma”[MeSH Terms] OR (“platelet-rich”[All Fields] AND “plasma”[All Fields]) OR “platelet-rich plasma”[All Fields] OR (“platelet”[All Fields] AND “rich”[All Fields] AND “plasma”[All Fields]) OR “platelet rich plasma”[All Fields]) |
| 2 | (“hip”[MeSH Terms] OR “hip”[All Fields]) “femoroacetabular”[All Fields] OR “impingement”[All Fields] OR (“arthroscopy”[MeSH Terms] OR “arthroscopy”[All Fields]) AND (“mesenchymal stem cells”[MeSH Terms] OR (“mesenchymal”[All Fields] AND “stem”[All Fields] AND “cells”[All Fields]) OR “mesenchymal stem cells”[All Fields]) |
| 3 | (“hip”[MeSH Terms] OR “hip”[All Fields]) “femoroacetabular”[All Fields] OR “impingement”[All Fields] OR (“arthroscopy”[MeSH Terms] OR “arthroscopy”[All Fields]) AND (“bone marrow”[MeSH Terms] OR (“bone”[All Fields] AND ““marrow””[All Fields]) OR ““bone marrow””[All Fields]) AND aspirate [All Fields] AND concentrate[All Fields] |
| 4 | (““hip””[MeSH Terms] OR ““hip””[All Fields]) “femoroacetabular”[All Fields] OR “impingement”[All Fields] (““arthroscopy””[MeSH Terms] OR ““arthroscopy””[All Fields]) AND (““intercellular signalling peptides and proteins””[MeSH Terms] OR (““intercellular””[All Fields] AND ““signalling” All Fields] AND ““peptides””[All Fields] AND ““proteins””[All Fields]) AND ““intercellular signalling peptides and proteins””[All Fields] AND (““growth””[All Fields] AND ““factors””[All Fields]) AND ““growth factors””[All Fields]) |
| 5 | (““hip””[MeSH Terms] OR ““hip””[All Fields]) AND “femoroacetabular”[All Fields] OR “impingement”[All Fields] OR (““arthroscopy””[MeSH Terms] OR ““arthroscopy””[All Fields]) AND (““hyaluronic acid””[MeSH Terms] OR (““hyaluronic””[All Fields] AND ““acid””[All Fields]) OR ““hyaluronic acid””[All Fields]) |
| 6 | (“hip”[MeSH Terms] OR “hip”[All Fields]) AND “femoroacetabular”[All Fields] OR “impingement”[All Fields] OR (“arthroscopy”[MeSH Terms] OR “arthroscopy”[All Fields]) AND autologous[All Fields] AND (“chondrocytes”[MeSH Terms] OR “chondrocytes”[All Fields] OR “chondrocyte”[All Fields]) AND (“embryo implantation”[MeSH Terms] OR (“embryo”[All Fields] AND “implantation”[All Fields]) OR “embryo implantation”[All Fields] OR “implantation”[All Fields]) |