
Abstract
Background:
The surgical management of chronic lateral ankle instability (CLAI) has evolved since the 1930s, but for the past 50 years, the modified Broström technique of ligament repair has been the gold standard. However, with the development of arthroscopic techniques, significant variation remains regarding when and how CLAI is treated operatively, which graft is the optimal choice, and which other controversial factors should be considered.
Purpose:
To develop clinical guidelines on the surgical treatment of CLAI and provide standardized guidelines for indications, surgical techniques, rehabilitation strategies, and assessment measures for patients with CLAI.
Study Design:
A consensus statement of the Chinese Society of Sports Medicine.
Methods:
A total of 14 physicians were queried for their input on guidelines for the surgical management of CLAI. After 9 clinical topics were proposed, a comprehensive systematic search of the literature published since 1980 was performed for each topic through use of China Biology Medicine (CBM), China National Knowledge Infrastructure (CNKI), PubMed, Web of Science, EMBASE, and the Cochrane Library. The recommendations and statements were drafted, discussed, and finalized by all authors. The recommendations were graded as grade 1 (strong) or 2 (weak) based on the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) concept. Based on the input from 28 external specialists independent from the authors, the clinical guidelines were modified and finalized.
Results:
A total of 9 topics were covered with regard to the following clinical areas: surgical indications, surgical techniques, whether to address intra-articular lesions, rehabilitation strategies, and assessments. Among the 9 topics, 6 recommendations were rated as strong and 3 recommendations were rated as weak. Each topic included a statement about how the recommendation was graded.
Conclusion:
This guideline provides recommendations for the surgical management of CLAI based on the evidence. We believe that this guideline will provide a useful tool for physicians in the decision-making process for the surgical treatment of patients with CLAI.
Ankle sprain is one of the most frequently encountered injuries during sporting activity, 1,173 and up to 85% of patients sustain lateral ligament injury. Reports indicate that 34% to 70% of patients may continue to experience persistent symptoms of pain, swelling, or a feeling of instability. 192,193,231 Among these patients, chronic lateral ligament instability is one of the primary causes of symptoms. In addition, up to 93% of patients present with intra-articular lesions. 72,101,183,193
Chronic lateral ankle instability (CLAI) is defined as recurrent sprains or repeated “giving way” resulting from trauma for at least 1 year. 61,66 Giving way is considered an uncontrolled or unpredictable excessive inversion of the ankle joints that occurs at heel strike or toe-off during walking or running. 61 CLAI can be further subcategorized into functional ankle instability (FAI) and mechanical ankle instability (MAI). FAI affects patients with symptoms of instability but cannot be assessed by physical examination. Furthermore, it is believed that FAI results from a neuromuscular deficit, and this condition is commonly treated with nonsurgical therapies, including phased peroneal firing and proprioception exercises. In contrast, MAI typically demonstrates positive results for the anterior drawer test or stress radiography. 66 Patients with MAI typically require surgical treatment if physical therapy has failed. 66,91
The surgical treatment for CLAI began with a nonanatomic reconstruction by Nilsonne in 1932, 150 followed by other nonanatomic operations such as the Watson-Jones, 208 Evans, 55 and Chrisman-Snook 37 procedures. Despite excellent short-term results, nonanatomic reconstruction has been implicated in alteration of kinematics of the ankle and subtalar joint and has been associated with subsequent posterior facet arthritis of the subtalar joint, laxity of the graft, and poor postoperative functional recovery. 65,87,89,176 Therefore, anatomic repair was proposed by Broström in 1966 14 and modified by Gould et al 59 in 1980. Since that time, this combination has been regarded as the gold standard with which all other techniques are compared. 59,158 Anatomic ligament repair restores near-normal anatomic characteristics and joint mechanics by repairing the ligament remnants. 18,100 Recently, arthroscopic anatomic repair and reconstruction of the ankle lateral ligaments have gained popularity among many surgeons. 62,63,114,138,146 Arthroscopic lateral stability surgery can entail an anatomic repair, but the early procedures were more reliant on nonanatomic imbrication of the soft tissue, which had the potential to alter the kinematics of the hindfoot. 172 Thus, the decision to consider an arthroscopic repair compared with an open repair involves many considerations and factors. The decision must also weigh the option to address intra-articular abnormality, the choice of autograft or allograft, rehabilitation protocols, and the time lost for athletes.
To date, no consensus exists regarding the correct decision-making paradigm for CLAI. The aim of this guideline is to assist physicians in making the most appropriate treatment decisions based on the best available evidence and to categorize that evidence based on the strength of recommendation criteria.
Methods
The present guideline is proposed to be used in patients aged 16 to 60 years with CLAI.
General Outline of the Process
The process began in July 2017. A total of 9 topics regarding indication, surgical technique, rehabilitation, return to sporting activities, and assessment of outcomes were proposed. Comprehensive systematic searches of the related literature published since 1980 were performed for each topic, and a draft of the guideline statement on the recommendations was prepared. The draft was reviewed, modified, and finalized by all the authors listed on this consensus statement. Then, the evidence level and grading of the recommendations were determined at a consensus meeting in May 2018, when the recommendations were discussed and modified by 20 national surgeons, 1 epidemiologist, and 1 nurse (all of whom were experienced in the treatment of CLAI), until 70% agreement was met. Finally, the guidelines were modified and finalized by 28 external specialists independent from the authors who assessed the final drafts.
Method of Systematic Literature Review
A systematic review of each topic was carried out through use of China Biology Medicine (CBM), China National Knowledge Infrastructure (CNKI), PubMed, Web of Science, EMBASE, and the Cochrane Library. The main search terms were (lateral ankle ligament OR ankle instability) plus a specific term for each topic. Studies were included if they extracted risk-benefit outcomes from each topic. Studies were excluded if they were nonclinical studies, reviews, or study protocols. The information from each included paper was summarized, such as the design of the study and the risk of bias of the study, through use of the Cochrane Handbook for Systematic Reviews of Interventions 39 and the Newcastle-Ottawa scale for assessing nonrandomized studies. 147
Determination of Evidence Level and Grading of Recommendations
The grading of recommendations was determined based on the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach. 5 Randomized controlled trials (RCTs) were regarded as having a high level of evidence, observational studies were considered to have a low level of evidence, and case reports and expert opinions were thought to have the lowest level of evidence.
Assessment of the presence or absence of factors that decrease evidence levels included the following:
Limitations of study design
Inconsistent results
Indirect evidence
Inaccurate data
High probability of publication bias
Assessment of the presence or absence of factors that increase evidence levels included the following: Profound effects with no confounders Dose-response gradient Possible confounders that diminish actual effects
The final level of evidence was graded from A (highest) to D (lowest). The strength of recommendations was decided with consideration of the following factors: the balance between benefits and harm, quality of evidence, patient values and preferences, and medical costs (Table 1). Therefore, 1A indicates high-quality evidence with a strong recommendation, and 2D indicates very low–quality evidence with a weak recommendation.
Definition of GRADE Strength of Recommendations a

a GRADE, Grading of Recommendations Assessment, Development, and Evaluation.
Notes on Using the Guideline
This guideline is based on evidence of relatively general and standard practices for CLAI, especially for patients with MAI. However, surgeons can treat individual CLAI patients without compromising this guideline.
Results and Discussion
Surgical Recommendations for CLAI
When Should CLAI Be Treated Surgically?
Recommendation
When (1) patients exhibit symptoms of CLAI after 3 to 6 months of nonsurgical treatment; (2) physical examination reveals tenderness around the lateral ligaments or a positive anterior drawer test or talar tilt test; (3) the diagnosis of CLAI was also confirmed by stress radiography or magnetic resonance imaging (MRI), surgery is suggested (2C).
Statement
No comparative studies of nonsurgical versus surgical treatment for CLAI or studies directly regarding surgical indication for CLAI were found. Studies on clinical treatment for CLAI were searched, and those with levels of evidence (LOE) 1 through 3 were included. In-depth analysis of the inclusion criteria for surgical patients in each study was conducted to obtain surgical indications that were widely recognized by researchers. According to this search strategy, a total of 14 studies were included, §§ of which 2 studies were LOE 1, 99,229 3 studies were LOE 2, 69,126,143 and 9 studies were LOE 3. ∥∥ Among them, the most frequently presented surgical indications for CLAI were as follows: patients had symptoms of ankle instability after trauma, such as pain, giving way, recurrent ankle twisting, and limited sports or physical activity (14 studies), and preoperative physical examinations were necessary (ie, surgical indications should be supported by corresponding physical signs) (14 studies). Physical examinations included local tenderness of the injured ligament, positive anterior drawer test, or positive talar tilt test. All studies noted that preoperative imaging tests were routine examinations; that is, surgical indications should be supported by corresponding imaging results. Stress radiography and MRI were the most commonly used adjuvant examinations; 3 studies used stress ultrasound testing. 34,114,126 Patients underwent routine conservative treatment before surgery in all studies, including use of brace protection and training for proprioception, ankle valgus muscle strength, and ankle joint range of motion. However, the duration of conservative treatment differed: 9 studies clearly indicated that conservative treatment was required for longer than 6 months, ¶¶ among which 2 studies were LOE 1, 3 studies were LOE 2, and 4 studies were LOE 3. Another 2 studies of LOE 3 clearly indicated that conservative treatment was essential for longer than 3 months (Table 2). 34,167 In the future, controlled study on nonsurgical versus surgical treatment for CLAI will be needed to further determine the surgical indications.
Brief Description of Included Studies a

a LOE, level of evidence.
Do CLAI and Osteochondral Lesions Need to Be Addressed Simultaneously During Surgery?
Recommendation
Management of osteochondral lesions (OCLs) of the talus or tibia and simultaneously torn lateral ankle ligaments in patients with CLAI could alleviate symptoms, and the short-term clinical outcomes are good postoperatively, so surgery of both lesions simultaneously should be a safe and reliable treatment strategy (2C).
Statement
Normally, patients with CLAI should be immobilized for 3 to 4 weeks postoperatively. However, patients with combined CLAI and OCL who are treated with a bone marrow stimulation procedure should begin passive ankle movement at an early stage after surgery. This poses a contradiction in rehabilitation protocols when cartilage and ligament surgery are performed simultaneously, which may have adverse effects on patient outcomes. Currently, it is recommended that OCLs be addressed first, and then open or arthroscopic anatomic repair or reconstruction of the ligaments should be performed. However, many retrospective cohort studies ## reported no significant difference in short-term follow-up in terms of American Orthopaedic Foot & Ankle Society (AOFAS), visual analog scale (VAS), Karlsson, or Tegner scores between isolated CLAI and CLAI combined with OCLs when these conditions were treated simultaneously, which may indicate the safety and effectiveness of addressing CLAI and OCLs at the same time. Gregush and Ferkel 60 reported promising outcomes after long-term follow-up (mean, 7.3 years) of simultaneous arthroscopic treatment of an OCL of the talus and open lateral ankle stabilization. However, larger sample sizes and prospective study designs should be used to provide firm information regarding long-term results.
Open Versus Arthroscopic Anatomic Repair for CLAI—Which Procedure Is Better?
Recommendation
Patients undergoing either procedure can be expected to experience equivalent short-term functional outcomes (1B).
Statement
Yeo et al 229 performed an RCT to compare arthroscopic repair (n = 25) with open repair (n = 23) for CLAI. After 12 months postoperatively, the AOFAS, VAS, and Karlsson scores were improved significantly in both groups (P < .001). However, no statistically significant difference was found between groups with regard to AOFAS, VAS, and Karlsson scores (P = .736, .577, and .5, respectively) or radiologic outcomes, including the anterior talar translation and talar tilt angle (P = .39 and .436, respectively). Li et al 114 conducted a cohort study (n = 60) to assess the effectiveness of open (n = 37) and arthroscopic (n = 23) procedures for CLAI. Both groups showed significant improvement in AOFAS, Karlsson, and Tegner activity scores (P < .001) at the final follow-up. However, no significant difference was noted in these outcomes between groups postoperatively. Rigby and Cottom 162 demonstrated similar outcomes, with no statistically significant difference (P > .05) between the open (n = 32) and arthroscopic (n = 30) groups with regard to AOFAS, Karlsson, or VAS scores pre- and postoperatively. Matsui et al 138 evaluated the functional outcomes between arthroscopic (n = 19) and open (n = 18) repair of CLAI before and at 12 months after surgery. Scores on the Japanese Society for Surgery of the Foot (JSSF) scale significantly improved from 69.9 to 98.0 in the arthroscopic group and from 70.8 to 95.4 in the open group (P < .01). In addition, the talar tilt angle and displacement of the talus on stress radiography were significantly improved postoperatively in both groups (P < .01). However, no significant difference was found in the assessment scores or ankle stability tests between groups. Unique to this study was the fact that the authors evaluated the duration of surgery and time to return to daily activity, which were both significantly shorter in the arthroscopic group (P < .05), while it remained inconclusive whether arthroscopic anterior tibiofibular ligament (ATFL) repair enabled early recovery (Table 3). In contrast, a systematic review 50 demonstrated that athletes treated with open ankle ligament repair procedures (167 athletes) returned to play almost 1 month earlier than athletes treated with arthroscopic procedures (19 athletes); however, because the sample sizes between groups were not comparative, more studies should be performed to make a firm conclusion.
Characteristics of Included Studies a
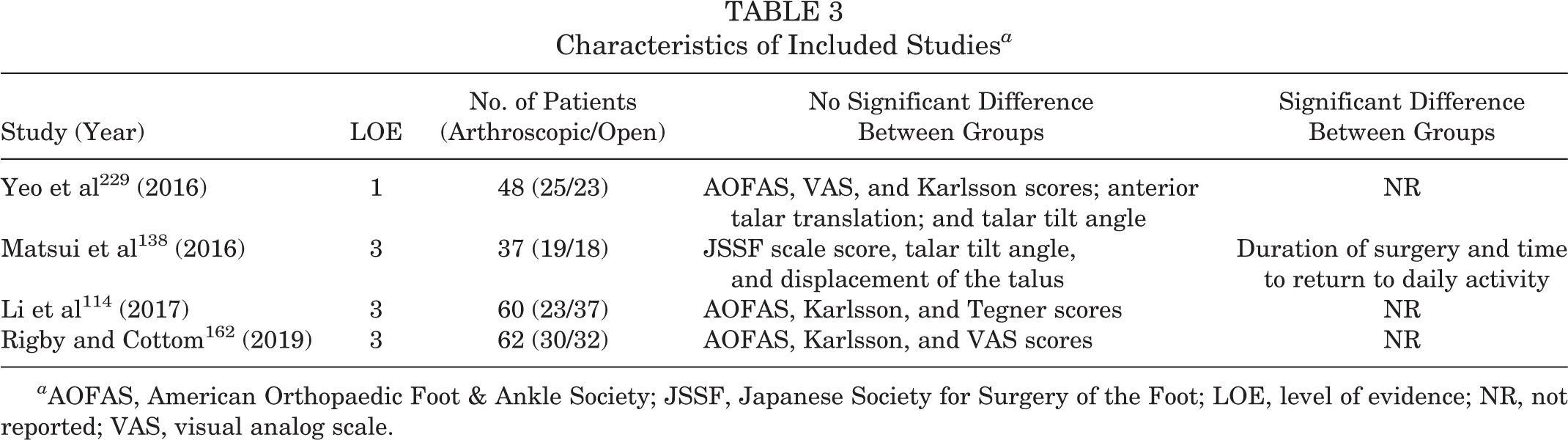
a AOFAS, American Orthopaedic Foot & Ankle Society; JSSF, Japanese Society for Surgery of the Foot; LOE, level of evidence; NR, not reported; VAS, visual analog scale.
Open Versus Arthroscopic Anatomic Reconstruction for CLAI—Which Procedure Is Better?
Recommendation
Patients undergoing either procedure can expect to experience equivalent short-term functional outcomes (1C).
Statement
No comparative study between open and arthroscopic reconstruction for CLAI is available. Youn et al 234 reported that VAS score, Karlsson score, anterior talar translation, and talar tilt angle significantly improved after arthroscopic reconstruction of the ATFL and calcaneofibular ligament (CFL). Another 6 studies 73,77,85,200,206,217 described similar results with regard to Karlsson score, anterior talar translation, and talar tilt angle when open anatomic reconstruction was performed. These findings indicate that patients undergoing either open or arthroscopic procedures can be expected to experience equivalent short-term functional outcomes.
Autograft Versus Allograft After Anatomic Reconstruction for CLAI—Which Graft Is Better?
Recommendation
Neither type of graft has superiority over the other. Either autograft or allograft can be considered a promising candidate for anatomic reconstruction (1C).
Statement
In 5 comparative studies 117,135,217,222,241 (n = 262), 132 patients received autograft reconstruction and 130 patients had allograft procedures. Among them, 4 studies 117,135,217,241 analyzed the preoperative and postoperative outcomes of reconstruction with autografts and allografts, which all demonstrated good clinical results at the final follow-up; however, no significant difference was found between the 2 groups for AOFAS score, Karlsson score, VAS score, anterior talar translation, or talar tilt angle.
Is It Necessary to Reconstruct the Calcaneofibular Ligament?
Recommendation
When patients with CLAI have subtalar joint instability and both the ATFL and CFL are ruptured, ATFL and CFL reconstruction should be taken into consideration (2C).
Statement
In the study by Okuda et al 152 in which ATFL reconstruction (n = 11) was compared with ATFL and CFL reconstruction (n = 16), anterior talar translation and talar tilt angle were significantly improved after surgery (P < .001), but no difference was observed between groups at final follow-up. However, 6 of 27 patients did not reach 90 on the Hamilton score, which was related to subtalar joint instability, in the authors’ opinion. Maffulli et al 133 noted that patients (n = 38) showed remarkable improvement in AOFAS and Kaikkonen scores (P < .001) after isolated ATFL reconstruction. However, 10 patients with subtalar joint instability continued to have recurrent sprains and pain. This result indicates that ATFL and CFL reconstruction is suggested if patients with subtalar joint instability have ATFL and CFL rupture.
Rehabilitation: When to Start Range of Motion and Weightbearing Exercises?
Recommendation
For patients who undergo anatomic repair or reconstruction, range of motion (ROM) (mostly dorsiflexion) and partial weightbearing with a brace are encouraged from the second day after surgery. For patients with OCL who undergo anatomic repair or reconstruction and additional microfracture, early ROM is advised to avoid the limitation of joint mobility, while weightbearing should be relatively delayed (1C).
Statement
In the study by Miyamoto et al, 141 18 patients started ankle ROM and muscle training 2 days after ATFL reconstruction, while the other 15 patients began this regimen 1 month after the same procedure. No significant difference was found in the Karlsson score, Peterson score, anterior talar translation, or talar tilt angle. However, the time to return to sports was significantly shorter (P < .01) in the aggressive rehabilitation group (13.4 weeks) than in the traditional rehabilitation group (18.5 weeks). Jiang et al 81 studied patients with OCL following anatomic repair (n = 34) who started passive ROM exercises at 2 weeks and weightbearing at 8 weeks postoperatively, while patients with isolated CLAI (n = 36) began ROM exercises at 3 weeks and weightbearing at 4 weeks after surgery. No significant difference was found in VAS, AOFAS, or Tegner scores between groups. With regard to the limitation of ankle movement, patients with OCL (23.5%) were remarkably more likely to have limited movement than were the patients with isolated CLAI (5.6%) (P < .05). The authors explained that this might result from more bleeding and synovial reactive hyperplasia when addressing the OCL, causing adhesion of the joint. Therefore, patients with OCL are recommended to start rehabilitation at an early phase.
What Measurements Should Be Used as Criteria for Return to Sports?
Recommendation
Joint stability, muscle strength, and full ROM are important indicators in terms of returning to sports after surgery (1C).
Statement
In 6 studies, 28,29,31,32,92,93 the investigators considered joint stability to be an important parameter, measured by methods such as physical examination and anterior talar translation. Further, 4 studies 90,93,102,136 demonstrated that muscle strength should be recovered to 90% to 100% of the unaffected limb. Of these, 3 studies 92,93,102 described using full ankle ROM as an assessment for return to sports. In a review, Hunt et al 75 found that a considerable number of published studies used patient-reported outcomes for clinical measurement but very few used return to sports as a reported outcome metric. Further studies on outcomes following ankle stabilization should include clear and consistent metrics for return to sport and level of play.
Assessment of Outcomes for CLAI
Recommendation
The measurement most commonly used by clinicians is the AOFAS score, followed by the Karlsson score, and the evaluations most commonly used by patients are the VAS score and Foot and Ankle Ability Measure (FAAM) scale. The most commonly used objective assessments are the talus tilt test and the anterior drawer stress radiograph (1C).
Statement
A total of 197 studies (137 in English a and 60 in Chinese b ) were included and screened. Of them, 134 studies (76 in English c and 58 in Chinese d ) used the AOFAS score (68%), 62 studies (55 in English e and 7 in Chinese f ) used the Karlsson score (31.4%), 38 studies (25 in English g and 13 in Chinese h ) used the VAS score (19.2%), and 11 studies (11 in English i and 0 in Chinese) used the FAAM score (5.6%). Regarding objective measurements, the talus tilt test and anterior drawer stress radiography are the most commonly used assessments. However, it is difficult to recommend an evaluation based on statistical frequency in clinical practice, and physicians should make decisions on specific cases accordingly.
Conclusion
This guideline presents the most standard surgical management strategies for CLAI at the current time and will be revised every 5 years. We believe it will be helpful for surgeons to make evidence-based decisions when treating patients with CLAI surgically. Meanwhile, we expect this guideline to assist physicians and researchers in designing future studies according to the current understanding of operative treatment for CLAI.
The main recommendations are as follows: Surgery is suggested when patients continue to have symptoms of CLAI after 3 to 6 months of nonsurgical treatment and have indications of CLAI on physical and imaging examinations (stress radiography or MRI). Simultaneous surgery for CLAI and OCL lesions of the talus or tibia is suggested when both are present. Open and arthroscopic procedures are both recommended in patients with CLAI who undergo anatomic repair or reconstruction. Autograft and allograft are both recommended for anatomic reconstruction in patients with CLAI. When patients with CLAI have subtalar joint instability and both the ATFL and the CFL are ruptured, ATFL and CFL reconstruction is suggested. For patients with CLAI who undergo anatomic repair or reconstruction, ROM (mostly dorsiflexion) and partial weightbearing with a brace from the second day after surgery are recommended; for those with OCL who undergo anatomic repair or reconstruction and additional microfracture, early ROM and relatively delayed weightbearing are recommended. Joint stability, muscle strength, and full ROM are recommended prior to returning to sport after surgery. The AOFAS score, Karlsson score, VAS score, FAAM scale, talus tilt test, and anterior drawer stress radiographs are recommended to assess CLAI.
Footnotes
Acknowledgments
This guideline was reviewed by the following: Bin Cai, MD (Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University, Shanghai, China); Christopher D. Murawski, MD (School of Medicine, University of Pittsburgh, Pittsburgh, Pennsylvania, USA); Dong Jiang, MD (Peking University Third Hospital, Beijing, China); Fei Chang, MD (Second Affiliated Hospital of Jilin University, Changchun, China); Guangrong Yu, MD (Tongji Hospital, Tongji University, Shanghai, China); Jiazhang Huang, MD (Huashan Hospital, Fudan University, Shanghai, China); Jin Woo Lee, MD (Yonsei University College of Medicine, Seoul, Republic of Korea); John G. Kennedy, MD (Hospital for Special Surgery, New York, New York, USA); Hailin Xu, MD (Beijing University People’s Hospital, Beijing, China); Huanghe Song, MD (First Affiliated Hospital of Nanjing Medical University, Nanjing, China); Kowk Bill Chan, MD (Virtus Medical Group, Hong Kong, China); Kehe Yu, MD (Second Affiliated Hospital of Wenzhou Medical University, Wenzhou, China); Masato Takao, MD (Clinical and Research Institute for Foot & Ankle Surgery, Tokyo, Japan); Mingzhu Zhang, MD (Beijing Tongren Hospital, Beijing, China); Niek C. van Dijk, MD (Academic Medical Center, University of Amsterdam, Amsterdam, the Netherlands); Pieter D’Hooghe, MD (Aspetar Hospital, Doha, Qatar); Richard D. Ferkel, MD (Southern California Orthopedic Institute, Van Nuys, California, USA); Siu Wah Kong, MD (Asia Medical Specialists, Hong Kong, China); Stephane Guillo, MD (Centre for Orthopaedic Sports Surgery, Bordeaux-Mérignac, France); Tun Hing Lui, MD (North District Hospital, Hong Kong, China); Xiaofan Dou, MD (Zhejiang Provincial People’s Hospital, Hangzhou, China); Xiaohui Gu, MD (Zhejiang Provincial People’s Hospital, Hangzhou, China); Xin Ma, MD (Huashan Hospital, Fudan University, Shanghai, China); Xu Tao, MD (Southwest Hospital, Army Medical University, Chongqing, China); Yasuhito Tanaka, MD (Department of Orthopedic Surgery, Nara Medical University, Nara, Japan); Yuan Zhu, MD (Ruijin Hospital, Shanghai Jiao Tong University, Shanghai, China); Zhengyi Wang, MD (Third Affiliated Hospital, Beijing University of Chinese Medicine, Beijing, China); Zhi Wang, MD (Beijing Tongren Hospital, Beijing, China).
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.