
Abstract
Background:
We have previously reported the technique of arthroscopically assisted drilling of osteochondritis dissecans (OCD) lesions of the elbow via the radius in a distal-to-proximal direction. With this technique, the entire OCD lesion can be drilled vertically under arthroscopic guidance with pronation and supination of the forearm and flexion and extension of the elbow joint.
Purpose:
To retrospectively evaluate return to sport, range of motion, and the Japanese Orthopaedic Association–Japan Elbow Society Elbow Function Score (JOA-JES score) after treatment of an elbow OCD lesion by drilling through the radius.
Study Design:
Case series; Level of evidence, 4.
Methods:
From November 2003 to January 2006, a total of 7 male adolescent baseball players with OCD lesions of the elbow were treated through use of arthroscopically assisted drilling via the radius. The stage of the OCD lesion was evaluated based on preoperative plain radiographs. Patients were observed for a minimum of 36 months, and clinical analysis included time for return to sport, elbow range of motion, and the JOA-JES score before intervention and at final follow-up.
Results:
We evaluated all 7 patients at a mean follow-up time of 36.1 months (range, 24-68 months). The stage of the OCD lesion on plain radiography was “translucent” in 1 patient, “sclerotic” in 5 patients, and “loosening” in 1 patient. The mean range of motion before surgery was 131.2° and –4.7° in flexion and extension, respectively, and this improved to 138.6° and 1.1° at final follow-up. The improvement in extension was statistically significant (P = .04). The mean JOA-JES score of 83.0 before surgery significantly improved to 94.0 at final follow-up (P < .001). One patient required excision of a free body at 51 months postoperatively, but all patients returned to sports early and without pain at an average of 4.6 months postoperatively. No feature of osteoarthrosis was noted on radiography on the final examination in any patient.
Conclusion:
The findings of this study demonstrate that arthroscopically assisted drilling of an elbow OCD lesion through the radial head allows for early return to sporting activities as well as improved motion and functional scores.
Keywords
Osteochondritis dissecans (OCD) of the elbow occurs in 3.4% of adolescent baseball players, 8 and the stage is classified according to Minami et al 10 as translucent, sclerotic, or loosening based on plain radiography. For OCD in the translucent and early sclerotic stages, conservative treatment by prohibiting pitching motion is selected because changes in the subchondral bone are likely to be reversible. However, when the disease is resistant to conservative treatment, surgical options should be considered. If the stage has not progressed, microfracture or drilling of bone may be indicated. Some reports have been published regarding microfracture for unstable OCD lesions of the capitellum, 3,5 in which investigators approached OCD lesions by avoiding the radial head. It is difficult to perform vertical microfracture in every part of the subchondral bone of the lesion. Further, treatment that entails only drilling of bone has not been elucidated, partly because of the absence of an effective method of bone drilling.
In the conventional procedure, anterograde bone drilling is applied from the lateral joint space of the humeroradial joint toward the lesion of the humeral capitellum, or retrograde drilling is applied from the lateral humeral condyle toward the subchondral bone of the lesion; however, accurate vertical drilling of the subchondral bone is difficult. To resolve this problem, we designed a method to vertically drill the entire lesion under arthroscopy of the elbow joint by inserting only 1 Kirschner wire from the radial diaphysis toward the articular facet, with pronation and supination of the forearm and flexion and extension of the elbow joint. 1 Since our procedure is relatively minimally invasive, pain is relieved early after surgery and range of motion (ROM) training and muscle strengthening exercise can be initiated, ensuring that the patient can return to sports early. In addition, we hypothesized that secondary osteoarthrosis may be inhibited after the procedure. In the current study, we report on the clinical and radiographic outcomes of 7 adolescent baseball players who underwent arthroscopically assisted drilling via the radius for elbow OCD lesions.
Methods
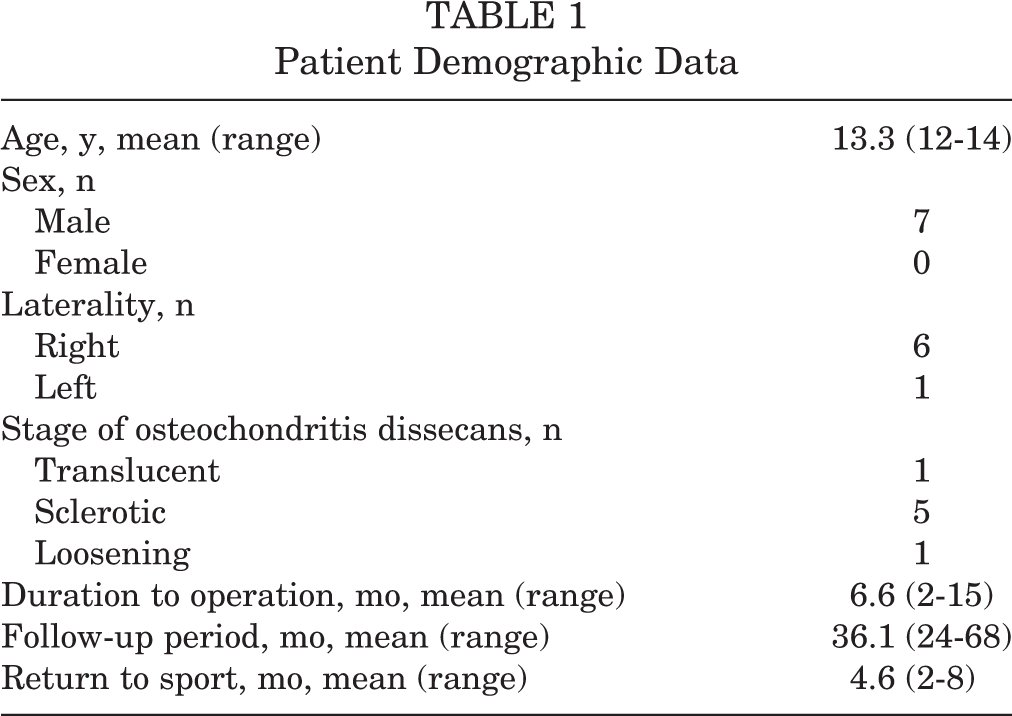
Ethical approval for this study was obtained from the ethical review board of our hospital. The study participants were 7 patients (7 elbows) with an elbow OCD lesion who underwent surgery via our procedure between November 2003 and January 2006. The right side was affected in 6 patients and the left side in 1 patient; in all patients, the dominant side was affected. All patients were boys who were baseball players. The mean age at the time of surgery was 13.3 years (range, 12-14 years), the mean disease duration before surgery was 6.6 months (range, 2-15 months), and the mean follow-up period after surgery was 36.1 months (range, 24-68 months) (Table 1).
Patient Demographic Data
Surgical Technique
The patient was placed in the supine position on the operating table. An air tourniquet was attached to the upper arm, the elbow joint was positioned at 90° of flexion, and 10 to 20 mL of saline was injected from the posterior lateral side of the elbow joint. A 30° oblique-view endoscope with a 2.4-mm diameter was inserted through an anterior lateral portal prepared on the anterior lateral side of the humeroradial joint to start intra-articular endoscopic observation. When this observation was difficult due to synovitis, a synovectomy was performed through use of a shaver. The patient’s forearm was placed in a pronation position to avoid damage to the posterior interosseous nerve, and one 1.8-mm Kirschner wire was inserted into the joint at 3 cm distal to the humeroradial joint and at about 20° to the bone axis from the center of the radial diaphysis (Figure 1A).

Diagram of the drilling technique via the radius. Drilling of the medial and lateral side of the capitellar osteochondritis dissecans lesion was achieved by (A) pronating or (B) supinating the forearm, respectively. Drilling of the posterior and anterior lesion was achieved by flexing and extending the elbow, respectively, (C) 30°, (D) 60°, (E) 90°, and (F) 120°.
The Kirschner wire was advanced until its tip came out of the cartilage surface of the radial head under arthroscopy. The forearm was placed in a supination position so that the Kirschner wire tip could be set to the lateral side of the lesion of the humeral capitellum (Figure 1B). The Kirschner wire was then advanced toward the humerus at 30°, matching the flexion angle of the elbow joint to the posterior side of the lesion, and the bone was drilled until bleeding was confirmed (Figure 2A). The Kirschner wire inserted into the humerus was pulled out to the articular facet of the radial head, according to the extent of the OCD lesion; the flexion angle was changed to 60°, 90°, and 120° toward the anterior side of the lesion while the supination position was retained; and drilling was performed (Figure 1, C-F). Then, drilling was applied to the medial side, similar to that on the lateral side, at 30°, 60°, 90°, and 120° of flexion, so as to match the Kirschner wire tip to the medial side of the lesion of the humeral capitellum while the forearm was retained in a pronation position (Figure 2B).

(A) Arthroscopic findings showed right humeral capitellum after removal of free body. (B) A Kirchner wire was advanced toward the humerus through the radial head. C, capitellum; R, radial head.
Postoperative Treatment
The area from the upper arm to the fingers was fixed with a plaster cast for 1 week after surgery, and ROM training of the elbow joint was started after 1 week. Pitching motion was initiated 8 weeks after surgery, and full-force pitching was permitted 4 months after surgery.
Evaluated Parameters
On preoperative plain radiographs, we established the OCD stage as defined by Minami et al 10 : translucent, an early stage showing an irregular rarefaction or transparency of the trabecula in the region consistent with the humeral capitellum; sclerotic, in which separation of the lesion has started and a transparent zone is present between the lesion and base bed, with sclerosis of the base bed; and loosening, in which a free loose body is present. ROM of the elbow and the Japanese Orthopaedic Association–Japan Elbow Society Elbow Function Score (JOA-JES score) were measured before surgery and at final follow-up, and the preoperative and final values for each were compared by paired t test. 12,17 The time to return to sports and the rates of recurrence and complications were also investigated. In all analyses, P < .05 was defined as statistically significant.
Results
The OCD stage was translucent in 1 patient, sclerotic in 5 patients, and loosening in 1 patient. The mean preoperative ROM was 131.2° in flexion and –4.7° in extension, and these improved to 138.6° and 1.1°, respectively, at final follow-up. The improvement in extension was statistically significant (P=.04). The mean JOA-JES score was 83.0 before surgery, and it improved to 94.0 at final follow-up (P = .001) (Table 2). For each study patient, the final JOA-JES score increased compared with his preoperative score (Figure 3).
Comparison of Clinical Evaluation Data a

a Data are presented as mean ± SD. JOA-JES score, Japanese Orthopaedic Association–Japan Elbow Society Elbow Function Score.

Japanese Orthopaedic Association–Japan Elbow Society Elbow Function (JOA-JES) scores for the study patients (each patient is represented by a separate line). All patients had increased scores at final evaluation.
One patient required excision of a free loose body 1.5 cm in diameter at 51 months after surgery because of catching, but all patients returned to sports without pain at a mean of 4.6 months (range, 2-8 months) after surgery. One patient who took 8 months to return to sport was considered to be in the late sclerotic phase because pain lasted for 8 months when he pitched with full strength. No nerve injury was noted in any patient. Follow-up telephone interviews with 3 patients after an average of 84.0 months confirmed that they had continued playing baseball at their own level without ROM limitation or pain. No feature of osteoarthrosis was noted on plain radiography of the elbow joint in the final examination in any patient, and no symptom of posterior interosseous nerve injury was shown.
Discussion
The findings of this study demonstrate that arthroscopically assisted drilling of an elbow OCD lesion through the radial head allows for early return to sports activities, improved motion, and improved functional scores. In conservative treatment of OCD of the elbow, long-term rest of the elbow and prohibition of pitching are necessary. However, patients sometimes resume pitching if symptoms subside within a short time, and this may cause disease progression. In a survey of outcomes of 6 months of conservative treatment in 24 patients with early and advanced OCD of the elbow, Takahara et al 14 found that pain remained in 13 patients, showing that this condition may not always be healed by long-term conservative treatment. When the stage progresses and a free loose body is formed, curettage and excision are performed, but residual pain after surgery and progression to arthropathic changes over time can occur. 2,9,15 Autologous cartilage transplant to a large lesion has led to favorable short- and midterm outcomes, 7,11 but this procedure is relatively invasive and complex.
Bone drilling is a minimally invasive procedure for cases in the translucent and sclerotic stages of OCD; this procedure facilitates fusion of the lesion and surrounding bone tissue by promoting blood circulation from the tissue via opening a bur hole in subchondral bone. 4 In the loosening stage, the defective region can be repaired with fibrous cartilage by bleeding from the bone marrow. However, since lesions are likely to be formed in the humeral capitellum above the radial head and because the joint space between the humeral capitellum and radial head is narrow, it is technically difficult to apply anterograde bone drilling vertically to the lesion in the direction from the lateral joint space of the humeroradial joint to the cartilage surface of the lesion. Retrograde bone drilling from the lateral humeral condyle to subchondral bone of the lesion is possible but has several drawbacks: Another skin incision is necessary, drilling vertical to the lesion through a single drill hole is difficult, and making numerous drill holes may cause fracture. Drilling bone from the posterior side of the elbow joint has been tried, 16 but additional skin incision is also necessary.
For these reasons, we developed an anterograde bone drilling method in which only 1 drill hole is prepared from the radial diaphysis toward the articular facet of the humeral head through use of a 1.8-mm Kirschner wire, and the lesion is drilled in the anteroposterior direction by bending and extending the elbow joint and in the mediolateral direction by pronating and supinating the joint. The advantages of this method are as follows: Incision of the joint is not necessary, lesions can be accurately drilled because the method can be applied under arthroscopy, the entire lesion can be vertically drilled, and early rehabilitation is possible. The indication is specific to the translucent to loosening stages because the treatment effects of vertical drilling under arthroscopy can be obtained using this procedure, compared with the effect of conventional bone drilling. However, it is necessary to pay attention to the path of the posterior interosseous nerve. The posterior interosseous nerve courses under the dorsal surface of the radial neck, 13 and its path changes by rotation of the forearm. 6 Therefore, we place the forearm in pronation to minimize the risk of nerve injury.
In the current study, we found that a free loose body formed in 1 patient at 51 months after surgery and necessitated excision, but all patients were able to return to sports without pain at an average of 4.5 months after surgery. No secondary osteoarthrosis developed, suggesting that active bone drilling prevents progression of the lesion stage and promotes healing, facilitating an early return to sports in patients with translucent- or sclerotic-stage lesions that are resistant to short-term conservative treatment. A similar effect may be obtained for patients with loosening-stage lesions in which the lesion is centrally positioned.
Limitations
This study had several limitations. First, the sample size was small. Because we restricted the survey to patients with all relevant data, only 7 patients were included in this study. Second, epiphyseal separation, lesion size, and differences in the occurrence site were not evaluated. Third, long-term follow-up was not performed because the participants were not professional athletes and have since ended high-level sports activities. Fourth, although we noted no hypertrophy of the radial head or arthropathic changes, careful long-term follow-up is needed regarding the influence of the prepared drill hole on the radial head, cartilage surface of the lesion, and epiphyseal line of the radial head. Fifth, we evaluated the course of treatment using only plain radiographs. We did not perform appropriate magnetic resonance examinations, which are useful for evaluation of OCD treatment.
Conclusion
The study outcomes showed that drilling of bone through the radial head under arthroscopy for OCD of the elbow permits vertical drilling of the entire lesion and allows an early return to sports activities.
Footnotes
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethical review board of Kyoto Kuramaguchi Medical Center (2016060604).