
Abstract

Keywords
The medial patellofemoral ligament (MPFL) is the main soft tissue restraint of the medial patellar stabilizers. 2 Patellar dislocation usually leads to this ligament being torn or to osteochondral injury. 2,3,14,16 A range of tendon grafts have been used for MPFL reconstruction 1,4,6,7,11 –15 ; however, reports of patellar dislocation combined with a large, displaced vertical patellar fracture are sparse in the literature. 16 Small marginal patellar fractures are common with acute patellar dislocations. We present a rare case of an acute patellar fracture combined with patellar dislocation in a 19-year-old girl. Our case is unique because it is not a “typical” marginal patellar fracture but rather a large, displaced vertical patellar fracture requiring reduction and internal fixation. Owing to a history of preexisting recurrent patellar dislocation combined with the presence of trochlea dysplasia, MPFL reconstruction was required. The patient was successfully treated with MPFL reconstruction and patellar fracture fixation using two 4.0-mm cannulated screws plus sutures. Such a case has not been described previously in the literature.
Case Report
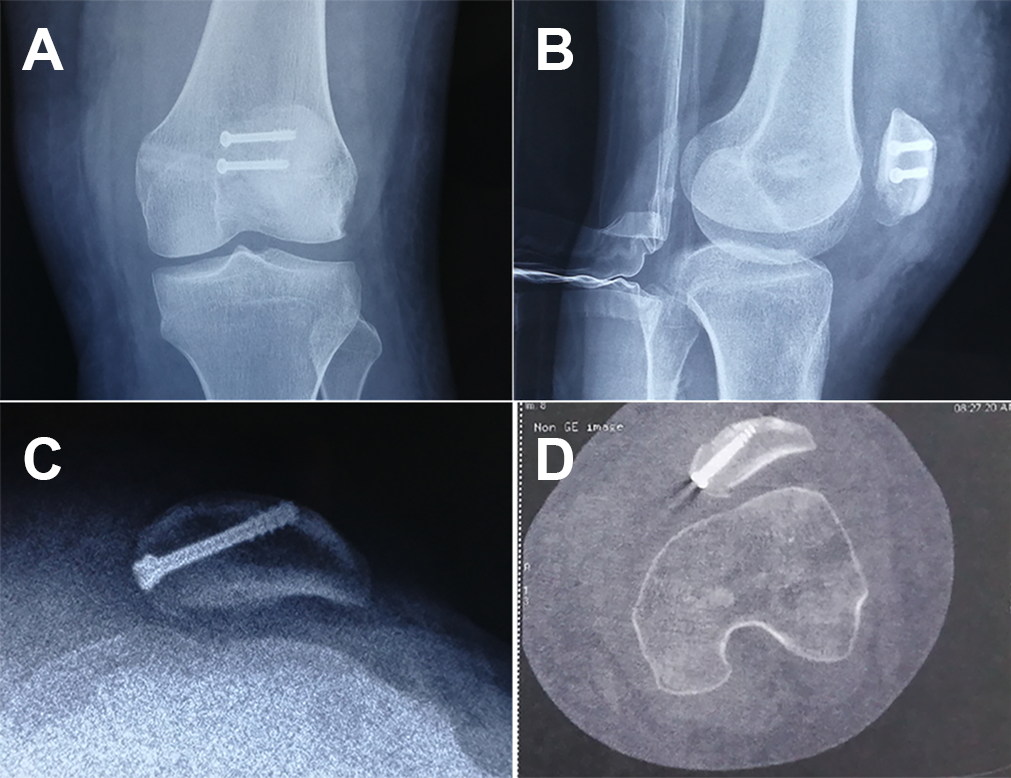
A 19-year-old girl presented to an emergency department with pain and swelling of the right knee after a jump during a table tennis match. Physical examination revealed swelling in the knee, pain upon palpation, and limited knee motion. Plain radiographs and computed tomography (CT) scans were obtained from the emergency department that confirmed the diagnosis of patellar subluxation with a vertical fracture involving the medial third of the patella (Figure 1). Her medical history revealed symptoms of recurrent patellar instability (patellar dislocation >2 times before this injury), and now she was diagnosed with the same in the outpatient department. Surgical treatment was recommended to her prior to this patella fracture and patella dislocation, but she refused since she was preparing for an important entrance examination. The tibial tubercle–trochlear groove distance (TT-TG) was 16 mm. The patient was subsequently taken to the operating room for patellar reduction and internal fixation combined with MPFL reconstruction. Consent for publication was obtained from the patient. The study was also approved by the local ethics committee (2017-114-2).

Vertical fractures on the anterior-posterior (A, B) radiographs and (C, D) CT images of the patella. (C) Trochlear dysplasia on the axial view of the CT scan. CT, computed tomography.
Surgical Technique
The surgical technique involved patellar fracture fixation and reconstruction of the MPFL at the medial border of the patella (Figure 2).

A schematic diagram of the patellar fracture fixation and reconstruction of the medial patellofemoral ligament.
For patellar reduction and internal fixation, a 6- to 8-cm medial parapatellar incision was used to expose the medial face of the patella. Then, the fracture surface was carefully cleaned. The fracture was anatomically reduced and then held firmly with large towel clips, with special attention to restoring a smooth articular surface; to fix the vertical fracture, two 4-mm cannulated screws (Synthes USA) were passed transversely from the medial side to the lateral side through each fragment (Figure 3A). A lateral retinacular release was performed on this patient with tight lateral structures using a banana knife.

(A) Two cannulated screws were passed transversely to fix the medial vertical fracture of the patella. (B, C) Then, No. 2 FiberWire sutures were passed through the 2 cannulated screws. (D) The central portion of the autograft was then fixed on the medial patella with the sutures.
MPFL Reconstruction
We performed the MPFL reconstruction after patellar reduction and internal fixation. For this, 4-mm partially threaded cannulated screws (Synthes USA) were used instead of bone tunnels (Figure 3, B and C). The superomedial edge of the patella was exposed using a nucleus pulposus forceps. The MPFL for this patient was reconstructed with a semitendinosus tendon fixed with sutures. Using a 2-cm incision at the pes anserinus, the semitendinosus tendon was freed and harvested with a tendon stripper. Then, two No. 2 FiberWire sutures (Arthrex) were passed through the 2 cannulated screws. The reconstructed ligament was then fixed with the 2 sutures that passed through the 2 cannulated screws (Figure 3D).
Next, augmentation was achieved with No. 2 nonabsorbable sutures with the overlying patellar fascia. A 2- to 3-cm incision was made over the medial femoral epicondyle; the femoral insertion site was then identified under fluoroscopy as described by Schöttle et al 12 on a true lateral knee view. Graft tension was evaluated through the arc of motion. If a single measurement discrepancy for the length change pattern of the graft was <3 mm, the measurement was considered isometric. 8 The femoral tunnel was overreamed with a reamer equal to the diameter of the semitendinosus graft (7 mm) with a depth of approximately 40 mm. The reconstructed MPFL was then passed into the femoral tunnel via the eyelet-passing pin. Next, the 2 free ends were fixed with a 7 × 20–mm bioabsorbable interference screw (Milagro, DePuy Mitek) with the knee at 30° of flexion. A flexion test was performed intraoperatively to determine the stability of the fracture and the correct tension of the patella, and then the capsular tears were repaired with multiple interrupted sutures.
Postoperative radiographs (Figure 4, A and B) and the axial cut of the CT image (Figure 4C) were obtained at follow-up.
(A-C) Postoperative radiographs and (D) axial cut on computed tomography obtained at follow-up that demonstrated proper position of the patella with anatomic reduction fixed with cannulated screws.
Postoperative Care
The knee was placed in extension in a hinged knee brace, and the patient was allowed to be weightbearing as tolerated in the first 2 weeks after surgery. Leg raising exercises as well as quadriceps muscle training were encouraged postoperatively with crutch support. Active range of motion exercises of the knee were permitted, with an allowed range of 0° to 30° of motion from 2 to 4 weeks postoperatively, 0° to 60° from 4 to 6 weeks postoperatively, and 0° to 90° from 6 to 8 weeks postoperatively. After 8 weeks postoperatively, full range of motion was permitted as tolerated. Controlled sports activities (such as jogging and swimming) were performed after 3 months postoperatively, when full quadriceps strength had returned. Fifteen months after the operation, the patient was able to participate in sports activities without pain or recurrent patellar instability.
Discussion
The main finding of the present case report was that patellar stability of the knee was restored with our surgical procedure. After fracture fixation and MPFL reconstruction, the patient returned to sports without any episodes of recurrent dislocation or subluxation and no pain at the most recent follow-up. Patellar dislocation usually leads to a torn MPFL and/or an osteochondral injury. 5,9,10,14,16 Different methods have been described for surgical treatment of patellar osteochondral fractures. Sutures or screws have been the common mode of fixation for fractures, whereas MPFL repair or reconstruction has become a good procedure for restoring patellar stability. 1,4,6,7,10 –15 Most techniques for patellar fixation during MPFL reconstruction use patellar bone tunnels, 1 interference screws, 4 soft tissue sutures, 13 or suture anchor fixation. 15 In the present case, the patellar instability was associated with a large medial vertical patellar fracture. Traditional patellar bone tunnels, interference screws, soft tissue sutures, or suture anchor fixation may have been unsuitable for this case.
The case presented here illustrates an instance of chronic patellar instability in a patient sustaining a medial vertical patellar fracture. In this patient, we used a novel technique for fracture fixation simultaneously with MPFL reconstruction. This technique provided secure fixation for medial patellar fracture and MPFL reconstruction. Two cannulated screws were passed transversely from the medial side to the lateral side through each fragment to fix the medial vertical patellar fracture. The 4.0-mm partially threaded cannulated screws were used instead of bone tunnels for MPFL reconstruction. To the best of our knowledge, there have been no published reports of a similar treatment method in the English literature. This case adds a rare occurrence to the literature. At the 12-month follow-up, our patient had favorable results, and the patient had returned to sports with no pain and no instability.
Examples of patellar dislocation combined with osteochondral injury have been described by several authors. 5,9,10,14,16 Sillanpää et al 14 described MPFL injury characteristics at the patellar attachment. They recommended osteochondral repair for patellar MPFL avulsions that include an osteochondral fracture. Toritsuka et al 16 reported a study of 7 patients who sustained medial marginal fractures of the patella after patellar dislocation. In that study, after the small fracture fragment was removed, the MPFL was repaired by reattachment to the patella with anchors. However, in our case, the fracture was relatively larger, and the anchors may have been unsuitable for fracture fixation.
The technique that is described in this study has several limitations. First, researchers may worry that this technique may influence the bone-tendon healing of the graft at the patella because the graft was attached to the screw head. To solve this potential problem, in the future, patients can be treated with headless compression screws for this type of injury. Second, this technique is unsuitable for fixation of relatively smaller patellar fractures.
Conclusion
This novel technique for fracture fixation and MPFL reconstruction was successfully used for treating a rare case of a large vertical patellar fracture combined with recurrent patellar dislocation.
Footnotes
The author declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.