
Abstract
Background:
Even in patients with an open capitellar physis, nonsurgical treatment for advanced-stage osteochondritis dissecans (OCD) of the capitellum often yields poor outcomes. However, surgical methods for such patients are controversial. At our institution, we have consistently performed closed-wedge osteotomy of the distal humerus to treat advanced-stage OCD of the capitellum, regardless of the OCD grade or condition of the capitellar physis.
Purpose:
To clarify the clinical and radiological results and determine the influence of the capitellar physis on closed-wedge osteotomy for advanced-stage OCD of the capitellum in young patients.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 32 patients with OCD of the humeral capitellum were treated surgically with closed-wedge osteotomy. Of these, 17 patients with more than 2-year follow-up were available for an evaluation. The mean patient age was 11.8 years (range, 11-12 years), and the mean follow-up period was 70.1 months (range, 25-184 months). The clinical assessment included range of motion, elbow pain, and the Japanese Orthopaedic Association (JOA) and Timmerman-Andrews scores. The radiological assessment at the final examination included cross-bridging of the physis, size and fishtail deformity of the distal part of the humerus, size of the radial head, healing of the OCD lesion, and osteoarthritis.
Results:
The mean range of motion and JOA and Timmerman-Andrews scores improved significantly after surgery; 13 patients were completely pain free. In 11 patients with an open capitellar physis, metaphyseal-epiphyseal, cross-bridging was observed in 1 patient. A fishtail deformity of the distal part of the humerus was not observed. Healing of the OCD lesion was defined as excellent in 9 patients, good in 3, fair in 3, and poor in 2. In 3 of the 5 patients in whom healing was described as fair or poor, there was a lesion of the lateral widespread type with osteoarthritis before surgery. Moderate osteoarthritic changes were evident in 2 patients.
Conclusion:
Closed-wedge osteotomy for the treatment of advanced-stage OCD of the capitellum in young patients can provide satisfactory clinical and radiological results. However, fair and poor outcomes were found in lateral widespread–type cases with osteoarthritis before surgery. We believe that patients in whom osteoarthritic changes have not yet appeared are eligible for closed-wedge osteotomy.
Osteochondritis dissecans (OCD) of the capitellum typically occurs in young baseball players aged 11 to 17 years. 1,3,28 Grade I OCD is usually diagnosed at 11.5 years. Younger patients are usually at an early OCD stage. Because the capitellar physis is usually open in patients younger than 12 years, such patients are usually treated conservatively. However, advanced-stage OCD of the capitellum can occur in young patients, and surgical treatment has been shown to yield better clinical results in such cases, even if the capitellar physis is open. 13,20,21
Surgical options for advanced-stage OCD include open or arthroscopic debridement or removal of loose bodies, fragment fixation, osteochondral autografting, and closed-wedge osteotomy. The advantages of closed-wedge osteotomy for OCD of the capitellum are reduced compression of the capitellum, revascularization and remodeling of the OCD lesion, and long-term maintenance of the congruity of the humeroradial joint. This technique has also shown good medium- and long-term outcomes for advanced-stage OCD of the capitellum. 7,30 At our institution, we consistently perform closed-wedge osteotomy for advanced-stage OCD of the capitellum, regardless of the OCD stage or condition of the capitellar physis. In cases where the capitellar physis is open, the osteotomy line, similar to the fracture line of the lateral condylar fracture of the humerus, crosses the physis.
Over the past 24 years, we have treated OCD of the capitellum in young patients with open capitellar physis using osteotomy. The aim of this study was to evaluate the clinical and radiological results and the influence of the capitellar physis on closed-wedge osteotomy in patients aged ≤12 years with an open or closed capitellar physis.
Methods
Patients
This study received ethics committee approval from Niigata Central Hospital. Between 1986 and 2009, a total of 32 patients aged ≤12 years with OCD of the humeral capitellum were surgically treated with closed-wedge osteotomy at Niigata Central Hospital and were evaluated at least 2 years after surgery. Of these patients, 17 (53.1%) were reviewed in the present study; 14 patients were excluded because they could not participate in the survey or because the radiographs at the final examination were not available. One patient was excluded because he suffered a humeral shaft fracture due to trauma after surgery.
All 17 study patients were male. Four patients were 11 years old, and 13 were 12 years old at the time of surgery. The mean follow-up duration was 70.1 ± 41.8 months. The capitellar physis was open in 11 patients and closed in 6 at the time of surgery. The sport related to symptom onset was baseball (13 patients) as well as soccer, dodgeball, and softball (1 patient each). Intraoperative findings of the OCD lesion were graded according to the International Cartilage Repair Society (ICRS) classification. 5 Eleven were categorized as ICRS grade III, and 6 were categorized as ICRS grade IV. Based on the site of the OCD lesion, radiographic findings were classified as central, lateral-localized, and lateral-widespread types; a lateral-widespread OCD lesion was defined as an extension to one-third of the capitellum involving the lateral margin. 8 A central lesion was observed in 8 patients and a lateral-widespread lesion in 9 patients. At both the preoperative and final examinations, radiographic findings of osteoarthritis were classified into 4 grades: grade 0, normal; grade 1, sclerosis or irregularity of the subchondral bone and no narrowing of the joint space; grade 2, slight narrowing of the joint space and osteophytes with a wide stalk; and grade 3, marked narrowing of the joint space and osteophytes with a narrow stalk or the presence of free bodies. 18 At the preoperative examination, 14 patients were classified as having grade 0 osteoarthritic changes, and 3 were classified as having grade 1 osteoarthritic changes according to these criteria.
Operative Technique
A curved incision was made over the lateral aspect of the elbow from a point 5 cm proximal to the lateral epicondyle to the radial head. Dissection was performed anteriorly, releasing the brachioradialis and extensor carpi radialis longus from the lateral supracondylar ridge of the humerus. This dissection was continued distally between the extensor carpi radialis longus and the extensor carpi radialis brevis, allowing exposure of the anterior capsule with preservation of the lateral collateral ligament and origins of the extensors of the wrist and fingers from the lateral epicondyle. This provided good access to the anterior aspect of the radiohumeral joint. The lateral collateral ligament was severed to widen the radiohumeral joint. The capitellum was exposed, and the articular cartilage and subchondral bone were inspected. Loose bodies present in the radiohumeral joint and/or proximal radioulnar joint were removed.
Wedge osteotomy, with the base positioned laterally and a 10° angle of intervention, was performed at a site 2 to 3 cm proximal to the lateral epicondyle, with its apex just medial to the capitellum. The posterior aspect of the capitellum was not exposed because the capitellum receives its main blood supply from the posterior aspect of the distal humerus. The articular surface of the apex was kept intact. Cancellous bone was collected from resected wedgelike bone, and bone pegs were made from cortical bone. If dislocated fragments or loose fragments were large and remained in the subchondral bone, they were fixed using bone pegs after transplanting cancellous bone between the fragment and its bony bed; bone peg fixation was performed in 16 patients. Small fragments were removed. The osteotomy site was closed, and stable fixation was obtained using a screw and Kirschner wire 7,29 (Figure 1). No repair of the severed lateral collateral ligament was performed.

Illustrations of closed-wedge osteotomy of the distal humerus.
Postoperative Treatment
After surgery, a long arm cast was applied with the elbow at 90° flexion and the forearm in the neutral position for 3 weeks. At 3 weeks after surgery, the patient began active range of motion (ROM) exercises to prevent deterioration of the lesion. At 2 to 3 months after surgery, mild passive ROM exercises were initiated. Return to throwing activities was permitted 6 months after surgery.
Clinical Assessment
Clinical evaluations included elbow ROM (total arc), pain, return to sports, and elbow function at the time of the final examination. Elbow function was assessed according to the clinical rating system of the Japanese Orthopaedic Association (JOA) 9 as well as the Timmerman-Andrews score. 24
Radiological Assessment
We observed metaphyseal-epiphyseal cross-bridging, fishtail deformity, and width of the lataral condyle and the radial head using postoperative radiographs to investigate the effect of closed-wedge osteotomy on the physis. A central deficiency of the distal humerus was defined as a fishtail deformity. The width of the lateral and medial condyles of the humerus was measured as shown in Figure 2. 19 The width of the lateral condyle divided by the width of the medial condyle was defined as the lateral condyle ratio. The lateral condyle ratio was compared between the affected and unaffected sides.

Radiograph showing the width of the lateral condyle (A), width of the medial condyle (B), and lateral condyle ratio (A/B).
The radial head ratio was defined as the maximum width of the radial head divided by the minimum width of the radial neck, measured as described in Figure 3. Healing of the OCD lesion was evaluated at the final examination and was classified into 4 grades: excellent, completely healed; good, slight flattening; fair, subsidence; and poor, displaced or detached fragment. 6 Osteoarthritis was graded at final follow-up.

Radiograph showing the width of the radial head (C), width of the radial neck (D), and radial head ratio (C/D) . 6
Statistical Analysis
Statistical analysis was performed using the paired or unpaired Student t test, Mann-Whitney U test, Wilcoxon signed-rank test, Pearson product moment correlation coefficient, and Fisher exact probability test. The paired Student t test was used to compare elbow ROM preoperatively and postoperatively. The unpaired Student t test was used to compare the radial head ratio between the affected and unaffected sides and ROM in the open and closed physes. The Mann-Whitney U test was used to compare the size of the lateral condyle on the affected side with that on the unaffected side. The Wilcoxon signed-rank test was used to compare preoperative JOA and Timmerman-Andrews scores with postoperative scores.
Differences between an open and closed capitellar physis with respect to the size of the lateral condyle and hypertrophy of the radial head were analyzed using the Mann-Whitney U test. Healing of the OCD lesion was classified as complete or incomplete; cases graded as excellent were included in the completely healed group, and other cases were included in the incompletely healed group. We considered patients with osteoarthritis grade 0 at final examination as having no osteoarthritis and those with grades 1 to 3 as having osteoarthritis. Differences between these 2 groups with respect to elbow ROM and hypertrophy of the radial head ratio were analyzed using the unpaired Student t test, and differences with respect to JOA and Timmerman-Andrews scores were analyzed using the Mann-Whitney U test. Relationships among outcomes in terms of elbow pain at the final examination, site of the OCD lesion, healing of the OCD lesion, and presence of osteoarthritis were confirmed using the Fisher exact probability test. Correlations between the radial head ratio and elbow ROM at the time of the final examination were analyzed using the Pearson product-moment correlation coefficient. A difference was considered significant when the P value was <.05.
Results
The patients’ clinical and radiological results are illustrated in Tables 1 and 2.
Patient Characteristics a
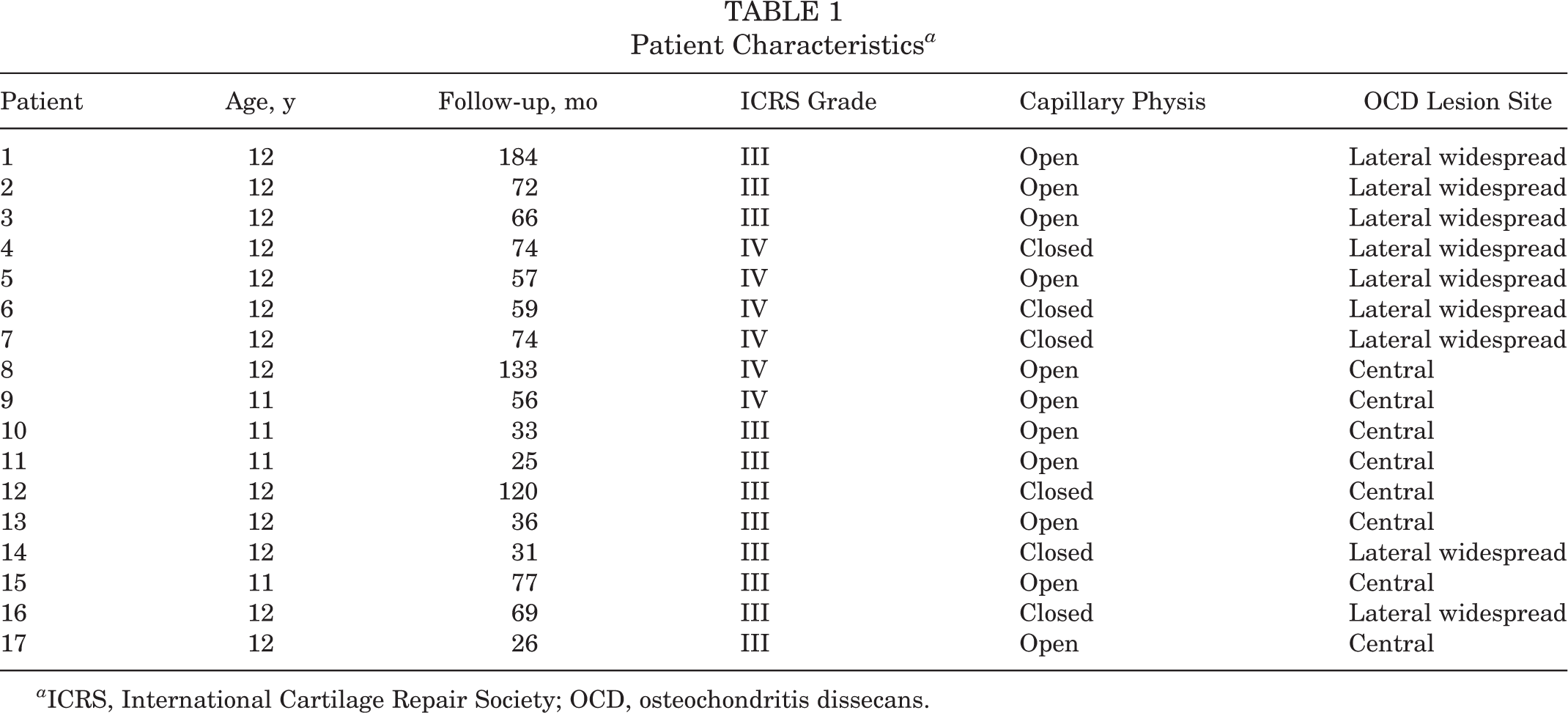
a ICRS, International Cartilage Repair Society; OCD, osteochondritis dissecans.
Clinical and Radiological Results a

a JOA, Japanese Orthopaedic Association; Post, postoperative; Pre, preoperative; ROM, range of motion.
Clinical Assessment
Range of Motion
The mean ROM of the elbow improved significantly, from 117.8° ± 25.2° preoperatively to 131.4° ± 17.2° postoperatively (P = .024). The mean ROM of the elbow was 131.8° ± 16.5° in the open physis group and 130.5° ± 20.1° in the closed physis group (P = .886), it was 137.2° ± 16.2° in the completely healed group and 124.8° ± 16.8° in the incompletely healed group (P = .14), and it was 129.1° ± 15.9° in the osteoarthritis group and 135.5° ± 20.2° in the no osteoarthritis group (P = .481) There was no between-group difference in any of the comparisons. No significant correlation between the radial head ratio and ROM was found (γ = –.344, P = .19).
Elbow Pain
All patients reported pain before surgery; however, 13 were pain free at the time of the final examination. Slight pain during elbow motion was reported in 3 patients and mild pain during daily activities in 1 patient. The relationship between pain and open/closed physis, healing of the OCD lesion, or osteoarthritis was assessed. Elbow pain persisted in the incompletely healed group versus the completely healed group (P = .029), but the state of the physis or presence of osteoarthritis was not related to pain (P = .555). Elbow pain persisted in 2 patients with grade 2 osteoarthritis.
Return to Sports
Nine of 13 baseball players returned to baseball at the same level as before surgery. Other baseball players chose to play basketball, tennis, or table tennis. One softball player chose to play soccer. One dodgeball player chose to play tennis. The remaining 2 players returned to the same sports after surgery. All patients were club activity–level players.
JOA and Timmerman-Andrews Scores
The mean JOA score improved significantly, from 75.0 ± 11.6 preoperatively to 93.7 ± 8.6 postoperatively (P < .001). The mean Timmerman-Andrews score also improved significantly, from 143.2 ± 32.0 preoperatively to 184.7 ± 19.6 postoperatively (P < .001). These improvements were not related to open/closed physis, completely/incompletely healed lesion, or presence/absence of osteoarthritis (Table 3).
Postoperative JOA and Timmerman-Andrews Scores a

a Data are reported as mean ± SD unless otherwise indicated. JOA, Japanese Orthopaedic Association.
Radiological Assessment
Metaphyseal-Epiphyseal Cross-bridging, Fishtail Deformity, Lateral Condyle Ratio, and Radial Head Ratio
Metaphyseal-epiphyseal cross-bridging was observed in one 11-year-old patient who was classified as ICRS grade III. Four weeks after surgery, metaphyseal-epiphyseal cross-bridging was recognized at the osteotomy site. Two months after surgery, the capitellar physis began to close. A radiograph taken at 8 months after surgery showed that the capitellar physis was completely closed. Deformity, including fishtail deformity, was absent (Figure 4).
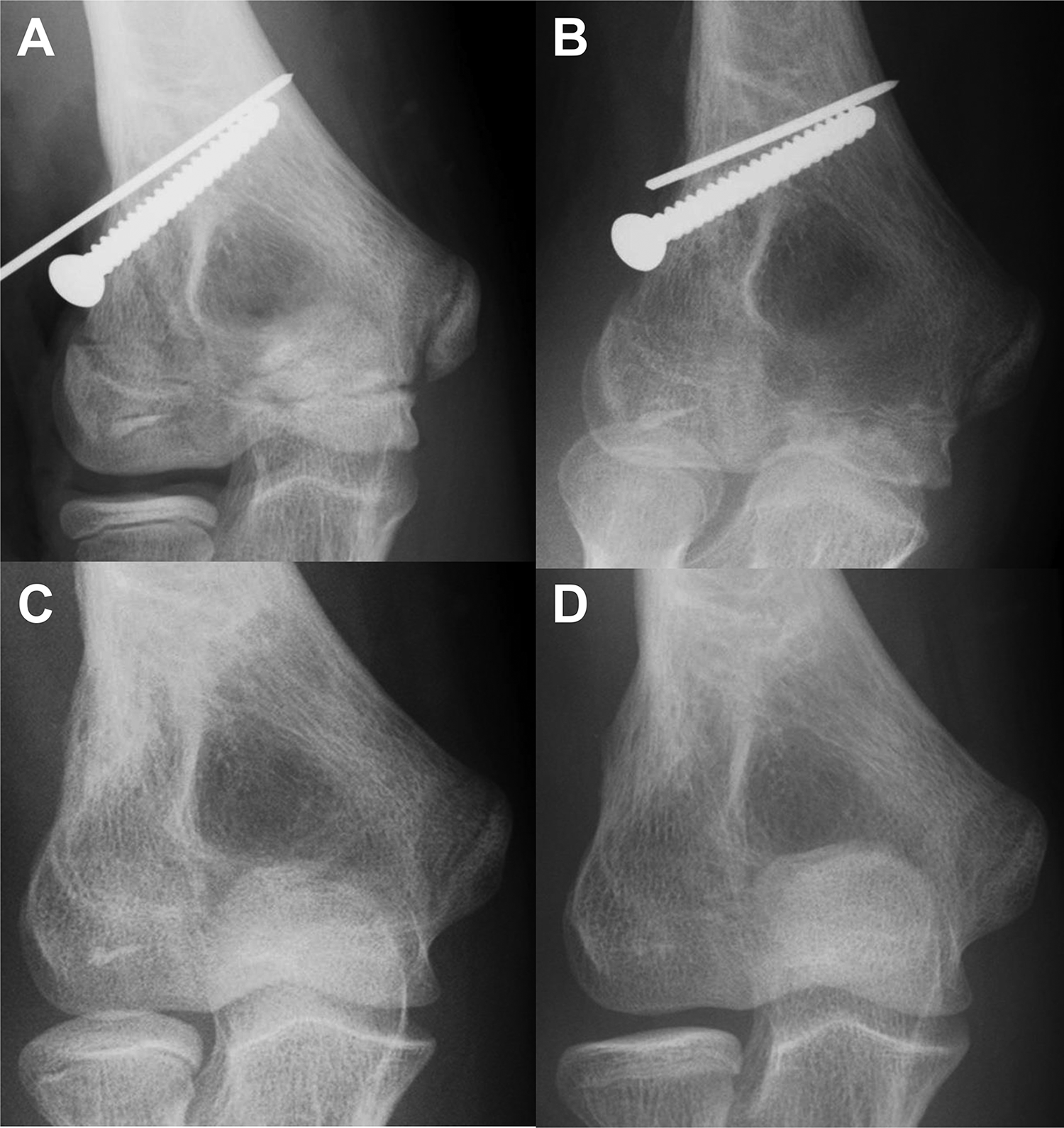
Patient No 15. An 11-year-old boy with an International Cartilage Repair Society grade III osteochondritis dissecans lesion. Anteroposterior radiographs of the elbow (A) at the time of surgery, (B) 1 month later, and (C) 5 months later. (D) At 8 months later, the deformity was absent, and healing of the osteochondritis dissecans lesion was excellent.
The mean lateral condyle ratio was 1.22 ± 0.47 on the affected side and 1.04 ± 0.39 on the unaffected side. This difference was not statistically significant (P = .182). The mean lateral condyle ratio was 0.97 ± 0.43 in patients with an open capitellar physis and 1.15 ± 0.31 in patients with a closed growth plate. This difference was not statistically significant (P = .216).
Healing of OCD Lesion
Healing at the time of the final examination was defined as excellent in 9 patients, good in 3, fair in 3, and poor in 2. Regarding an association between healing and classification of the OCD lesion on the basis of the site, 6 cases of the central type had excellent healing and 2 had fair/poor healing, whereas patients with a lateral-widespread lesion had excellent healing in 3 cases, good in 3, fair in 2, and poor in 1. Three of the 5 cases in which healing was fair or poor had lateral-widespread lesions. There was no relationship between healing and the state of the physis or the site of the OCD lesion (P = .627 and P = .109, respectively) (Table 4). Two of the 5 cases in which healing was fair or poor showed preoperative radiographic findings of osteoarthritic changes.
Relationship Between Healing and Site of OCD Lesion a
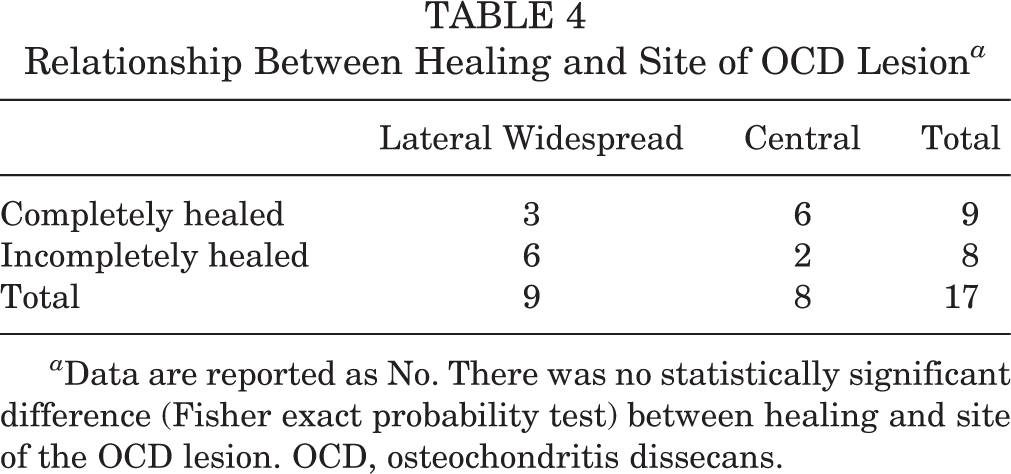
a Data are reported as No. There was no statistically significant difference (Fisher exact probability test) between healing and site of the OCD lesion. OCD, osteochondritis dissecans.
Osteoarthritis
Osteoarthritis grading at the final examination was as follows: 6 patients with grade 0, 9 with grade 1, 2 with grade 2, and 0 with grade 3. For the 11 patients with osteoarthritis at final examination, the preoperative ICRS classification of their lesion was grade III in 7 patients and grade IV in 4 patients. The condition of the physis before surgery was not related to presence of osteoarthritis (P = .661). There was no difference in the frequency of osteoarthritis between the completely and incompletely healed groups (P = .088). Osteoarthritis was more frequently found with a lateral-widespread lesion than with a central lesion (P = .043) (Table 5). Two patients who progressed to grade 2 had a lesion of the lateral-widespread type with grade 1 osteoarthritis preoperatively.
Relationship Between Presence of Osteoarthritis at Final Follow-up and Site of OCD Lesion a

a Data are reported as counts. There was a statistically significant difference (Fisher exact probability test) between lateral widespread and central type. OCD, osteochondritis dissecans.
Radial Head Ratio
The mean radial head ratio was 1.91 ± 0.13 on the affected side and 1.69 ± 0.12 on the unaffected side at the final examination; the affected side was significantly larger than the unaffected side (P < .0001). The mean radial head ratio was 1.87 ± 0.14 in the completely healed group and 1.96 ± 0.12 in the incompletely healed group (P = .157) and 1.93 ± 0.14 in the osteoarthritis group and 1.88 ± 0.12 in the no osteoarthritis group (P = .408). The differences were not statistically significant.
Discussion
Nearly all patients with OCD of the capitellum between 10 and 12 years of age are in an early development stage and have an open physis, thus nonoperative treatment is often recommended for these patients. However, nonoperative treatment for advanced-stage OCD in patients with an open physis may not be effective. 13,21,23 Several surgical procedures have been described for the treatment of OCD. Some authors have performed fragment fixation using a bone peg, drilling, arthroscopic microfracture, and/or osteochondral autografting for advanced-stage OCD lesions with an open physis. 12,17,20,25,26 We consistently perform closed-wedge osteotomy for advanced-stage OCD of the capitellum, regardless of the age at the time of surgery or OCD stage. This is because closed-wedge osteotomy often results in reduced compression of the capitellum and revascularization and remodeling of the OCD lesion, similar to that achieved with radial shortening osteotomy for Kienböck disease. 30
At the beginning, only osteotomy was performed; however, a modification of the osteotomy procedure with bone peg grafting was subsequently devised to further improve performance. Indications for bone peg grafting have only been reported in cases up to ICRS grade I or II. 11,15 Given that the results of this study were obtained for ICRS grade III or IV, we believe that the osteotomy effect is significant. Regarding the clinical outcomes of closed-wedge osteotomy, Kiyoshige et al 7 reported on 7 patients with an early-stage OCD lesion. This procedure led to reduced joint degenerative changes and better clinical outcomes and radiographic findings compared with other surgical procedures for advanced-stage OCD. 7 Our clinical results showed that JOA and Timmerman-Andrews scores improved significantly because of increased ROM and reduced elbow pain after surgery. Our radiographic findings showed no deformity, and good healing was obtained in 12 patients. In cases where healing was fair or poor, hypertrophy of the radial head was suppressed to the same extent as in the patients with good healing. These results indicate that closed-wedge osteotomy is effective for 11- or 12-year-old patients with OCD of the capitellum.
Eight of 9 patients with a lateral-widespread lesion had developed osteoarthritis at the time of the final examination. Patients with a lateral-widespread lesion with osteoarthritis before surgery had worse radiographic and clinical outcomes than other cases examined in this study. However, osteoarthritis was maintained at grade 1 in 6 of the 8 patients. During surgery for lateral-widespread lesions, it is difficult to fix and stabilize the fragment of the lateral margin of the capitellum. For this reason, several authors have reported that the lateral-widespread type may be predictive of a poor prognosis in a variety of procedures. In a retrospective case series in which 8 of 32 patients with a lateral-widespread lesion underwent osteochondral peg fixation, 4 of the 8 had to undergo a second surgical procedure. 8 Mihara et al 12 performed drilling, fragment fixation, and removal of the detached fragment with drilling on 27 patients with advanced-stage OCD lesions, reporting that 4 of 27 patients assessed with >70% flattening of the capitellum or degenerative changes on final radiographs showed a large lesion extending from the lateral margin to the center of the capitellum preoperatively.
The following reason could explain why fragments of the lateral margin of the capitellum contain a small amount of bone 25 and why blood circulation in the outermost portion of the capitellum is very poor during childhood. 4 When the lateral margin of the capitellum is insufficiently remodeled, contact pressure in the radiocapitellar joint is greater with a lateral defect than with a central defect under valgus torque, 14 and enlargement or deformity of the radial head occurs through adaptation. 12 As a result, cartilage fragments come apart and progress to osteoarthritic changes or free bodies. Our results showed that 6 of the 9 patients with a lateral-widespread lesion attained excellent or good healing. We noted that healing of lesions with osteoarthritic changes preoperatively was worse than in lesions without osteoarthritic changes. This finding indicates that it is important to perform closed-wedge osteotomy for patients with lateral-widespread lesions before osteoarthritic changes occur.
To the best of our knowledge, no report has described the influence of a surgical procedure on the physis. If patients with an open capitellar physis undergo closed-wedge osteotomy, the osteotomy site crosses the capitellar physis similar to a fracture of the lateral humeral condyle. In other words, we artificially create a fracture of the lateral humeral condyle and perform osteosynthesis. Common abnormalities of growth after a fracture of the lateral condyle include overgrowth of the lateral condyle, a fishtail deformity, and formation of a metaphyseal-epiphyseal cross-bridge. 16,19 In this study, no excessive deformity of the distal humerus was observed.
Several factors may have contributed to this finding. First, the incidence of cross-bridging of the epiphyseal cartilage is rare after fractures of the lateral condyle. 16 Similarly, if the osteotomy site passes an open capitellar physis, we believe that cross-bridging is less likely to occur after closed-wedge osteotomy. Second, we speculate that there is a relationship between bone age at the time of surgery and the timing of capitellar physis closing. The physis between the ossific nucleus in the capitellum and the metaphyseal bone becomes uniformly narrow by the age of 10 years, although bony fusion does not occur until 12 years at the earliest. At 13 years, the cartilaginous line has usually disappeared, and between 14 and 16 years, this is regularly the case. 4 In addition, the epiphyseal closure progresses earlier on the affected side because of the influence of OCD 10,27 and osteotomy. For those reasons, we think that an excessive deformity of the distal humerus will not occur even if the osteotomy line crosses the capitellar physis.
The limitations of the current study include its retrospective nature and the small number of patients evaluated, which could cause potential patient selection or reviewer bias. The follow-up rate was low. We asked the patients to cooperate in the survey through letters and telephone calls, but many patients did not participate because of relocation or interrupted communication. High rates of degenerative joint disease and residual elbow symptoms after OCD of the elbow treated conservatively and with surgical treatment have been observed after long-term follow-up 2,22 ; however, the minimum follow-up period in our study was 2 years. Particularly when considering how young these patients were at the time of surgery, we consider that a longer follow-up period is needed in future research.
Conclusion
Closed-wedge osteotomy for advanced-stage OCD of the capitellum in young patients can provide satisfactory clinical and radiological results. Poorer outcomes were seen in cases with lesions of the lateral-widespread type and preoperative degenerative changes in the elbow joint. It is important to perform the operative procedure early, regardless of the condition of the capitellar physis, if OCD of the capitellum is in an advanced stage.
Footnotes
Acknowledgment
The authors thank Akiyoshi Yamazaki, MD, and Munenori Matsueda, MD, for providing assistance with the data collection.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics committee of Niigata Central Hospital.