
Abstract

Keywords
The patient in this case report was a 16-year-old, healthy, right-hand dominant male who presented to the emergency department with right elbow pain and swelling after a fall while playing basketball earlier the same day. He landed directly on his right elbow, which resulted in immediate pain, swelling, and inability to use the extremity. No other injuries were sustained. He had no history of injury or pain to the right elbow. He also had no history of tobacco or drug use. On physical examination, there was mild swelling and tenderness to palpation of the olecranon along with a palpable gap at the fracture site. He was neurovascularly intact distally. Compartments of the arm were soft and compressible. Initial anteroposterior and lateral radiographs of the right elbow demonstrated a persistent olecranon apophysis determined by smooth, rounded edges without cortical interruption and bony separation through the olecranon apophysis involving approximately 40% of the joint surface with 1.5-cm displacement (Figure 1, A and B). Contralateral elbow radiographs confirmed that the left olecranon physis was closed (Figure 2).

Initial injury radiographs, (A) anteroposterior and (B) lateral, demonstrating displaced olecranon apophyseal fracture.

Contralateral left elbow lateral radiograph demonstrating no olecranon physis.
The decision was made to proceed with open reduction and internal fixation (ORIF). There was an underlying elbow flexion contracture of approximately 15° preoperatively during examination under anesthesia. A posterior approach was utilized, with a longitudinal curvilinear incision centered over the olecranon. Full-thickness flaps were developed down to the fracture site. On visualization of the fracture site, it was apparent that the fracture extended through a persistent olecranon physis because of rounded bony edges, smooth cartilage in place of cancellous intramedullary bone, and fractured cartilage at the joint surface, suggesting preinjury physeal deformity and nonunion. The fracture site was subsequently debrided and the persistent physeal cartilage was removed. Indirect articular reduction was first attempted by lining up the dorsal olecranon surfaces using a tenaculum clamp with a drill hole in the dorsal cortex of the distal fragment. K-wires were then used for provisional fixation, and reduction was checked on multiplanar fluoroscopy (Figure 3). Obvious deformity at the articular surface was noted on fluoroscopy when using the posterior olecranon cortical surface as a reference.
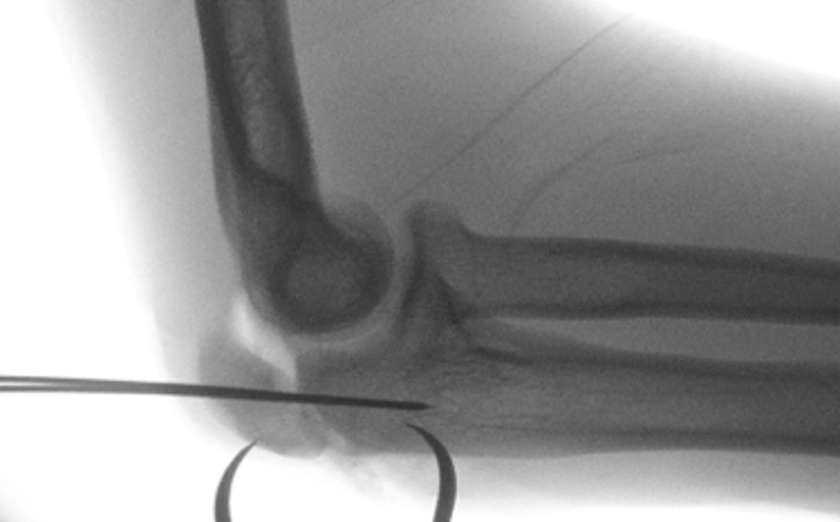
Fluoroscopic lateral radiograph showing the reduction by lining up the posterior cortical surface with provisional fixation, which demonstrates malalignment of the articular surface.
Subsequently, provisional fixation was removed and direct reduction was then performed by aligning the elbow articular cartilage. K-wires were used again for provisional fixation, and a congruent joint surface was achieved. Although the articular cartilage was in near-anatomic alignment and a smooth elbow range of motion (ROM) was noted, there was a mismatch between the posterior bone edges of the dorsal olecranon because of the chronic injury of the olecranon physis after removal of the persistent cartilage. An olecranon variable-angle plate (Trimed Inc) was then placed and affixed into position without complication (Figure 4). The olecranon plate was used because of concerns that a tension band construct may cause gapping at the articular surface in this case where a gap was noted dorsally. The aforementioned dorsal cortex mismatch and fracture gap was filled with 3 mL of demineralized bone matrix allograft to help stimulate fracture healing and minimize nonunion via its osteoconductive and osteoinductive properties. Although bone autograft is widely considered the gold standard because of its osteoinductive, osteoconductive, and osteogenic capabilities, allograft was selected to avoid donor-site morbidity, particularly when employed in a pediatric patient in order to fill in the gap created by the removal of the persistent physis. An anterior elbow splint preventing more than 15° of elbow flexion was then applied (Figure 5).

Fluoroscopic lateral radiograph showing reduction with articular congruity and fixation achieved with K-wires and olecranon plate. Dorsal olecranon gapping is noted with adequate articular congruity because of the fracture going through a persistent olecranon physis.
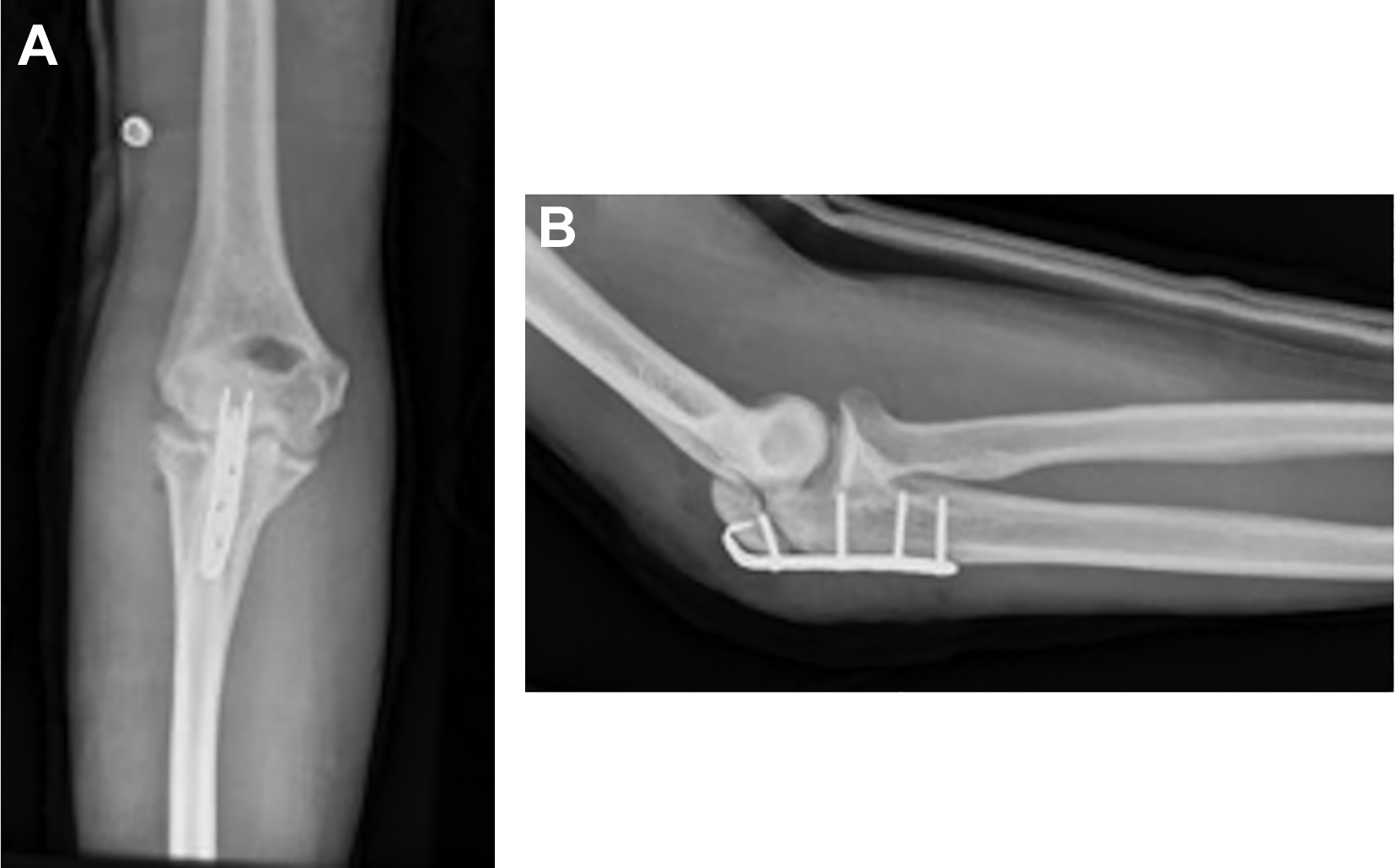
Final radiographs, (A) anteroposterior and (B) lateral, of reduction using olecranon plate.
Two weeks postoperatively, the patient underwent physical therapy for progressive ROM, without motion restrictions. Six weeks postoperatively, the patient had 15° to 110° of elbow flexion as well as full pronation and supination without pain, with maintained reduction on radiographic imaging (Figure 6).

(A) Anteroposterior and (B) lateral radiographs 10 months postoperatively showing improved union across the fracture site.
The patient continued to progress clinically and started playing basketball 3 months postoperatively. Progressive radiographic obliteration of the fracture gap signifying bony healing was noted, and during his last appointment (10 months postoperatively), he was found to have a painless elbow ROM ranging from 8° to 150° of flexion and no tenderness at the fracture site. His Mayo Elbow Performance Score was 100, and his pain rating on a visual analog scale was 0. A follow-up was obtained through telephone 2.5 years postoperatively; the patient continues to have no issues of hardware prominence and continues to play basketball without symptoms.
Discussion
Elbow fractures represent approximately 5% to 10% of all pediatric fractures. 7 Of these, the incidence of an isolated olecranon fracture is 12% to 20%, 7,24 with physeal injury still rarely described in the orthopaedic literature. 6,10,11,17,29,31 The olecranon initially forms as multiple ossification centers which are first radiographically apparent at age 9 to 11 years and fuse by 13 to 17 years. 5,6,10,14,17,28 This process begins on the anterior border of the olecranon and progresses in a proximal-to-distal direction. 11,17 As is the case in a substantial set of pediatric fractures, avulsion forces at tendinous insertions are a common cause and mechanism of injury. With regard to olecranon anatomy and pattern of injury, there exists some debate as to the exact insertion of the triceps expansion, with some authors describing its location distal to the olecranon physis 28,36,39 and others describing the insertion directly into the olecranon physis. 31,33
Because of the rarity and infrequency of physeal fractures at the olecranon, there is no accepted standard method or indication for treatment. The most commonly cited indication for operative intervention is the degree of fracture displacement, but this varies between studies from displacements greater than 2 to 5 mm on initial radiographs. 3,10,14,18,21,27,31,34 Still others advocate for surgery when there is any incongruence of the articular surface 31 or if palpation of the olecranon defect during elbow ROM demonstrates any instability. 39
More commonly seen than displaced persistent olecranon physeal fractures are mildly displaced fractures of the physis in younger children. One study of 16 adolescent baseball players with symptomatic persistent olecranon physes showed a high success rate of nonoperative treatment with activity modification if there was simple widening of the olecranon physis compared with the contralateral side. However, the 4 patients that had significant sclerosis at the physis at the time of presentation did not have resolution of symptoms or physeal closure with nonoperative treatment (all eventually underwent surgery). 26 Fractures that are deemed operative have traditionally been treated with a tension band technique, with overall good clinical outcomes. ‡ Minimal loss of extension has been commonly reported. 1,10,12,15,18,29,31 There exist some well-described complications, including K-wire migration, symptomatic hardware, and loss of reduction. 10,19,21 The tension band implants typically are removed postoperatively, as they are commonly prominent. In a long-term clinical follow-up study of pediatric olecranon fractures treated with casting or with open reduction and tension band techniques, Karlsson et al 21 demonstrated that a tension band technique in fractures displaced more than 4 mm resulted in promising clinical outcomes up to 25 years after injury, even with cases of small articular incongruity. Another long-term follow-up study of 39 patients with primarily nonoperatively treated pediatric olecranon fractures showed good clinical results at an average of 24 years after injury. Additionally, these patients' previous injury did not influence their choice of occupation. 3
Several case series and case reports of painful persistent olecranon physes have been described, mostly in overhead athletes such as baseball players, 4,9,13,25,26,30 weight lifters, 38 and tennis players. 32 In our review of the literature, the prevalence of bilateral persistent olecranon physis was not well documented; however, almost all studies that included a contralateral elbow radiograph had complete fusion of the olecranon, as in our patient.
Although the exact cause is unknown, a preoperative elbow flexion contracture of 15° to 30° is common in these cases. 4,25,30,32 Perhaps genetic predisposition or repetitive microtrauma (possibly creating a persistent physis) also contributed to the development of a soft tissue flexion contracture. The possibility also exists that abnormal elbow mechanics resulting from lack of full extension alters the position of the limb during injury, transmitting abnormal forces across the joint. In our patient, there was no mention of previous elbow ROM limitations in the medical history. Ten months postoperatively, our patient was noted to have an elbow ROM ranging from 8° to 150°, an improvement from his preoperative examination under anesthesia (a flexion contracture of 15°). Although no anterior soft tissue release was performed, by closing the persistent physeal gap, there was likely a decrease in posterior olecranon fossa impingement allowing for improved elbow extension. In these cases, ORIF with or without bone grafting is typically performed after months of failed nonoperative treatment, 4,9,13,25,26,30,38 most commonly with a tension band construct, although nonoperative treatment has been successfully attempted in young patients. 25,32 Good outcomes have been obtained with ORIF, with a high healing rate. 4,9,13,25,26,30,38 The most common complications are hardware prominence and subsequent need for hardware removal. 4,13,25 Nonunion appears to be rare after ORIF of persistent nondisplaced olecranon physes.
Only 8 cases of displaced persistent physeal fractures have been reported in adults 4,8,23,35,37 ; the case details are outlined in Table 1. One 26-year-old soccer player had a displaced olecranon fracture after a fall on his previously asymptomatic elbow and was treated with ORIF with tension band wiring that developed a nonunion. 35 The patient subsequently underwent a wedge-shaped osteotomy and revision internal fixation with a tension band construct that united. One case series reported 3 patients with displaced persistent olecranon physes after direct trauma. 23 All underwent ORIF with tension band construct after curettage of the physeal surfaces, and each patient went on to nonunion, with 2 patients undergoing revision ORIF with bone grafting and 1 refusing subsequent surgery. 23 Enishi et al 8 reported on a 36-year-old former baseball player with a displaced fracture through a persistent olecranon physis; the patient underwent ORIF with a tension band construct with iliac crest autograft that ultimately united with removal of internal fixation 13 months postoperatively. Charlton et al 4 reported a case of a displaced persistent olecranon fracture in an 18-year-old baseball pitcher who underwent ORIF using tension band construct and autograft iliac crest bone graft. This healed uneventfully and hardware removal was performed, although the reason for removal was not reported. Turtel et al 37 reported on 2 cases of similar displaced olecranon fractures treated with ORIF with tension band technique, with both resulting in a fibrous union but good clinical outcomes. In all of these previously reported cases of displaced fractures through persistent olecranon physes, the final outcomes were good, but ORIF using a K-wire and tension band construct resulted in a 75% nonunion or fibrous union rate (6 of 8 cases). The only cases that healed were the 2 cases in which primary iliac crest bone autograft was used at the time of initial fixation, while none of the nonunion cases reported the use of bone graft of any type (Table 1).
Review of all Reported Cases of Displaced Persistent Olecranon Physes a

a DBM, demineralized bone matrix; ICBG, iliac crest bone graft (autograft); ORIF, open reduction and internal fixation; ROH, removal of hardware.
To our knowledge, no other cases in the literature describe the initial treatment of a displaced persistent olecranon physis in a healthy adolescent with a plate and screw construct, although some cases may be included in the case series that were not identified as persistent physes. In this case, the tension band technique would be difficult given the lack of bony contact because of a dorsal fracture gap (from persistent physeal cartilage removal), thus preventing adequate apposition at the fracture site and resulting in an incongruous articular surface. The advantages of plate and screw fixation with bone allograft of the associated defect in these cases are that stable fixation is achieved to allow for union across the gap created by removal of the persistent epiphysis, and reduction can be maintained at the articular surface. In addition, some studies have reported lower rates of symptomatic hardware with a plate and screw construct.
Although less frequently described in the literature for pediatric fractures, plate and screw fixation is widely utilized in the adult population, with good outcomes reported. 2,20,22 In addition, lower rates of symptomatic hardware are seen with a plate and screw construct. 20 A plate and screw construct was used in our patient to give adequate fixation to hold the reduction to allow for healing across the fracture gap caused by removal of the persistent olecranon physis.
Displaced physeal fractures of the olecranon are relatively rare. However, this case highlights that it is difficult to reduce a displaced persistent olecranon physis based on standard methods of aligning the posterior cortex given the preinjury deformity. There is often greater intra-articular displacement seen intraoperatively than is initially appreciated on radiographic imaging, 14 and special attention should be paid to the articular surface during reduction to allow for a congruent joint with minimal articular depression despite potential gapping at the olecranon fracture site. 10,16 In addition, the cartilage needs to be removed on both sides of the physis before fixation and, given the literature review, we recommend supplemental use of allograft or autograft of the subsequent defect to allow for bony healing in cases of a persistent physis.
Conclusion
Olecranon physeal fractures in healthy adolescents are rare. Outcomes after ORIF are generally good, but some loss of extension is common. Displaced olecranon fractures through a persistent physis can be successfully treated with ORIF using a variety of techniques; however, given the cases reported in the literature, there can be a consideration for a plate and screw construct and bone grafting to fill the gap at the time of initial surgery, as well as complete removal of persistent physeal cartilage. We recommend the use of any form of bone graft to fill the defect left by removal of the physeal cartilage because of the high nonunion rate (100% nonunion rate in 6 cases) reported in the literature in cases without bone graft. In addition, we present this case as an illustration of the importance of using the articular cartilage as a guide for anatomic reduction and to allow full ROM, which led to an excellent clinical result in this case.
Footnotes
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.