
Abstract
Background:
The optimal surgical treatment of anterior shoulder instability remains controversial.
Hypothesis:
(1) Implants and facility-related costs are the primary drivers of variation in direct costs between arthroscopic Bankart and Latarjet procedures, and (2) distal tibial allograft (DTA) is more costly than Latarjet as a function of the graft expense.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Intraoperative cost data were derived for all arthroscopic anterior stabilizations and Latarjet and DTA procedures performed at a single academic institution from January 2012 to September 2017. Cost comparisons were made between those undergoing arthroscopic stabilization and Latarjet and between Latarjet and DTA. Multivariate regressions were performed to determine the difference in direct costs accounting for various patient- and surgery-related factors.
Results:
A total of 87 arthroscopic stabilizations, 44 Latarjet procedures, and 5 DTA procedures were performed during the study period. Arthroscopic Bankart repair was found to be 17% more costly than Latarjet, with suture anchor implant cost being the primary driver of cost. DTA was 2.9-fold more costly than Latarjet, with greater costs across all domains. Multivariate analysis also found the number of prior arthroscopic procedures performed (P = .007) and whether the procedure was performed in an ambulatory or inpatient setting (P < .0001) to be significantly associated with higher direct costs.
Conclusion:
Latarjet is less costly than arthroscopic Bankart repair, largely because of implant cost. Value-driven strategies to narrow the cost differential could focus on performing these procedures in an outpatient setting in addition to reducing overall implant cost for arthroscopic procedures. Perceived potential benefits of DTA over Latarjet may be outweighed by higher costs.
Because of the high risk for recurrence, 7 the optimal surgical treatment of anterior traumatic glenohumeral instability remains controversial, with advocates for arthroscopic labral repair and open Latarjet. Balg and Boileau 1 developed an Instability Severity Index Score based on the presence or absence of important risk factors for recurrence: age <20 years, participation in competitive contact sports, hyperlaxity, and bone loss. Patients scoring 6 of 10 possible points were found to recur at a rate of 70% with arthroscopic Bankart repair, suggesting stabilization with Latarjet as the preferred procedure. Subsequent published cohort studies of arthroscopic Bankart repair failure suggest that this threshold can be as low as 4 points to prevent recurrence. Although bone loss is considered, it is possible for the system to indicate Latarjet in the younger competitive athlete with hyperlaxity (external rotation >85°) 1,2 and minimal to no bone loss. 6,19 Despite higher reported complication rates with the Latarjet procedure, 4 some may advocate for its use in the primary setting for a young competitive collision-sport athlete with hyperlaxity. Thus, clinical controversy remains regarding the preferred method of surgical treatment for primary or recurrent instability in a high-risk population.
With the advent of bundled payments, there is a growing body of literature analyzing the health care expenditures of common arthroscopic procedures. 5,8,13,15,23 Specifically, many recent studies have focused on the patient-related and surgical factors that drive health care expenditures in common arthroscopic procedures. 5,8,13,15,23 The few published studies on anterior instability to date have leveraged billing charges and modeling methods in the performance of cost studies. Crall et al 10 performed a cost-effectiveness analysis of arthroscopic Bankart repair versus nonoperative treatment using a mathematical Markov model, where variables change over time based on preselected health states that describe how patients with shoulder dislocations may be treated. For example, a patient with a dislocated shoulder can be treated operatively or nonoperatively and can go on to several subsequent health states. In the nonoperative group, the patient could experience successful treatment or recurrence, leading to surgery or additional therapy. Patients treated operatively could achieve successful stabilization, postoperative stiffness requiring additional therapy, infection requiring antibiotics or additional surgery, and recurrence requiring additional surgery or therapy. Based on known probabilities, the model cycles patients through all possible health states, and costs are compared. 10,16 –18
Crall et al 10 found arthroscopic Bankart repair to be cost-effective in men younger than 25 years, in women younger than 15 years, and in all patients with more than 1 recurrence regardless of age. Using the cost data established by Crall et al, Makhni et al 16 in 2016 performed an expected value decision analysis comparing revision arthroscopic Bankart repair and open Latarjet and found that Latarjet was more effective (43.78 vs 36.76 quality-adjusted life-years) and less costly ($13,672 vs $15,287) in patients without a humeral avulsion of the glenohumeral ligament (HAGL) or bone loss. Finally, Min et al 17 performed a cost-utility study comparing arthroscopic Bankart repair and open Latarjet and found both procedures to be very cost-effective, but the Bankart procedure was found to be superior because patients with failed Latarjet had worse health states than those with failed Bankart repairs. All of these analyses used charges and not costs, which obscure interpatient variation and examine this situation from the perspective of an insurer and not a provider.
The current study used a novel tool that allows the determination of direct intra- and perioperative costs. 8,13,14,23 Our purpose was to determine the direct cost of surgical techniques used for recurrent anterior instability while accounting for patient and surgical variables that drive cost and cost variation. Arthroscopic anterior stabilization, open Latarjet, and open anterior glenoid bone grafting with distal tibial allograft (DTA) were directly compared regarding direct costs and factors affecting costs.
Methods
This was a retrospective case-control study. After appropriate institutional review board exemption was granted, all cases of arthroscopic anterior stabilization, open Latarjet, and open anterior glenoid bone grafting with DTA were reviewed as performed by 6 fellowship-trained surgeons from January 2012 to September 2017 at a single academic institution. Patients treated in ambulatory and inpatient settings were included. Patients were identified from financial billing data through Current Procedural Terminology (CPT) codes 23460, 23462, and 29806, associated with DTA, open Latarjet, and arthroscopic anterior labral repair, respectively. The following data were then collected via chart review: patient demographics, body mass index (BMI), tobacco use, American Society of Anesthesiologists (ASA) score, participation in contact or collision sports, direction of instability, prior open or arthroscopic stabilization procedures, procedure performed, treating surgeon, inpatient versus ambulatory setting, whether the patient was admitted postoperatively, whether the patient underwent perioperative regional blockade or indwelling catheter anesthesia, patient positioning, and total number of anchors used. Specific factors examined in Latarjet and DTA included the number of screws used and the number of anchors used.
Three patient cohorts were identified: arthroscopic anterior Bankart repair, Latarjet, and DTA. Only patients undergoing an isolated Bankart repair were included in the arthroscopic repair cohort, and all those undergoing concomitant rotator cuff repair, HAGL repair, superior labrum anterior and posterior (SLAP) repair, posterior labral repair, remplissage, and biceps tenodesis were excluded. Patients in the Latarjet and DTA groups were then randomly matched in a 2:1 ratio with patients in the arthroscopic stabilization group. Surgical decision making regarding which procedure to perform in a given scenario was left to the surgeon. In general, however, there were common indications. Arthroscopic repair was considered first-line treatment for recurrent anterior dislocations in collision/contact athletes with soft tissue or bony Bankart lesions in the absence of critical bone loss as determined by the attending surgeon. No uniform definition of bone loss was used but rather was left to the discretion of the attending surgeon. Patients were examined, and additional considerations were made according to their presumed risk of experiencing a recurrence. Those presenting with recurrent instability and critical bone loss were indicated for Latarjet or DTA. Those with a history of failed surgical stabilization were treated in an arthroscopic or open fashion at the discretion of the attending surgeon, largely on the basis of the presence of bone loss.
The value-driven outcomes tool is a comprehensive source of data from which the direct costs related to patient care encounters can be identified. 14 Direct patient-related and procedure-related costs from the surgical encounter were captured and included in this cost analysis. The value-driven outcomes tool creates an estimate of direct costs for operating room (OR)/facility utilization based on operative time, whereas non-OR/facility utilization costs are estimated from preoperative holding area and postanesthesia care unit (PACU) time as logged in the electronic medical record. The tool assigns a variable percentage of facility overhead costs on a per-minute basis, based on individual patient utilization. Many cost figures contributing to facility overhead are captured in this process, including equipment cost, nursing and staff salaries, utility costs, and equipment and facility maintenance costs. Costs assigned to the encounter vary by time and are tailored in ways not captured by flat facility charges. Thus, longer or more technical procedures are assigned higher costs. Similarly, medical complexity will drive cost variation in the non-OR/facility utilization and pharmacy cost groups, as a patient with hypertension may require longer preoperative or PACU stays to treat procedure-related hypertension.
The tool provides specific costs for medical devices and surgical implants, medications, diagnostic laboratory tests, and radiologic imaging. Variables examined from the value-driven outcomes database included total direct cost of the case, OR/facility utilization cost, non-OR/facility utilization cost, OR supplies implant cost (which includes cost of surgical implants and other related consumable supplies), non-OR supplies implant cost (including consumables used preoperatively and in the PACU), laboratory cost, pharmacy cost, other services cost, and imaging costs. These cost data are supplied via the Personal Consumption Expenditures Price Index for health care and were calculated in 2017 US dollars for this study.
The actual dollar amounts are confidential, as they are a result of cost negotiations between the hospital system and implant suppliers and cannot be presented in the actual dollar amount in any form to include mean or range of costs outside of the university. Therefore, these costs are normalized by cost category in the following way: a value of 0 is assigned to the minimum reported cost, and a value of 1 is assigned to the maximum reported cost. Normalization in this fashion facilitates publication for research while still reporting actual cost data. The strength of the tool lies in the direct cost data, as it does not reflect billing charges and thus escapes variation in insurance reimbursement, billing, and coding errors. 8 This tool has been validated, and its use has been reported in the orthopaedic literature. 8,13,14,23
Statistical Analysis
Descriptive statistics, including counts and percentages or means and standard deviations, were employed to describe clinical, demographic, and surgical characteristics of the patient cohort. Demographic, clinical, and surgical characteristics were compared between patients who received arthroscopic instability repair and Latarjet procedures, with the Student t test for continuous variables and chi-square tests for categorical variables. Outcome variables, including total direct cost and stratified cost as a function of cost types, were also compared between the study cohorts with a t test.
A multivariate regression analysis was performed to examine the effect of performing either arthroscopic instability repair or Latarjet procedures on the total direct cost, controlling for potential confounders: performing provider, ASA score, perioperative neuromonitoring, year when procedure was performed, approach of the surgery (open, arthroscopic, both), location where surgery was performed, number of prior arthroscopic instability procedures, and number of anchors and screws used. A generalized linear model with a log link and Gaussian/Poisson variance function was fitted to account for a skewed distribution with a heavy right-hand tail for the outcome variable. Statistical significance of the multivariate analysis was set at P ≤ .05.
Results
Demographics
Our study included 44 Latarjet procedures, 87 arthroscopic anterior Bankart repairs, and 5 DTA procedures (Figure 1). Manual chart review identified and excluded patients as outlined in Figure 1. For CPT 23462 (Latarjet), 48 results were identified, and 4 patients were excluded for concomitant procedures. For CPT 23460 (capsulorrhaphy anterior with bone block), 7 results were identified, and 2 patients were excluded because they underwent a posterior bone block procedure. A search was performed for patients undergoing CPT 29806 (arthroscopic capsulorrhaphy), and 90 patients remained after those who underwent concomitant surgical procedures were excluded. Of these 90 patients, 3 were excluded owing to missing cost data (2 patients) or having the procedure performed at an off-site surgical facility for which cost data were not reliably available. The remaining 87 eligible isolated arthroscopic anterior Bankart repairs were used as a comparison group with the Latarjet cohort.

Patient exclusion process: 4 patients were excluded from the Latarjet group (2 had concomitant open reduction internal fixation, 2 had incomplete medical records); 3 patients were excluded from the arthroscopic Bankart group (2 had no cost data, 1 was treated at an outside facility); and 2 patients were excluded from the distal tibial allograft (DTA) group (2 posterior bone blocks).
Descriptive statistics identifying the number and percentage of patient demographics across all cohorts are highlighted in Table 1. Age and BMI were similar across the arthroscopic and Latarjet cohorts, while the DTA group was older (mean ± SD, 37.2 ± 8.7 years) than the arthroscopic repair (23.8 ± 8.1 years) and Latarjet (26.3 ± 6.6 years) groups. The arthroscopic Bankart repair (74.7%) and Latarjet (79.6%) groups were largely male, and all patients undergoing a DTA procedure were male. Tobacco use ranged from 16.1% to 40.0% in the cohorts. Nearly one-fourth of the Latarjet cohort participated in contact or collision sports, in contrast to over half the arthroscopic cohort. No patients in the DTA cohort currently participated in contact or collision activities.
Descriptive Statistics for Patient Demographics and Clinical Characteristics a

a Data are reported as mean ± SD or n (%). ASA, American Society of Anesthesiologists; BMI, body mass index; DTA, distal tibial allograft.
The rates of prior surgical stabilization differed in the treated groups (Table 2). Of patients who underwent Latarjet, 56.8% (25 of 44) had undergone at least 1 prior arthroscopic Bankart, with 29.6% (13 of 44) having had 2 or more; 9.1% (4 of 44) had undergone a prior open Bankart procedure. In contrast, in the matched arthroscopic repair cohort, 5.8% (5 of 87) had undergone a prior arthroscopic stabilization, and 2.3% (2 of 87) had undergone a prior open Bankart procedure. Of those treated with DTA, 40% (2 of 5) had undergone a prior arthroscopic stabilization, and 40% (2 of 5) had undergone a prior open bone block procedure.
Rates of Prior Open and Arthroscopic Procedures a
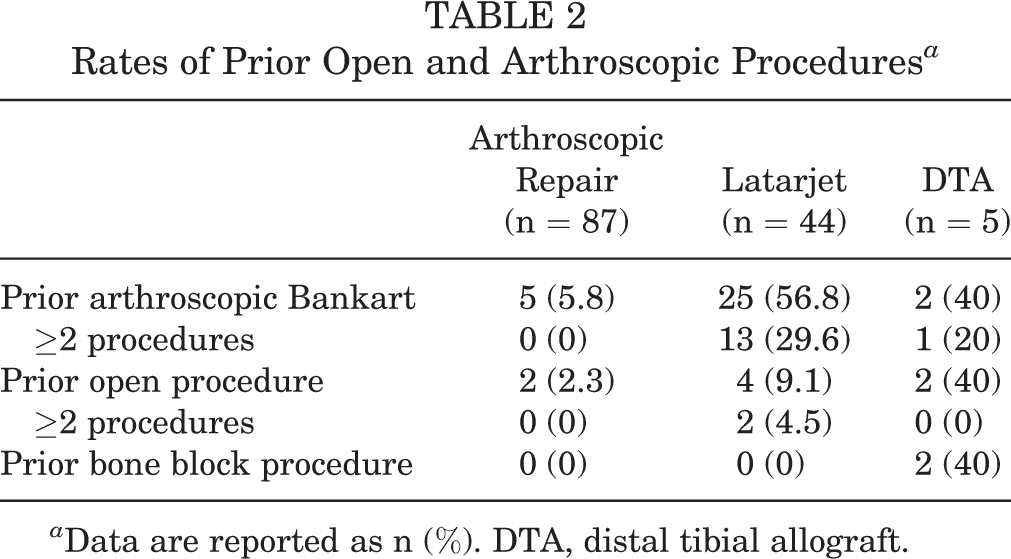
a Data are reported as n (%). DTA, distal tibial allograft.
Surgical Factors
Three surgeons (R.T.B., R.Z.T., P.E.G.) performed the bulk of the studied procedures (Table 3). Surgical treatment was overwhelmingly performed in an outpatient facility. Overall, 98.9% of arthroscopic repairs and 77.3% of Latarjet procedures were done in the ambulatory setting. No patients treated arthroscopically were admitted postoperatively, as opposed to 1 of the 44 patients (2.3%) treated with Latarjet and 2 of the 5 patients (40%) treated with DTA. Each of these 3 patients who were admitted postoperatively had undergone their surgical procedure in an inpatient hospital setting. No patient undergoing surgical treatment in the ambulatory setting was admitted postoperatively. Treatment with DTA was divided more evenly, with 3 of 5 performed in an inpatient facility and 2 of 5 in an outpatient facility. All groups had high rates of perioperative regional anesthesia, with either single-shot interscalene blocks or placement of interscalene catheters. A small subset of patients in the Latarjet and DTA cohorts underwent intraoperative neuromonitoring. Surgical procedures with intraoperative neuromonitoring were uniformly performed in the inpatient facility.
Surgeon and Perioperative Factors a

a Data are reported as n (%). DTA, distal tibial allograft.
Several significant differences between the Latarjet group and its matched arthroscopic cohort were discovered in univariate analysis: performing provider, ASA score, perioperative neuromonitoring, year when procedure was performed, approach of the surgery (open, arthroscopic, both), location where surgery was performed, number of prior arthroscopic instability procedures, and number of anchors and screws used. Age, sex, BMI, tobacco use, rates of postoperative admission, and rates of perioperative regional anesthesia did not differ significantly between groups (Table 4).
Demographic Comparison Between Latarjet and Arthroscopic Bankart Cohort a

a Data are reported as n (%). Age, sex, body mass index, tobacco use, rates of postoperative admission, and rates of perioperative regional anesthesia did not differ significantly among groups. ASA, American Society of Anesthesiologists.
b Each P value demonstrates a statistically significant difference between the Latarjet and arthroscopic repair groups (P ≤ .05).
Cost Analysis
In the univariate analysis, the strongest driver of cost variance was implant-related costs (OR supplies and implant cost), as arthroscopic Bankart repair was less costly in all other cost domains: OR/facility utilization, non-OR/facility utilization, laboratory, pharmacy, imaging, and other services (Figure 2). In this univariate analysis, total direct cost was not significantly different. DTA was 2.9-fold more costly than Latarjet. This cost difference was seen across most cost domains: total direct cost of the case, OR/facility utilization cost indicating longer OR times, non-OR/facility utilization cost indicating greater amounts of pre- and postoperative care, OR supplies implant cost to include the allograft, and other services cost.

Normalized costs by procedure. Values are presented as mean ± SD. *Latarjet vs arthroscopic Bankart, P ≤ .05. **Latarjet vs DTA, P ≤ .05. DTA, distal tibial allograft; OR, operating room.
Although total direct cost was not significantly different in a univariate analysis, the difference between the arthroscopic Bankart procedure and Latarjet in multivariate analysis became statistically significant after controlling potential covariates. Our multivariate analysis indicated that direct costs were 17% higher for the arthroscopic Bankart procedure as compared with the Latarjet. Multivariate analysis found that, in addition to which procedure was performed (Latarjet vs arthroscopic repair) (P = .025), outpatient vs inpatient surgical setting (P < .0001) and prior arthroscopic instability surgery (P = .007) were significant predictors of cost. Surgical stabilization performed in the inpatient hospital versus an outpatient surgical facility resulted in 47% higher costs. Patients who had previously undergone 2 or more prior arthroscopic stabilizations had 25% higher costs. Multivariate analysis noted no significant difference in cost between groups based on age, sex, BMI, ASA, performing surgeon, perioperative regional block, or the year performed (Table 5).
Multivariate Cost Analysis: Factors Associated With Direct Cost a
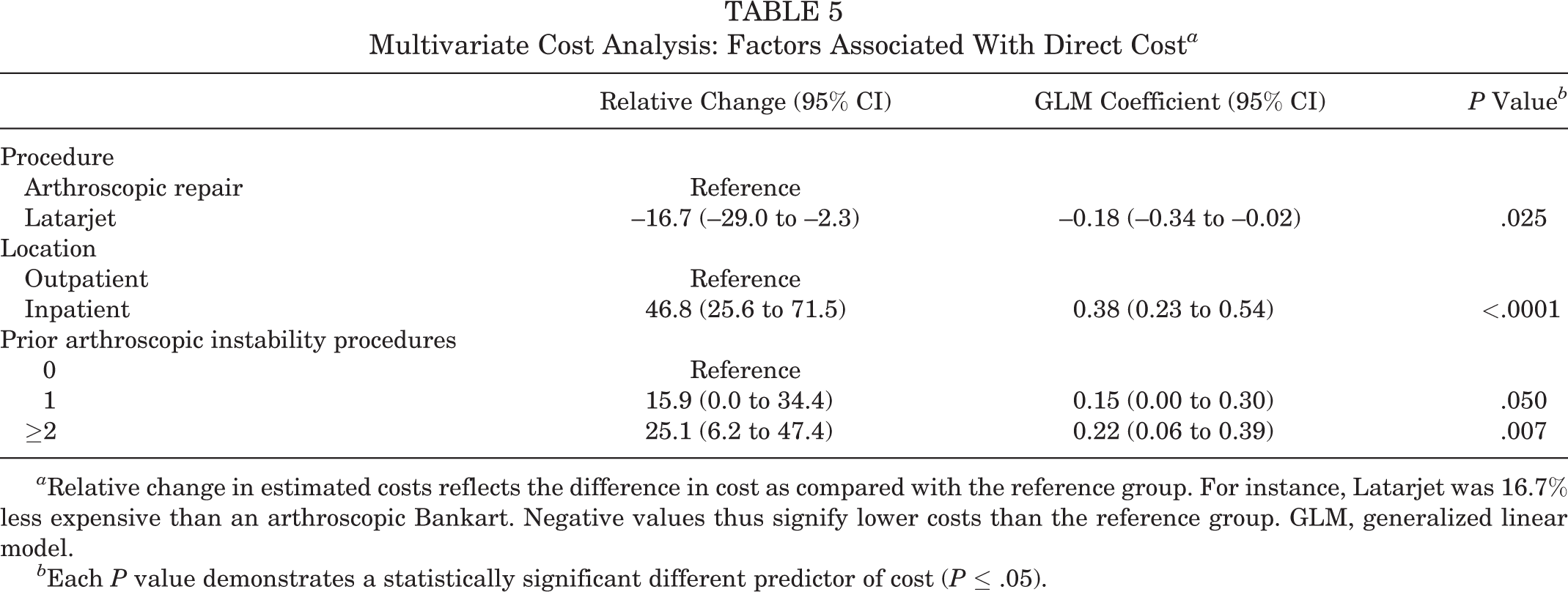
a Relative change in estimated costs reflects the difference in cost as compared with the reference group. For instance, Latarjet was 16.7% less expensive than an arthroscopic Bankart. Negative values thus signify lower costs than the reference group. GLM, generalized linear model.
b Each P value demonstrates a statistically significant different predictor of cost (P ≤ .05).
Discussion
Controlling for patient characteristics, arthroscopic Bankart repair was 17% more costly than Latarjet, with OR supplies/implant cost (ie, number and/or cost of suture anchors) being the primary driver of cost difference. All other cost domains—including OR/facility utilization cost (a strong surrogate for operative time), non-OR/facility utilization (an indicator of preoperative and PACU care), and others—favored arthroscopic Bankart. Direct cost in Latarjet and arthroscopic Bankart repair differed significantly as a factor of the surgical procedure performed, the number of prior arthroscopic procedures performed, and whether the procedure was performed in an ambulatory or inpatient setting. In a subgroup univariate analysis, DTA was 2.9-fold more costly than Latarjet.
Our study demonstrated that when considering direct costs and accounting for patient-specific factors, Latarjet was less costly than arthroscopic Bankart repair. The 2 previous studies examining cost comparisons between arthroscopic Bankart and Latarjet did not examine direct costs and reached conflicting conclusions regarding which procedure is less expensive. 16,17 Our findings seemed to rely solely on the implant cost (ie, the type or number of suture anchors used). The mean number of anchors used within the arthroscopic group of our study was 3.5 ± 0.8, which is similar to the number of anchors used in prior cost studies. These studies utilized 3 or 4 total 2.4-mm BioComposite SutureTak Anchors (Arthrex Inc) and did not publish implant cost explicitly. 16,17 This difference drove the 17% cost difference, which is larger than the 5% and 11% difference found in the 2 prior reports using cost-effectiveness analysis data. 16,17 Boileau et al 3 reported on higher rates of recurrence with arthroscopic Bankart repairs with fewer than 3 anchors. In light of this finding and our current data regarding cost, reduction in the number of anchors or scrutiny of individual anchor cost is a reasonable strategy to narrow the cost gap, although the former may increase recurrence risk.
In our study, OR/facility utilization cost, a strong surrogate of operative time, was lower in the arthroscopic Bankart group when compared with Latarjet, as one may expect. Previous cost studies support this. Makhni et al 16 presumed a set 120-minute operative time for the arthroscopic Bankart and Latarjet, while Min et al 17 presumed a significantly lower operative time of 52 minutes for the Bankart group as compared with a modest reduction in OR time of 84 minutes for the Latarjet group; and these studies reached opposite conclusions commensurate with these differences. The conflicting findings in these studies highlights the importance of ascertaining differences in direct costs because if one can choose between similar procedures, the cheaper option is often chosen.
The results of the study clearly identified the factors associated with higher cost in Latarjet and arthroscopic Bankart repair. Direct cost in Latarjet and arthroscopic Bankart repair differed significantly regarding several factors. Nonmodifiable factors included the number of prior arthroscopic procedures performed. Modifiable factors included the procedure performed and whether the procedure was performed in an ambulatory or inpatient setting. The number of prior arthroscopic procedures, while also nonmodifiable, may serve as a marker of increased complexity and likely increased OR time in the Latarjet and arthroscopic settings, leading to higher costs. This is an important point to consider, as while Latarjet was less costly within this study, a much larger proportion of patients undergoing Latarjet had undergone prior failed arthroscopic or open stabilizations. Regarding the modifiable factor of surgical setting, we found that anterior instability surgery performed in the inpatient setting was 47% more costly than the outpatient ambulatory hospital setting. Continued emphasis on performing anterior instability surgical procedures in outpatient settings in the correct clinical scenarios will aid in lowering costs.
Our results further demonstrated that DTA was 2.9 times more expensive than Latarjet. This is the first descriptive study to report on the cost of DTA and the difference in cost between the procedures. The finding is important, as glenoid reconstruction with DTA for recurrent anterior instability as described by Provencher et al 20,21 provides many potential benefits over Latarjet. The graft provides an opportunity to reconstruct larger areas of the articular surface, with articular cartilage re-creating a smooth glenoid arc of articulation throughout range of motion without the associated donor site morbidity of a coracoid transfer. The size and weightbearing nature of the distal tibia provide excellent screw fixation over the potentially smaller coracoid. 11,20,21 Coracoid transfer, however, does not carry a risk of disease transmission or a large associated cost and is not subjected to a narrow time window for implantation.
Despite the potential added benefits of the DTA technique, current research shows equivalent outcomes with Latarjet. Frank et al 11 reported on a matched comparison of 50 Latarjet and 50 DTA procedures in 2018 and found no significant differences in recurrence rates, complication rates, or reoperation rates. While there was a significant difference in Simple Shoulder Test scores favoring Latarjet, there were no significant differences in Western Ontario Shoulder Instability Index, American Shoulder and Elbow Surgeons score, pain visual analog scale, or Single Assessment Numeric Evaluation scores. While our study reported on a small cohort and did not specifically compare outcomes in terms of cost, it is important to consider the important potential benefits provided by DTA while taking into account its higher cost and equivalent outcomes. It is also important to note that there are neither long-term outcome studies nor other comparative studies other than the data previously cited. In contrast to arthroscopic Bankart, outside of select institutions, very few DTA procedures are currently performed, and increased costs demonstrated within this study could be a result of a learning curve or other inefficiencies. Future comparative studies will be needed and should be interpreted in light of the substantial difference in cost. To be considered a viable primary alternative to Latarjet, DTA will need to demonstrate substantially better outcomes at midterm and long-term follow-up to account for the magnitude of cost difference seen between the procedures. However, this cost differential should not limit consideration of DTA in the setting of a clear clinical indication, as there are certainly some clinical situations where DTA may be the best alternative (eg, revision from prior failed Latarjet).
Limitations
This study is not without limitations. This was a retrospective comparative study. All patients undergoing concomitant procedures other than isolated anterior Bankart repair were excluded in an effort to provide a better direct comparison. However, it is possible that residual confounding differences may have existed among groups. Another significant limitation of this study is due to its retrospective design. The cohorts were inherently different as a function of important risk factors to include bone loss and history of prior surgical stabilization. This difficulty arises because the surgeons used different indications for arthroscopic Bankart and open Latarjet stabilization. In particular, Latarjet was reserved for cases with critical bone loss in high-risk patients or in those who had failed prior stabilizations. Thus, a matched analysis based on bone loss was not possible, given that the groups were inherently different in this regard. Rather, patients were matched in a random 2:1 fashion to control confounders to better differentiate direct costs as a factor of patient and surgical characteristics for use as a clinical tool. While these differences are important, they do reflect typical practice patterns.
The most controversial limitation of this study is the inability to report cost differences in actual dollar amounts. Presenting the cost data in a normalized fashion protects confidential price negotiation, and there is a growing body of literature reporting cost data in this normalized fashion. 8,13,23 However, there is a concern with the generalizability of any cost differences if there are significant differences in implant prices among centers. This may limit the ability to extrapolate the findings to other institutions. Recent literature examining the total cost of total hip arthroplasty demonstrated a nearly 2-fold difference in cost among centers within the same community despite similar patient demographics, complication rates, and readmission rates, with price negotiation for implants accounting for a large proportion of cost variance. 12 It is therefore conceivable that hospitals with large differences in negotiated implant pricing may reach opposing conclusions regarding which procedure is less costly.
Finally, we limited the scope of this study to the surgical encounter and did not perform a cost-utility analysis. 18 A cost-utility analysis incorporates pre- and postoperative patient outcomes in addition to procedure-related costs to identify a cost per health unit gain. This is typically expressed as a quality-adjusted life-year. By limiting the cost data to the initial surgical encounter, we did not capture any differences in future expenditures from surgery-related complications and revision surgery, and we did not account for differences in patient-reported outcomes between the procedures. However, there is a growing body of literature seeking to identify important modifiable factors that drive higher costs in common arthroscopic procedures, such as anterior cruciate ligament reconstruction and rotator cuff repair. 5,9,13,15,22 Similar to the present study, these were not cost-utility or cost-effectiveness analyses. Nevertheless, as with the present study, these studies increase physicians’ awareness of the modifiable primary drivers of procedure costs—in this case, implant costs and surgical setting.
Conclusion
This study analyzed the direct costs associated with the surgical encounter without including future costs or patient outcomes, and findings indicated that the open Latarjet procedure is less costly than an arthroscopic Bankart repair after controlling for patient characteristics. Value-driven surgical strategies to narrow the gap in surgical technique should focus on reduction of overall implant cost. Emphasis should be placed on performing these procedures in an ambulatory setting, as performance of instability procedures in the inpatient setting is associated with significant cost. Last, the perceived potential benefits of DTA over Latarjet may be substantially outweighed by higher direct costs.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.T.B. has received royalties from Arthrex; consulting fees from Arthrex, DePuy, VirtaMed, and Cayenne Medical; research support from DePuy; speaking fees from DePuy; and educational support from Pinnacle. R.Z.T. has received royalties from Wright Medical and Zimmer-Biomet; has received consulting fees from Zimmer-Biomet, DePuy, and Cayenne Medical; and has stock/stock options in Connextions, Imascap, Shoulder Innovations, and DePuy. P.N.C. has received consulting fees from DePuy and hospitality payments from Tornier. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the University of Utah Institutional Review Board (IRB 00071740).