
Abstract
Background:
The fascia has been demonstrated to represent a potential force transmitter intimately connected to the underlying skeletal muscle. Sports-related soft tissue strains may therefore result in damage to both structures.
Purpose:
To elucidate the prevalence of connective tissue lesions in muscle strain injury and their potential impact on return-to-play (RTP) duration.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
Imaging studies describing frequency, location, and extent of soft tissue lesions in lower limb muscle strain injuries were identified by 2 independent investigators. Weighted proportions (random effects) were pooled for the occurrence of (1) myofascial or fascial lesions, (2) myotendinous lesions, and (3) purely muscular lesions. Study quality was evaluated by means of an adapted Downs and Black checklist, which evaluates reporting, risk of bias, and external validity.
Results:
A total of 16 studies (fair to good methodological quality) were identified. Prevalence of strain injury on imaging studies was 32.1% (95% CI, 24.2%-40.4%) for myofascial lesions, 68.4% (95% CI, 59.6%-76.6%) for myotendinous lesions, and 12.7% (95% CI, 3.0%-27.7%) for isolated muscular lesions. Evidence regarding associations between fascial damage and RTP duration was mixed.
Conclusion:
Lesions of the collagenous connective tissue, namely the fascia and the tendinous junction, are highly prevalent in athletic muscle strain injuries. However, at present, their impact on RTP duration is unclear and requires further investigation.
Muscle strain injuries rank among the most common musculoskeletal health complaints in ball game sports. 5,21,28,31 Excessive tissue loading, particularly through eccentric contractions during athletic movements, has been suggested to represent the main pathomechanism of injury. 23 Therefore, from a mechanistic perspective, the muscle’s ability to actively and passively withstand elongating forces is paramount to prevent a structural trauma diagnosed as a strain.
Contrary to prior assumptions, the skeletal muscles and their tendons are not the only structures transmitting and bearing tensile loads. In some muscles, less than 20% of the fibers span the entire distance between the origin and insertion, while the remaining fibers end in the muscle belly, being connected only via their endomysium. 15 This architecture strongly suggests a force-transmitting or force-absorbing role of the intramuscular connective tissue. On a more macroscopic level, a close relationship between the connective tissue and the active component of the locomotor system exists; the surrounding fasciae of adjacent muscles fuse tightly with each other, creating continuity instead of separation. 43
Results from biomechanical experiments underline the mechanical significance of the structural linkage between muscular and connective tissue. Upon proximal lengthening of the rat extensor digitorum muscle, Huijing and Baan 16 measured considerable force differences of up to 25% between the proximal and the distal tendon. Removing the extensor digitorum’s fascial continuity to the surrounding muscles almost eliminated the force difference, which implies a force transmission through the extramuscular connective tissue. In view of the significant mutual interactions between both muscular and connective tissue, it has been speculated that one major function of myofascial continuity consists in assisting the muscle during the absorption of elongating forces. 43 This hypothesis is supported by data from Butler et al, 6 who revealed high similarities of fasciae and tendons regarding most investigated material parameters (eg, maximal stress tolerance).
Against the background described above, the structural damage occurring in clinically diagnosed muscle strain injuries may not be restricted to the muscle only. Tissue overstretch will also affect the fascia, potentially leading to ruptures within the connective tissue. However, to date, the question as to whether muscular strain injuries are associated with damage of the fascia has not been investigated in a systematic review. Therefore, the aim of the present study was to summarize the scientific literature on the prevalence of fascial lesions in muscle strain injuries and their possible association with return to play (RTP) duration).
Methods
Study Design
A systematic review with meta-analysis was performed between April and June 2018. It was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines 26 and followed the recommendations for ethical publishing of systematic reviews by Wager and Wiffen. 40 The study was registered in the PROSPERO database (CRD42018090392).
Search Strategy
Two independent investigators (J.W. and M.B.) performed the systematic literature searches. Potentially relevant articles published in English between 1970 and January 2019 were identified in the following online databases: PubMed (MEDLINE), Scopus, Web of Science, ScienceDirect, and Google Scholar. The search terms contained topic-related key words with Boolean operators (PubMed: (“muscle injury” OR “muscle strain”) AND (imaging OR MRI OR ultrasound) AND (location OR site)).
Eligibility Criteria
Criteria for study inclusion were (1) cross-sectional imaging study (magnet resonance imaging [MRI] or ultrasonography [US]) with or without a subsequent observation period during the RTP process, (2) enrollment of adults (≥18 years old) engaged in regular athletic sports performance, (3) patients diagnosed with lower extremity muscle strain injury with structural tissue damage, (4) report of the specific injury location (fascia/myofascial junction, myotendinous junction, muscle only; studies reporting injuries in one of the locations were included only if clearly indicating that no abnormalities were found in the other locations), and (5) peer-reviewed publication in the English language. As the main objective of the present study was the analysis of tissue-specific lesion prevalence, reporting of data relating to the RTP process (in most cases the time frame between diagnoses and RTP or competition in days) was considered a secondary (optional) outcome.
Study Selection
The pool of publications retrieved by the initial literature search was further analyzed as follows (Figure 1). After elimination of duplicates, the titles and abstracts of all papers were screened regarding the fulfillment of the inclusion criteria. Additionally, the reference lists of all eligible studies were checked for relevant articles pertaining to the research question. Disagreement regarding the fulfillment of the inclusion criteria between the 2 investigators, who independently screened the studies, was resolved by discussion between them.
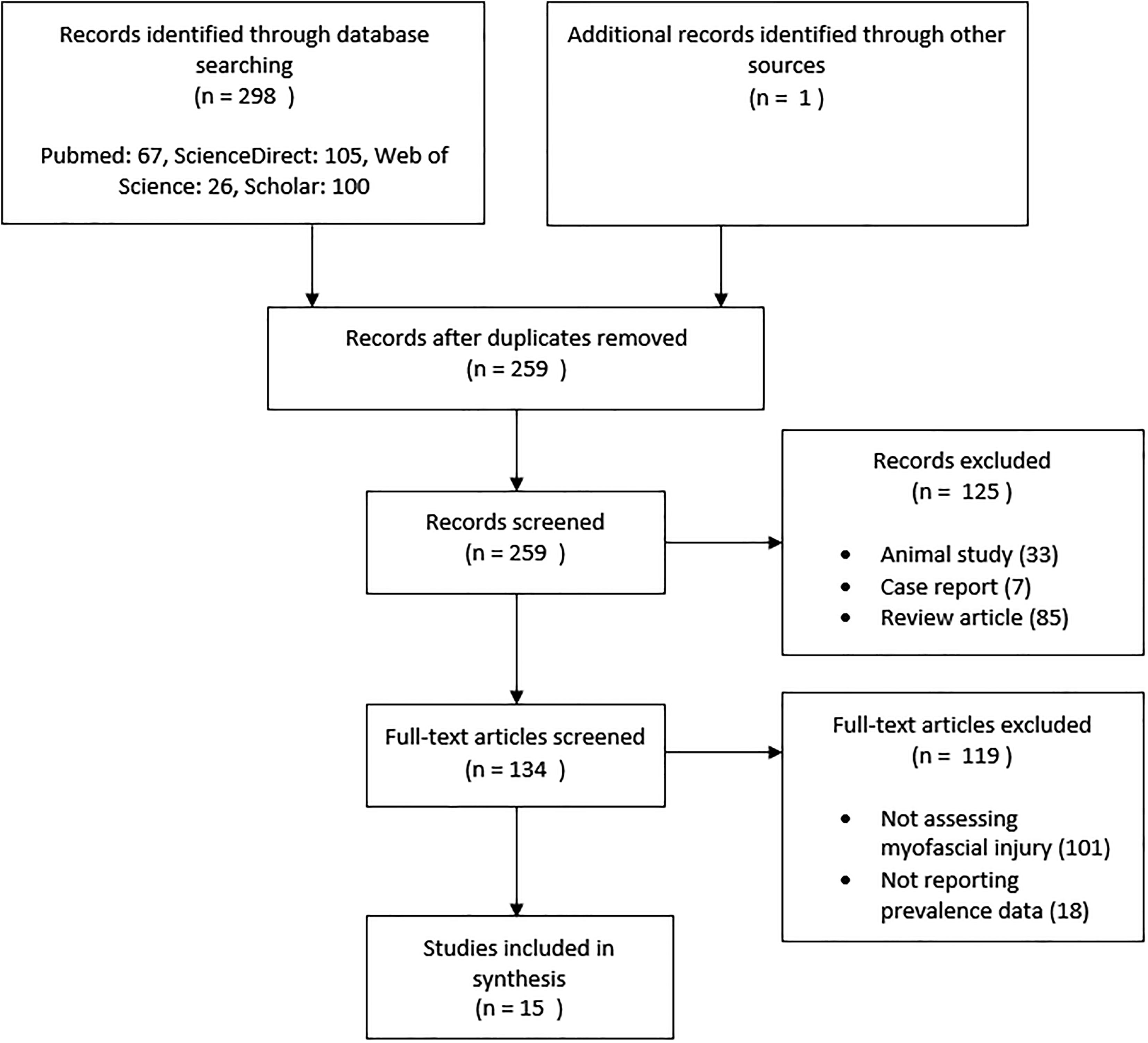
Overview of the study flow.
Data Extraction
The 2 investigators independently performed the data extraction using a standardized datasheet. The following variables were retrieved: mode of data collection and/or analysis (prospective or retrospective), setting (type of sport), sample size, demographic and anthropometric data (age, sex, weight, height, and body mass index), assessment method (US or MRI), injury location (affected joint or muscle), damaged tissue (muscle only, myotendinous junction, and/or myofascial junction and fascia), and size of the lesion (in millimeters).
Risk of Bias and Methodological Quality
An adapted version of the Downs and Black checklist 11 was used to evaluate the methodological quality of the included studies. The Downs and Black checklist has been proposed to be used in nonrandomized health care trials and exhibits good to excellent reliability (test-retest agreement, r = 0.88; interrater agreement, r = 0.75). 30 Our modified instrument included a total of 14 items grouped in 4 categories: reporting quality (5 items), risk of bias (5 items), external validity (3 items), and power (1 item). For each criterion met, 1 point was awarded and a sum score (maximum 14 points) was calculated. Power was rated as sufficient if an a priori sample size calculation was presented or if the achieved sample size was n > 73. This cutoff value was identified following the recommendations of Munn et al, 29 where n = z 2 p(1-p)/d 2 (z statistic for a 95% CI is 1.96, precision [d] of .05 and anticipated proportion [p] of 5%). All ratings were made by the 2 independent investigators, and disagreements were resolved by discussion and consensus between them.
Data Analysis
For all included studies, the prevalence (number) of lesions in the 3 locations was extracted. Myofascial lesions included structural damage to the soft tissue surrounding the muscle (deep fascia and epimysium) as well as to its junction to the muscle. This could also include muscular fibers directly inserting into the fascia. Myotendinous lesions comprised the group of tissue failures found in the muscle’s proximal or distal tendon, the paratenon, or the muscle fibers inserting into or near a tendon. Muscular lesions were documented if the site of injury was purely muscular and distant to muscle-related connective tissue such as the fascia, tendon, epimysium, or perimysium.
The obtained data were pooled by means of a random effects model, accounting for unobserved between-study heterogeneity: A Freeman-Tukey double arcsine transformation was used to compute weighted summary proportions, 3 which were reported including 95% CIs. Muscle-specific subgroup analyses were performed for lesions occurring in the fascia or myofascial tissue. Heterogeneity was tested by means of the I 2 test and Cochran Q test. Both the pooled and the individual studies’ proportions were displayed by means of forest plots. All calculations were made using StatsDirect, version 3.1.17.
Results
The study flow is depicted in Figure 1. The literature research returned 300 records. After we removed duplicates (n = 40) and excluded articles not pertaining to the research question (n = 244), 16 studies, collectively evaluating a total of 1503 muscle injuries (Table 1), were included. Reporting quality (mean, 3.6/5 points; range, 2-4 points) and external validity (mean, 3.2/5; range, 0.5-4.5) were moderate to good, and risk of bias (mean, 1.8/3; range, 1-3) was moderate (Table 2). It was noted that 5 of the 16 included studies (31.3%) presented adequate power. Significant heterogeneity was detected in all analyses (see below).
Overview of the Included Studies a

a Sample sizes were corrected for missing, incomplete, or imprecise data. F, female; M, male; MRI, magnetic resonance imaging; NR, not reported; P, prospective; R, retrospective; US, ultrasonography.
b Values are expressed as mean or mean ± SD.
c Delay between injury and diagnostic imaging. Values are expressed as means (if reported in the study) and ranges.
Methodological Quality of the Studies Included a
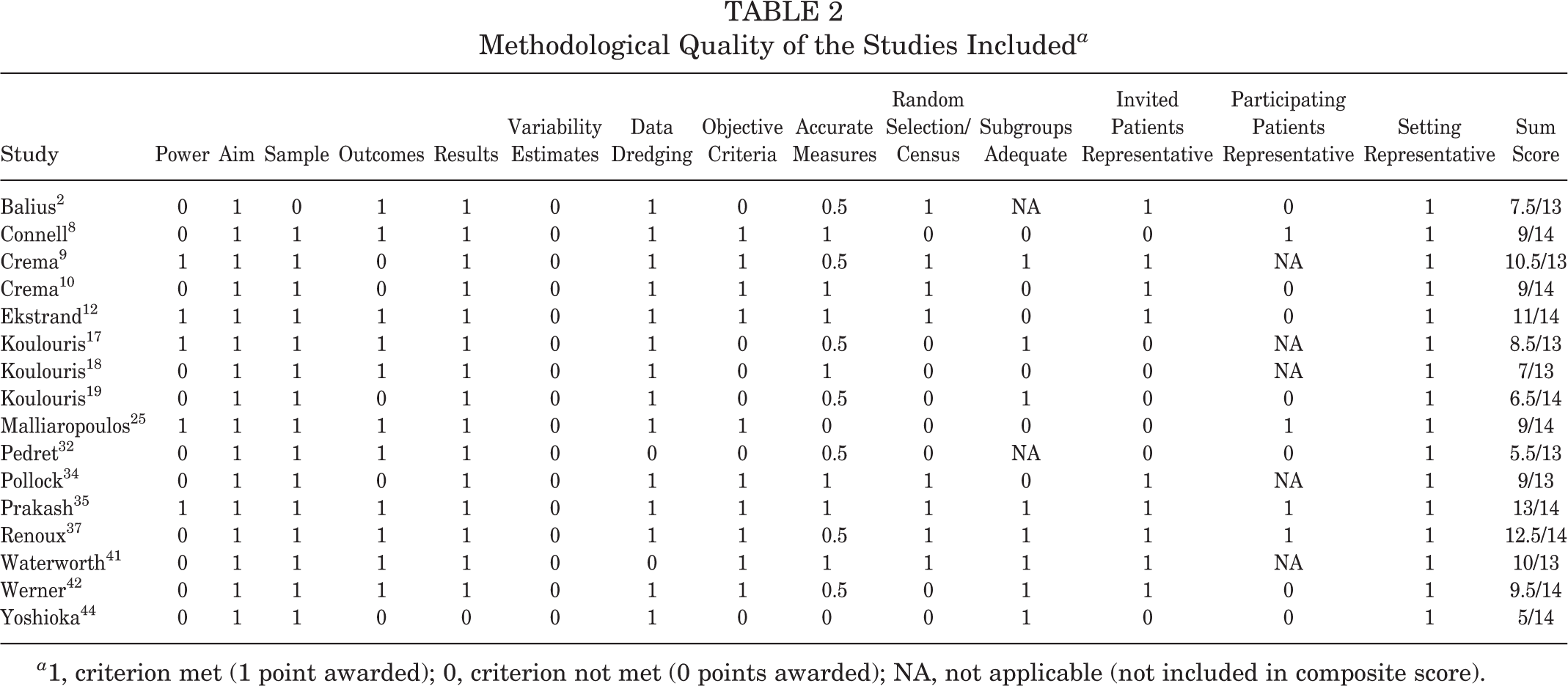
a 1, criterion met (1 point awarded); 0, criterion not met (0 points awarded); NA, not applicable (not included in composite score).
Prevalence of Fascial Injury
The majority of the studies reporting prevalence (14/15) collected MRI data, whereas 1 study 25 used US imaging only and 2 studies 8,17 performed both MRI and US screenings. The studies combining MRI and US did not clearly report the numbers of detected lesion types (myofascial, myotendinous, or muscular) stratified by imaging modality. The most frequently examined muscles were the hamstrings (n = 8 studies), followed by the soleus (n = 5 studies). The remaining 2 studies either reported data for the gastrocnemius or did not stratify the diverse lower leg muscles examined. Individual study findings are displayed in Table 3. The weighted summary proportions, obtained through random effects meta-analysis, revealed a myofascial lesion prevalence of 32.1% (95% CI, 24.2%-40.4%; I 2, 89.1%; Cochran Q, 128.7; P < .1) (Figure 2), whereas myotendinous or tendinous lesions were detected in 68.4% (95% CI, 59.6%-76.6%; I 2, 90.7; Cochran Q, 128.7; P < .1) (Figure 3) and muscular lesions in 12.7% (95% CI, 3.0%-27.7%; I 2, 95.3; Cochran Q, 106.8; P < .1) (Figure 4) of the cases. With regard to the subgroup of the myofascial tissue lesions, the prevalence varied between the different locations: damage was diagnosed more often in the soleus muscle (36.4%; 95% CI, 24.7%-48.8%; I 2, 74.9; Cochran Q, 15.9; P < .1) compared with the hamstrings (27.9%; 95% CI, 18.4%-38.6%; I 2, 89.9; Cochran Q, 69.3; P < .1).
Prevalence of Lesions by Type in the Included Studies a

a Values are expressed as numbers of lesions. Dashes indicate not determined or not investigated. BF, biceps femoris; CM, calf muscles; FHL, flexor hallucis longus; G, gastrocnemius; HS, hamstrings; NR, not reported; RF, rectus femoris; S, soleus; SM, semimembranosus; ST, semitendinosus; TP, tibialis posterior; VL, vastus lateralis.
b No clear differentiation between muscular, myofascial, and tendinous injuries.

Forest plot displaying the individual and pooled prevalences (random effects [RE] meta-analysis) of myofascial damage in muscle strain injury. Values displayed are mean proportions and 95% CIs.

Forest plot displaying the individual and pooled prevalences (random effects [RE] meta-analysis) of myotendinous damage in muscle strain injury. Values displayed are mean proportions and 95% CIs.

Forest plot displaying the individual and pooled prevalences (random effects [RE] meta-analysis) of isolated muscle damage in muscle strain injury. Values displayed are mean proportions and 95% CIs.
Fascial Injury and RTP
A total of 7 studies were identified that investigated the relationship of fascial injury and aspects of RTP (Table 4). 8,12,32,34,35,37,42 However, the applied statistical procedures and the objectives of the conducted analyses in the individual studies were too different to allow meta-analytic pooling of the results.
Associations Between Fascial Lesions and Aspects of Return to Play a

a CT, connective tissue; RTP, return to play.
b Pollock et al 34 found comparable values and no systematic difference between myofascial and myotendinous lesions.
We found 2 studies 35,42 that focused on the extent of the fascial lesion. Werner et al 42 compared the size of the lesion in players with short (<2 weeks) and long (>2 weeks) RTP duration. On average, the lesions were 3 times greater in the second subgroup, with prolonged injury-related downtime. Prakash et al 35 made similar findings, reporting longer RTP durations in patients with greater fascial damage. Injuries with clear connective tissue failure (grade 3) had a mean RTP duration of 48 days, while athletes with smaller lesions (grade 2) needed only 25 days of injury downtime.
We identified 4 studies 8,12,32,34 that compared the RTP duration of myofascial and myotendinous lesions. Connell et al 8 found an increased downtime in athletes with myofascial lesions, but the small difference of 1.2 days did not reach statistical significance. Pedret and colleagues 32 reported nonsignificant but higher values for defects with fascial contribution when compared with tissue failure at the myotendinous junction (35 vs 27 days). Slightly different observations were made by Ekstrand et al, 12 who similarly did not find a difference in RTP time between the respective injury types but registered lower values for myofascial lesions. Pollock et al 34 found comparable values and no systematic difference between myofascial and myotendinous lesions.
One study 37 compared RTP duration in muscular and general connective tissue (fascia and intramuscular connective tissue including tendon) lesions. According to the data reported, athlete downtime was significantly longer for connective tissue damage (7.6 weeks) than for muscle damage only (3.9 weeks).
Discussion
The present systematic review is the first study to summarize the evidence on the prevalence of fascial lesions in clinically diagnosed muscle strain injuries. In both sports practice and scientific research, it has been widely assumed that strains occurring in the soft tissue predominantly affect the skeletal muscles. 22 Our findings contradict this assumption; isolated muscular lesions were identified only in about 1 of 8 cases, and the damage was frequently located within or at the junction to the collagenous connective tissue. The term “muscle strain injury,” therefore, does not adequately reflect the morphological substrate of the condition and could be misleading during the diagnostic process. To avoid this, we suggest using more general terms (eg, “myocollagenous strain injury”) that may indicate more clearly the variety of potentially affected tissues.
The location with the highest damage prevalence was the myotendinous junction, which is plausible in view of its force-transmitting function during muscular contraction. However, as assumed in our hypothesis, the meta-analysis also demonstrated that a substantial share of injuries (almost one-third) affect the epimysium or fascia and its junctions to the muscle. It had already been speculated that the connectivity between the muscular structures (fibers, bundles) and the associated connective tissues (endomysium, epimysium, perimysium) may play a role in force transmission, distribution, and absorption. 43 The finding of frequent lesions in the extramuscular sheath during engagement in highly dynamic sports with sudden accelerations, decelerations, and changes of direction seems to morphologically support this assumption. Although the fascia basically exhibits a high strain tolerance and resistance to elongating forces, 6 except for its intrinsic properties, it does not have the capacity to quickly and actively react to high external forces. Owing to the presence of myofibroblasts, the mechanical properties of the fascia can be modulated via adjustment of their contraction level. However, unlike myocytes, fascial myofibroblasts can be activated only by the autonomous nerve system, and resulting stiffness becomes mechanically relevant only after days or weeks. 45 We hence hypothesize that the fascial connective tissue mechanically assists the muscle in taking up loads. Not having an effective active protection mechanism similar to muscle contraction, the fascia can be damaged if the external stresses are too high.
Although our findings impressively underline the vulnerability of the extramuscular connective tissue during athletic movement, it is still unclear whether fascial lesions cause longer RTP durations. The included studies investigating the association between fascial damage and athlete downtime yielded mixed results without indisputable evidence. Although a small trend toward longer RTP times in lesions with fascial damage may be concluded, future research is needed to substantiate this observation.
Current rehabilitation paradigms for muscle strain injury include a variety of methods, particularly eccentric training and neuromotor control exercise. 14 Even if future studies do not verify longer athlete downtimes due to fascial lesions, treatments specifically tailored to account for the affected tissues in different subgroups (purely muscular vs mainly collagenous lesions) could still lead to accelerated recovery. For the connective tissue, besides eccentric exercise, this may include dynamic stretching (possibly at a higher dosage than before) or nutritional supplementation. A recent study found that the intake of vitamin C–enriched gelatin combined with rope skipping exercise substantially improved collagen synthesis, 38 which would be expected to be paramount for the healing process of connective tissue.
Another issue relates to pain perception and muscle function. Findings from experimental studies suggest that fascial tissue exhibits a higher pain sensitivity than the muscle, which could explain potential delays in RTP time. For example, delayed-onset muscle soreness (DOMS), which also occurs particularly after eccentric loading, has been demonstrated to stem from the fascia rather than from the muscle itself. Under ultrasound control, different researchers used small needles to selectively apply noxious stimuli to both structures. Interestingly, the pain response was significantly stronger when the fascia was irritated, regardless of whether the stimulation was electrical 20 or biochemical. 13 So far, it has been assumed that DOMS is mainly associated with activity of afferents within the muscle 30 that are able to change the excitability of motoneurons at the spinal and/or cortical level. 1 These neural adjustments are thought to decrease the voluntary drive to muscles, resulting in a reduced capacity for maximal voluntary force production. 4,36 In view of the algogenic potential of the fascia, besides its sensory consequences (pain impairing engagement in activity), it seems plausible that an altered afferent feedback from the fascia (eg, from free and encapsulated nerve endings) contributes to the reduced neural drive. If similar processes (increased nociceptive input from the connective tissue) occur in muscle injuries with fascial lesions, this would open new frontiers for therapeutic treatments.
Despite the seemingly high prevalence of fascial defects in muscle injury and the potential benefits of specifically diagnosing and treating them, our meta-analysis showed major heterogeneity, which can be expected to a certain extent in prevalence trials. This finding may be explained by a plethora of factors. The foremost factor is that the frequency of injuries varied between the investigated muscles (ie, hamstrings vs soleus), and the muscle-specific subgroup analyses at least slightly reduced the statistical inconsistency. Clinicians may therefore be aware that some anatomic locations (eg, the soleus muscle) merit a focused investigation of the deep fascia. The frequent inclusion of the soleus and the high prevalence of fascial lesions in this muscle are surprising findings. With its biarticularity, the gastrocnemius is often expected to be a prime candidate for injury, and the soleus has only rarely been examined so far. 2 Future research should further delineate both fascial anatomy of the calf and the prevalence of injury to the soleus muscle.
Besides these content-related aspects, statistical heterogeneity may also be explained, in part, by shortcomings of the individual trials and our analysis. Several systems for the classification of muscle strain injuries have been proposed during recent years, 7,24,27,33,39 and the studies included in our review used varying approaches. This limitation highlights the need to establish clear and uniform criteria for classification, which will help to reduce heterogeneity between future studies. At least some of the available systems 7,27 recommend the separate assessment of (myo)fascial lesions as an independent category. Our data, pointing toward a considerably high prevalence of fascial damage, support this approach. Another issue relates to imaging modality. The vast majority of the studies describing prevalence used MRI to diagnose injury. However, our analysis also includes data from 1 US study and 2 studies that used both US and MRI. Unfortunately, the latter did not delineate how often the respective lesion types (eg, myofascial damage) were detected with the 2 imaging methods. If present, differences in sensitivity to detect structural trauma of the soft tissue may have affected the result to a small degree. Finally, some caution may be necessary when generalizing our findings: 4 of the included studies examined Australian Football players. Although the majority of the others (9 studies) enrolled athletes from diverse sports (eg, football, running, tennis), this could have introduced a small bias.
Perspective
The findings of our review have clinical implications for sports physicians, physical therapists, and exercise professionals. Based on a precise diagnosis, athletes with muscle injury and associated connective tissue lesions should be treated with specifically tailored methods (eg, oral supplementation of collagen peptides or high-velocity dynamic stretching) to quickly restore the load-bearing function of the collagen.
Conclusion
Lesions of the collagenous connective tissue are a frequent finding in muscle strain injuries diagnosed through use of imaging methods. However, because of the high heterogeneity of the included studies and the mixed evidence concerning the impact of fascial lesions on RTP duration, further research is warranted in order to (1) conclusively elucidate the role of fascial damage within sports rehabilitation and (2) develop specific treatment approaches.
Footnotes
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.