
Abstract
Background:
Transtibial pull-out repair of the medial meniscal posterior root (MMPR) has been largely assessed through biomechanical studies. Biomechanically comparing different suture types would further optimize MMPR fixation and affect clinical care.
Purpose/Hypothesis:
The purpose of this study was to determine the optimal suture material for MMPR fixation. It was hypothesized that ultra high–molecular weight polyethylene (UHMWPE) suture tape would be biomechanically superior to UHMWPE suture and standard suture.
Study Design:
Controlled laboratory study.
Methods:
The MMPR attachment was divided in 24 human cadaveric knees and randomly assigned to 3 repair groups: UHMWPE suture tape, UHMWPE suture, and standard suture. Specimens were dissected down to the medial meniscus, and the posterior root attachments were sectioned off the tibia. Two-tunnel transtibial pull-out repair with 2 sutures, as determined by the testing group, was performed. The repair constructs were cyclically loaded between 10 and 30 N at 0.5 Hz for 1000 cycles to mimic the forces experienced on the medial meniscus during postoperative rehabilitation. Displacement was recorded at 1, 50, 100, 500, and 1000 cycles. Ultimate failure load, displacement at failure, and load at 3 mm of displacement (clinical failure) were also recorded.
Results:
UHMWPE suture tape had significantly less displacement of the medial meniscus when compared with standard suture at 1 (–0.22 mm [95% CI, –0.41 to –0.02]; P = .025) and 50 (–0.35 mm [95% CI, –0.67 to –0.03]; P = .029) cycles. There were no other significant differences observed in displacement between groups at any number of cycles. UHMWPE suture tape had significantly less displacement at the time of failure than standard suture (–3.71 mm [95% CI, –7.17 to –0.24]; P = .034). UHMWPE suture tape had a significantly higher load to reach the clinical failure displacement of 3 mm than UHMWPE suture (15.64 N [95% CI, 0.02 to 31.26]; P = .05). There were no significant differences in ultimate failure load between groups.
Conclusion:
The meniscal root repair construct with UHMWPE suture tape may be stronger and less prone to displacement than that with standard suture or UHMWPE suture.
Clinical Relevance:
UHMWPE suture tape may provide better clinical results compared with UHMWPE suture and standard suture.
The orthopaedic literature has recently recognized the importance of anatomic repair of medial meniscal posterior root (MMPR) tears based on several biomechanical and clinical studies. 1,4,9,12 These studies have changed the treatment paradigm regarding meniscal root tears, resulting in the recommendation to repair meniscal root tears in patients with no to low-grade osteoarthritis. 5,6,19,24
Feucht et al 8 performed a systematic review on transtibial pullout for MMPR tears and observed that despite improved postoperative clinical outcomes, the healing status based on magnetic resonance imaging and second-look arthroscopic surgery was classified as complete in 62% of patients, partial in 34%, and failed in 10%. LaPrade et al 17 reported failure and the subsequent need for revision surgery in 9.7% of patients who underwent an index transtibial pull-out technique for medial meniscal root repair. These failures warrant the need to enhance the results of MMPR repair.
The transtibial pull-out repair technique of MMPR tears has emerged as a common method of anatomic fixation; however, the optimal method for meniscal root repair has yet to be determined. 16 Through biomechanical studies, the number of transtibial tunnels, the number of sutures, the suture configuration, and the location of sutures have been assessed to determine the most optimal method of repair. 11,13 –15,22 A recent systematic review evaluating the biomechanical properties of meniscal posterior root repair affirmed that there is currently no consensus regarding the superiority of a single suture material or shape. 11
It has been previously suggested that suture strength is important to the success of root repair. 3 Because the differences in suture materials range from braided polyester to ultra high–molecular weight polyethylene (UHMWPE), the material strength of suture may ultimately affect the overall strength of the repair construct. Also, it has been theorized that a wider suture material, such as suture tapes, could fill the hole created for the passage of the suture through the tissue and better distribute forces to avoid suture cutout, possibly reducing the common risk of recurrent displacement after meniscal root repair. 7
Therefore, the purpose of this study was to biomechanically determine the optimal suture material for MMPR fixation. Three suture materials were chosen for comparison based on suture composition and suture caliber/width to assess the effect of these differences. It was hypothesized that suture tape, composed of UHMWPE, would be biomechanically superior to suture composed of UHMWPE or well as standard braided polyester suture.
Methods
Twenty-four unpaired, fresh-frozen, male human cadaveric knee specimens (mean age, 51.6 years; range, 23-65 years) were used for this study. The cadaveric specimens used in this study were donated to registered tissue banks for the purpose of medical research and then purchased by our institution with a Smith & Nephew donation. The use of cadaveric specimens for research does not require institutional review board approval at the authors’ institution. Specimens were stored at –20°C and thawed to room temperature 24 hours before testing. The knees were carefully examined after dissection to ensure ligamentous and meniscal integrity and the absence of degenerative intra-articular disease. All knees were dissected free of skin. The patella and femur were disarticulated from the knee by dividing the cruciate and collateral ligaments, and the fibula was excised from the tibia. Next, each tibia was potted with poly(methyl methacrylate) (Fricke Dental International) in a cylindrical mold up to a point approximately 4 cm distal to the most proximal aspect of the tibial tuberosity.
Surgical Procedure
Eight knees were randomly assigned to each of the 3 repair groups: (1) nonabsorbable UHMWPE suture tape (ULTRATAPE; Smith & Nephew), (2) braided nonabsorbable UHMWPE suture (No. 2 ULTRABRAID; Smith & Nephew), and (3) braided nonabsorbable polyester standard suture (No. 0 ETHIBOND; Ethicon). We chose to test the conventional No. 0 ETHIBOND suture because of its low cost compared with ULTRABRAID suture and to assess the narrower gauge effect on meniscal tissue cutout.
The MMPR direct attachment and shiny white fibers were sharply dissected from their attachment sites. Two-tunnel transtibial pull-out meniscal root repair was performed in each knee using the allocated suture material for each group. Two sutures were placed in a vertical, simple suture configuration. 14 The tibial guide was set at a 45° angle, and the entry points of the tunnels were placed 3 cm below the anteromedial tibial plateau, midway between the tibial tubercle and medial collateral ligament. All transtibial repair tunnels were placed through the root attachment at an average 9.6 mm posterior and 0.7 mm lateral to the apex of the medial tibial eminence. The size of the transtibial tunnels was the same for all constructs (2.4-mm), which were drilled with the assistance of a guide and drill sheath (Smith & Nephew). It was possible to pass all types of sutures evaluated in this study in this tunnel size (2.4 mm), which is commonly used for No. 2 suture. 14
Two sutures of each randomized testing suture type were passed through the meniscus using a suture passer with a 19-gauge needle (FIRSTPASS MINI; Smith & Nephew), 7 mm from the transition zone of the meniscus. The posterior suture was placed 3 mm from the meniscocapsular junction in the red-red zone, and the anterior suture was placed 2 mm anterior to the posterior suture in the red-white zone. 13 With the assistance of a looped monofilament suture, the anterior suture was shuttled through the anterior tunnel, and the posterior suture was shuttled through the posterior tunnel. The sutures were manually tensioned and tied using a surgeon’s knot, followed by 5 half-hitches on alternating posts over a 4 × 12–mm surgical fixation button (ENDOBUTTON; Smith & Nephew) at the aperture of the transtibial tunnel in the anteromedial cortex of the tibia. The procedures were standardized and performed by 2 experienced orthopaedic surgeons (G.Y.N., M.J.S.). Surgical repair with UHMWPE suture tape is represented in Figure 1.

Medial meniscal posterior root repair with ultra high–molecular weight polyethylene (UHMWPE) suture tape in a right knee. (A) Superior view of UHMWPE suture tape passed through the meniscal root. (B) Superoposterior view of anatomic medial meniscal posterior root repair. (C) Medial view of the proximal tibia showing UHMWPE suture tape tied over the cortical fixation button.
Biomechanical Testing
Next, the medial meniscus was sectioned 3 cm from its posterior root attachment site. The posterior horn of the meniscus was clamped 1 cm medial to the location of the passed sutures by a custom clamp attached to the actuator of the dynamic tensile testing machine (ElectroPuls E10000; Instron). Metal wire was wrapped through the body of the meniscus and secured by the clamp with custom manufactured teeth to avoid slippage during testing as performed in previous studies. 3,14,15 The load vector was then aligned with the meniscal root circumferential fibers and parallel to the medial tibial plateau to best simulate the physiological hoop stresses of the posterior horn (Figure 2). The meniscus was preconditioned for 10 cycles from 1 to 10 N at 0.1 Hz. After preconditioning, the meniscus was cyclically loaded for 1000 cycles from 10 to 30 N at 0.5 Hz. Displacement at the completion of 1, 50, 100, 500, and 1000 cycles was recorded. This loading protocol has been used previously to approximate tensile forces in a postoperative rehabilitation regimen after meniscal root repair. 3 The meniscus was subsequently pulled to failure at a rate of 30 mm/min, and ultimate failure load and displacement were recorded. 3 Additionally, the load at clinical failure (3 mm of displacement) was recorded. 15,25 Clinical failure was defined based on a previous biomechanical study that reported that 3 mm of displacement is the threshold to compromise meniscal function in a porcine model. 25

Testing of the medial meniscal posterior root repair construct in a left knee. (A) Superior view of the tibial plateau. (B) Superoanterior view of the tibial plateau.
Statistical Analysis
The primary aim of this study was to compare cyclic displacement and load to failure for the 3 suture types used in this study for meniscal root repair. Parametric analysis of variance with Tukey pairwise post hoc comparison was performed. P values <.05 were considered statistically significant. All analyses and plots were produced using the statistical programming language R version 3.5.0. 20
Results
Cyclic Displacement
The displacement recorded for each of the groups tested after the completion of 1, 50, 100, 500, and 1000 cycles (after meniscus preconditioning) is presented in Figure 3. All suture groups showed the progression of displacement with an increase in cycles. UHMWPE suture tape had significantly less displacement of the medial meniscus when compared with standard suture at 1 (–0.22 mm [95% CI, –0.41 to –0.02]; P = .025) and 50 cycles (–0.35 mm [95% CI, –0.67 to –0.03]; P = .029). There were no other significant differences in displacement detected between suture groups.
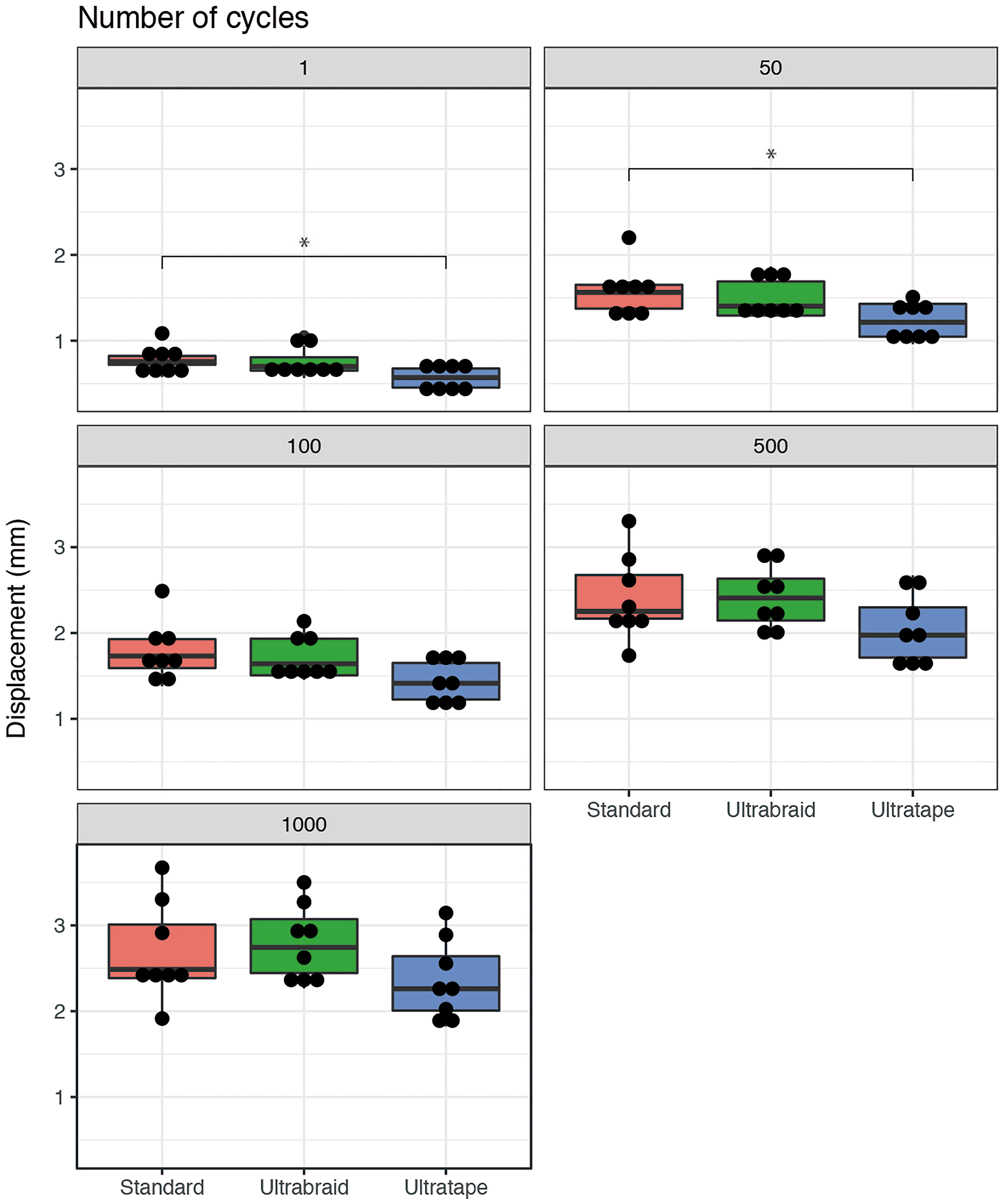
Cyclic displacement of different suture materials for transtibial pull-out repair of medial meniscal posterior root tears. Dots represent individual specimen observations. Thick horizontal lines represent group medians, while top and bottom sections of the boxes represent the 25th and 75th percentiles, respectively. *Statistically significant difference.
Ultimate Failure Load
There were no significant differences in ultimate failure load observed between groups (Figure 4). Suture cutout of the meniscus was the most common mechanism of failure, occurring in all repair constructs using 2-mm UHMWPE suture tape and No. 2 UHMWPE suture and 6 of 8 (75%) specimens in the standard suture group. Two specimens in the standard suture group failed by suture breakage.

Boxplot comparing ultimate failure load (N) between suture type groups. Dots represent individual specimen observations. Thick horizontal lines represent group medians, while top and bottom sections of the boxes represent the 25th and 75th percentiles, respectively.
Displacement at Failure
The UHMWPE suture tape group had significantly less displacement at the time of failure than the standard suture group (–3.71 mm [95% CI, –7.17 to –0.24]; P = .034). No significant difference was observed between the UHMWPE suture tape and UHMWPE suture groups (Figure 5).

Boxplot comparing displacement at failure (mm) between suture type groups. Dots represent individual specimen observations. Thick horizontal lines represent group medians, while top and bottom sections of the boxes represent the 25th and 75th percentiles, respectively. *Statistically significant difference.
Load at Clinical Failure
UHMWPE suture tape had a significantly higher load to reach the clinical failure displacement of 3 mm than UHMWPE suture (15.64 N [95% CI, 0.02 to 31.26]; P = .05). There was no significant difference between the standard suture group and UHMWPE suture group or UHMWPE suture tape group (Figure 6). There were no significant differences in pull-out strength between surgeons for each group.

Boxplot comparing load at 3 mm of displacement (N) between suture type groups. Dots represent individual specimen observations. Thick horizontal lines represent group medians, while top and bottom sections of the boxes represent the 25th and 75th percentiles, respectively. *Statistically significant difference.
Discussion
The most important finding of this study was that UHMWPE suture tape had a significantly higher load to reach the clinical displacement failure of 3 mm compared with UHMWPE suture. UHMWPE suture tape also had significantly less displacement at failure compared with standard suture. Additionally, UHMWPE suture tape had significantly less displacement of the medial meniscus when compared with standard suture only at 1 and 50 cycles. There were no other significant differences observed in displacement between groups at any number of cycles. Concerning ultimate failure load, no significant differences were found among the groups.
Because UHMWPE suture tape is wider than other analyzed sutures, it is possible that its unique shape/width provides a beneficial distribution of forces on meniscal tissue. As the flatter, larger width suture tape may have better distributed pull-out loads, it appeared as though suture strength was not the limiting factor during testing, as only 2 specimens in the standard suture group failed because of suture breakage. Although UHMWPE suture is stronger than standard sutures, no significant difference was observed between the 2 repair groups regarding the analyzed biomechanical properties probably because of the similarity in suture shapes and calibers, and suture strength may not significantly influence force distribution. As almost all specimens failed because of suture cutout, different suture configurations for sutures with a different composition and caliber/width should be assessed in future studies because more complex configurations (modified Mason-Allen and double double-locking loop/luggage tag) have higher ultimate failure loads. 2,15,21
Increasing interest in suture tapes has risen since their use in rotator cuff repair. Huntington et al 10 observed increased pressurized bone-tendon contact and mechanical strength in repair of the infraspinatus tendon of lambs using suture tape compared with suture wire. It has been hypothesized that wider sutures can better distribute forces over meniscal tissue and better fill the hole created during suture passage; conversely, it was also proposed that wider sutures damage more tissue during passage in meniscal root repair. 7,22 To the authors’ knowledge, there have been 2 previous studies that compared high–tensile strength suture tapes with other suture types in meniscal root injuries. 7,22 However, both of these studies used porcine menisci, which are reported to be approximately twice as stiff as human menisci, possibly resulting in an overestimation of repair strength in humans. 14,15,23 These studies also produced conflicting results. Robinson et al 22 reported a biomechanical advantage to UHMWPE suture tape, while Feucht et al 7 did not. It has been suggested that the study by Feucht et al 7 observed higher displacement for suture tape repair compared with other sutures because of knot slippage. This may have been because the utilized suture tape is commonly used to perform knotless fixation in shoulder surgery and not normally tied. In our study, we used knottable 2-mm suture tape (ULTRATAPE) and suture (ULTRABRAID), both composed of UHMWPE, as in the study by Robinson et al. 22 While Robinson et al observed that UHMWPE suture tape provided higher maximum failure loads than UHMWPE suture in a porcine model, we observed higher loads to reach the clinical displacement failure of 3 mm in UHMWPE suture tape repair compared with UHMWPE suture repair in a human model. However, our ultimate failure load was not significantly different. Concerning standard sutures such as ETHIBOND, in the study by Feucht et al, 7 FiberTape showed higher displacement during cyclic loading and higher maximum loads compared with No. 2 ETHIBOND in a porcine model, while in our study, suture tape (ULTRATAPE) had significantly less displacement at failure compared with No. 0 ETHIBOND, probably because ULTRATAPE is a knottable tape (less prone to slippage). In our study, despite No. 0 ETHIBOND being a weaker and thinner suture material, meniscal root repair performed with this suture was not significantly inferior compared with ULTRATAPE and ULTRABRAID regarding load at clinical failure and suture breakage.
Ideally, meniscal root repair should reach, at time zero, at least the same mean strength of the native meniscal root attachment (594 ± 241 N) for unrestricted rehabilitation; however, none of the sutures used for the transtibial pull-out repair technique in our study utilizing a human model (ETHIBOND, 169.47 ± 58.18 N; ULTRABRAID, 184.35 ± 30.15 N; ULTRATAPE, 172.03 ± 80.40 N), nor in the study by Robinson et al 22 using a porcine model (ULTRABRAID, 146.8 N; ULTRATAPE, 298.5 N), achieved an ultimate failure load close to the native meniscal root attachment strength. Another important feature for ideal meniscal root repair is not reaching clinical failure (displacement of 3 mm) during the rehabilitation/healing period because this threshold has been reported to compromise porcine meniscal function. 15,25 The biomechanical protocol (repair construct was cyclically loaded for 1000 cycles from 10 to 30 N at 0.5 Hz) to evaluate cyclic displacement was based on a previous study that estimated the tensile forces that repair constructs undergo with a typical 6-week toe-touch weightbearing postoperative rehabilitation program. 3,15 After 1000 cycles, all studied sutures presented a mean displacement inferior to the 3-mm threshold, with ETHIBOND and ULTRABRAID being closer to this limit (ETHIBOND, 2.69 ± 0.57 mm; ULTRABRAID, 2.79 ± 0.44 mm; ULTRATAPE, 2.36 ± 0.47 mm). Regarding the mean load to reach 3 mm of displacement, all repair groups exceeded the force of 30 N estimated to act on the meniscal repair construct during rehabilitation, especially ULTRATAPE, which presented a significantly higher load at 3-mm displacement compared with ULTRABRAID (ETHIBOND, 47.86 ± 12.61 N; ULTRABRAID, 46.04 ± 11.88 N; ULTRATAPE, 61.68 ± 12.68 N). This finding in a human cadaveric model suggests utilizing suture tape composed of UHMWPE, such as ULTRATAPE, can better withstand knee forces experienced during the postoperative rehabilitation/healing period even if a small accident increases the forces on a repair construct inadvertently, and as healing of the root occurs, it is likely that the type of suture becomes less important.
These results suggest that suture width/shape and knottability together are more important than suture composition and caliber for meniscal root repair. The suture passers were standardized for each meniscal root repair study: a half-circle conventional cutting needle (FCP-6; Ethicon) in the study by Feucht et al 7 , a FIRSTPASSST (Smith & Nephew) in the study by Robinson et al 22 , and the FIRSTPASS MINI in our study. It is worth noting that in a real scenario, suture passers such as FIRSTPASSST and FIRSTPASS MINI are used, not conventional needles. While these studies used 1 transtibial tunnel for repair and 2 sutures 22 or only 1 suture, 7 in the present study, we utilized the transtibial pull-out repair technique of the MMPR with 2 simple sutures and 2 transtibial tunnels. 14 Also, none of the previous studies assessed full repair constructs because the sutures were not tied over the anteromedial tibia, which is different from our study. 7,22 In addition, Robinson et al applied a testing force on the suture with a direction of load toward the tibial tunnel and not in the direction of the meniscal root attachment fibers . 22 However, the testing method in the present study was consistent with a previous study in which the repair strength was tested by pulling in line with the circumferential fibers of the menisci and parallel to the surface of the medial tibial plateau. This method of testing is believed to best reproduce the native forces experienced during loading by the menisci.
This study expands on the previous studies by using human specimens, a common root repair strategy, and a force vector that is representative of the in vivo state. Currently, an emerging root repair strategy reported in the literature includes 2 transtibial tunnels, 2 simple sutures, and sutures placed 7 mm from the root attachment site and 3 and 5 mm from the meniscocapsular junction. 11,13 –15,22 Suture placement 7 mm from the root attachment site is biomechanically superior to 3 and 5 mm but is often more technically challenging because of the anatomy of the knee. Simple suture-tying techniques are more appealing compared with other suture techniques because they are less complex and more resistant to meniscal displacement. 15 Also, as suture tapes are wider than sutures, they may potentially pose a problem to the articular surface, but suture tapes (and sutures) pull the meniscal root down against the tibial plateau to a level lower than the rest of the meniscus, and the root location is close to the nonarticular area, minimizing this issue.
We acknowledge some limitations in this study. As with any cadaveric study, the biological effects of tissue healing could not be replicated. In addition, the mean age of the specimens used in this study was higher than that of typically younger patient populations that undergo root repair procedures in traumatic cases. However, it has been reported in a previous study that the mean age of patients undergoing root repair was 53.3 years, similar to the mean age of the specimens used in this study (51.6 years). 18 Furthermore, each repair group was subjected to randomization to reduce the influence of meniscal tissue quality during biomechanical testing. Only male specimens were used in this study, and results may not be generalizable to the female population. 18 It has been reported that female patients are more commonly affected by degenerative meniscal tears, and future biomechanical studies should evaluate the differences in root repair strength between the sexes. Although 2 orthopaedic surgeons together standardized the surgical procedure in cadaveric knees before the study and performed most of the surgical procedures together, this could increase the chance of bias but also the reproducibility of our results. While assessing different calibers of different suture materials at the same time increases the representativeness of different sutures, this would make the true cause of a significant result more indistinguishable if we found a difference between No. 2 ULTRABRAID and No. 0 ETHIBOND. Suture construct strength was only tested using a 2-tunnel transtibial repair technique. Therefore, the findings of this study may not be directly transferable to single-tunnel repair techniques because using only 1 tunnel may alter the forces experienced at the meniscal tissue–suture interface, which could influence suture cutout and ultimate failure loads. It also should be acknowledged that the findings of this study may not be generalizable to other types of tapes or high–tensile strength sutures. We suggest that further clinical studies be performed to evaluate the clinical efficacy of high–tensile strength suture tape for 2-tunnel transtibial pull-out repair of the MMPR.
Conclusion
UHMWPE suture tape provides superior biomechanical properties for transtibial pull-out repair of the MMPR compared with UHMWPE suture regarding load at clinical failure and standard suture in relation to displacement at failure. The biological effects of healing were not considered. Concerning cyclic displacement and ultimate failure load, we found no significant differences among the groups.
Footnotes
Acknowledgment
The authors thank Smith & Nephew for the donation of medical devices/supplies and financial support to the acquisition of human cadaver knee specimens. The authors acknowledge Grant Dornan, MSc, for his statistical expertise.
One or more of the authors has declared the following potential conflict of interest or source of funding: Smith & Nephew donated the human cadaveric knee specimens and medical devices/supplies used in this study. M.J.S. has received consulting fees and research support from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Vail Health Institutional Review Board.