
Abstract
Background:
Prospective studies on injuries in martial arts competitions are scarce, especially those involving time-loss injuries. The upsurge of karate athletes competing in top-level karate competitions warrants elucidation of the time-loss injury risk.
Purpose:
To determine the time-loss injury proportion and incidence rate, describe the injury pattern among elite senior karate athletes, and compare the risk of time-loss injuries in male versus female athletes and in individual (ie, weight categories) versus team competitions (free-weight category).
Study Design:
Descriptive epidemiology study.
Methods:
Data were collected at 4 consecutive World Karate Championships (2010, 2012, 2014, and 2016). Injury incidence rates were calculated per 1000 athlete-exposures (IIRAE) and per 1000 minutes of exposure (IIRME), with 95% CIs. Subgroups were compared by calculating their rate ratios with 95% CIs.
Results:
A total of 506 injuries were recorded, of which 51 were time-loss injuries (10%). The overall time-loss injury rate was significantly lower for female versus male athletes and slightly lower for team versus individual competitions. Overall, 1.4% of all athletes sustained a time-loss injury, and the IIRAE and IIRME were 5.13 (95% CI, 3.82-6.74) and 1.98 (95% CI, 1.47-2.60), respectively. The most common type of time-loss injury was fracture (41%), followed by dislocation (20%) and concussion (12%).
Conclusion:
The time-loss injury incidence rate for top-level karate competitions found in this prospective study was relatively low. Comprehensive knowledge about the incidence of time-loss injuries during karate competitions represents an essential basis to develop effective strategies for injury prevention. Thus, the introduction of a uniform injury surveillance system in martial arts is of utmost importance.
Since the announcement that karate will make its debut appearance at the Summer Olympic Games in 2020 in Tokyo, Japan, 14 there has been an increase in the number of athletes participating in top-level karate tournaments. 22 The World Karate Federation (WKF), which is recognized by the International Olympic Committee as the international governing body for Olympic-style karate, has more than 150 member countries and hosts the World Karate Championships biennially. The World Karate Championships feature 2 events: kumite (fight with a real opponent) and kata (fight with imaginary opponents).
The kumite event is further divided into individual and team competitions. In individual competitions, athletes of similar weight compete against each other in specified weight categories. Karate is unique among the combat sports because there is a team competition in which team members compete in separate bouts without any matching by weight categories. Male teams comprise 7 members with 5 competing in a match, while female teams comprise 4 members with 3 competing in a match. Before each match, each team must designate the order in which its chosen team members will compete, without any weight consideration or stratification. The tournament format of both individual and team competitions is direct elimination with repechage (ie, a system in which competitors who lose to pool winners enter into a secondary championship bracket and compete for third place). The scoring system is as follows: kicks to the head and throws, followed by a scoring strike, are awarded 3 points (ippon); kicks to the trunk are awarded 2 points (waza-ari); and punches to the head and trunk are awarded 1 point (yuko). Bouts are ended before their allocated time if an 8-point score gap ensues.
WKF or Olympic-style karate is a light-contact sport. The most dangerous techniques are banned (attacks to the throat or face with an open hand; attacks with the head, knees, or elbows; throws over the shoulder; etc), and contestants must perform all techniques with control and good form. If techniques are not controlled, a warning or penalty is imposed by the referees. Kumite contestants are required to wear WKF-approved protective equipment such as body protectors (plus chest protectors for female athletes), mouth guards, hand protectors (mitts), and shin and foot protectors.
Karate confers numerous benefits to its practitioners (eg, health, self-defense, self-confidence) 1,5 ; however, an injury is an inherent risk of participation in any sport, especially in combat sports such as karate. The seemingly disparate data on injury severity in karate can be attributed to the diversity in operational injury severity definitions and classification methods across previous studies. In recent studies, the severity of injuries has been categorized as minor, moderate, or severe according to the nature of the injury (ie, diagnosis). 3,4,17,23 A more objective measure of injury severity is the number of days lost from participation, but few studies of karate injuries have reported on time loss. Thus, the severity of time-loss injuries in karate remains unclear.
There is a paucity of data examining the relative risk of injuries among male and female karate athletes. Similarly, no studies to date have compared the injury risk in individual (ie, with weight categories) and team (ie, without weight categories) competitions. It is important to attempt to identify potential risk factors for an injury (eg, competitions with or without weight categories) to inform the development of injury prevention strategies and policies in karate.
The aims of this study were to (1) determine the time-loss injury proportion and incidence rate, (2) describe the time-loss injury pattern, and (3) compare the risk of time-loss injuries in male versus female athletes and in individual versus team competitions among elite senior karate athletes competing at 4 consecutive World Karate Championships.
Methods
This injury surveillance study was approved by the appropriate ethics committee.
Participants
Injury and exposure data were collected prospectively from all the fights at 4 consecutive WKF World Karate Championships (2010 in Belgrade, Serbia; 2012 in Paris, France; 2014 in Bremen, Germany; and 2016 in Linz, Austria). An individual competition comprises 5 weight divisions per sex (<60 kg, <67 kg, <75 kg, <84 kg, and >84 kg for male athletes and <50 kg, <55 kg, <61 kg, <68 kg, and >68 kg for female athletes). A team competition has no weight categories, with male teams comprising 5 athletes and female teams comprising 3 athletes. All female bouts are scheduled for 2 minutes, while all male bouts are scheduled for 3 minutes (real time).
Data Collection
Exposure data were obtained from official tournament records. Injury data were recorded on-site by trained medical personnel using a simple check-off injury-reporting form, which was adapted from a form that had been used previously at the WKF World Karate Championships. 2 –4,8 Collected data included sex, age, weight category, injured body part, type of injury, and injury severity (non–time-loss or time-loss). For each tatami (competition area), there was 1 doctor plus 1 assistant. The WKF World Karate Championships are held in different locations each time. Thus, in an effort to standardize data collection across tournaments, the chair of the WKF Medical Commission instructs the local tournament sports medicine staff in the injury-recording procedure. The quality of recorded data was reviewed by the chair of the WKF Medical Commission and the on-site medical personnel 3 times per day to clarify any uncertain or incomplete entries and to ensure a uniform injury classification. When required, athletes were referred to a nearby hospital for further diagnostic procedures, and feedback on the diagnosis was retrieved directly by the chair of the WKF Medical Commission. In this study, all recorded injuries were subsequently coded by a trained researcher using the Orchard Sports Injury Classification System version 10 (OSICS-10). 20
Operational Definitions
An injury was defined as any physical complaint for which an athlete sought assistance from tournament medical personnel or for which referees asked the tournament doctors for an evaluation of the athlete to confirm that he or she was fit to continue competing. Injuries were categorized as non–time-loss or time-loss, where time-loss injuries were those that prevented the athlete from completing the present bout and/or subsequent bouts and from participating in sport activities for a minimum of 1 day thereafter. 6 One athlete-exposure (AE) was defined as 1 individual athlete participating in a bout in which he or she is exposed to the possibility of being injured, which means that for each bout, there are 2 AEs. One minute of exposure (ME) was defined as 1 minute of fighting per 1 individual athlete in a bout.
Data Analysis
The injury proportion was calculated as the percentage of athletes experiencing a time-loss injury. Time-loss injury incidence rates were calculated per 1000 AEs (IIRAE) and per 1000 MEs (IIRME) with 95% CIs using standard formulas for Poisson rates. 12 Subgroups were compared by calculating the rate ratio (RR) with the 95% CI. The 95% CI for the RR was used to determine whether 2 IIRs differed significantly from one another; that is, 2 IIRs were deemed statistically different from one another if the 95% CI for the RR did not include the null value (ie, 1).
Results
Incidence
Table 1 provides an overview of the number of athletes, number of time-loss injuries, number of AEs, MEs, and time-loss IIRs. A total of 3706 athletes participated in the 4 WKF World Karate Championships included in this study. A total of 506 injuries were recorded, of which 51 (10%) were time-loss injuries. Overall, 1.4% of athletes sustained a time-loss injury, and the IIRAE and IIRME were 5.13 (95% CI, 3.82-6.74) and 1.98 (95% CI, 1.47-2.60), respectively.
Number of Athletes, Number of Time-Loss Injuries, Number of AEs, MEs, and IIRs a

a Data in parentheses are 95% CIs. AE, athlete-exposure; IIRAE, injury incidence rate per 1000 athlete-exposures; IIRME, injury incidence rate per 1000 minutes of exposure; ME, minutes of exposure.
Injury Pattern
Tables 2 and 3 provide an overview of the frequency and proportion of time-loss injuries by type and by anatomic location, respectively. The most common type of time-loss injury was fracture (41%), followed by dislocation (20%) and concussion (12%).
Frequency and Proportion of Time-Loss Injuries by Type of Injury a
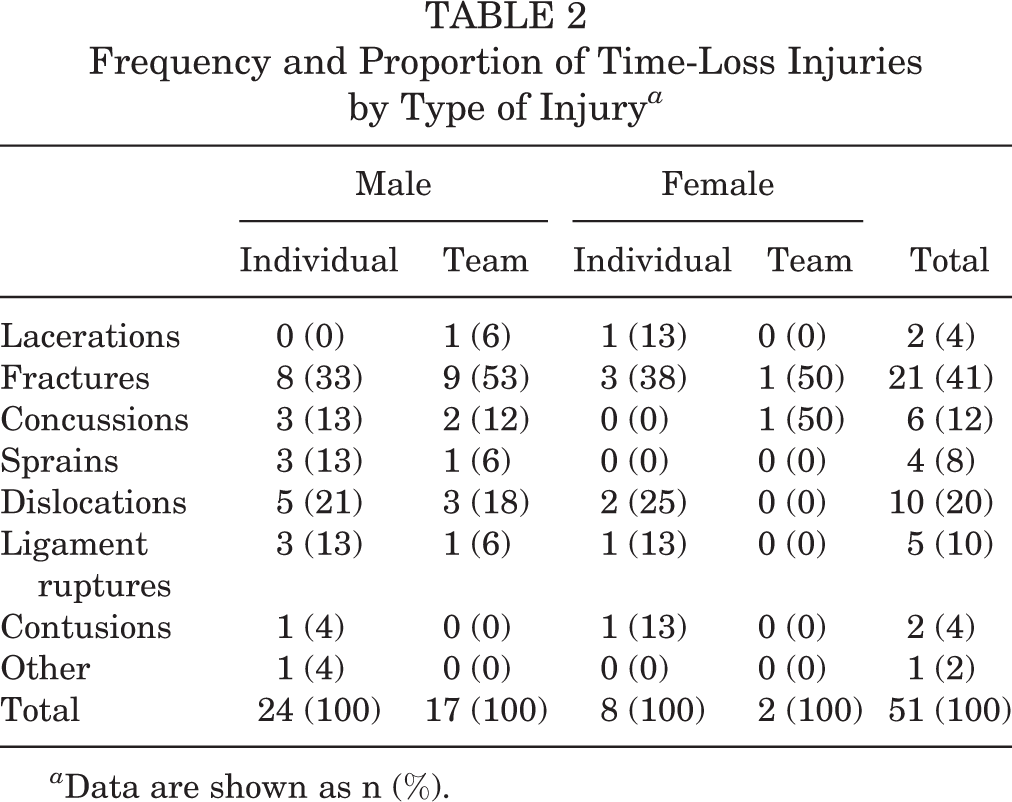
a Data are shown as n (%).
Frequency and Proportion of Time-Loss Injuries by Anatomic Location a

a Data are shown as n (%).
Risk Factors
With regard to risk factors, female athletes had a lower rate of time-loss injuries compared with male athletes; however, the difference was statistically significant when comparing the IIRAE (RR, 0.35 [95% CI, 0.17-0.70]) but not the IIRME (RR, 0.53 [95% CI, 0.27-1.05]). Athletes in team competitions had a lower time-loss injury rate compared with athletes in individual competitions; however, the difference was not statistically significant when comparing either the IIRAE (RR, 0.66 [95% CI, 0.38-1.17]) or the IIRME (RR, 0.65 [95% CI, 0.37-1.15]).
Discussion
The incidence of time-loss injuries in the WKF World Karate Championships as found in this study was low (IIRAE, 5.13 [95% CI, 3.82-6.74]). Time-loss injuries accounted for 10% of the total number of recorded injuries and affected only 1.4% of athletes competing in top-level karate tournaments.
Epidemiological studies using data from the WKF World Karate Championships have been published regularly since 1996. In 2009, Arriaza and colleagues 4 analyzed the incidence of injuries during the WKF World Karate Championships from 1996 to 2006. Despite noting the implementation of several modifications to the competition rules during the study period, the authors found that the incidence of time-loss injuries did not change significantly, with the IIRAE being 4.40 from 1996 to 2000, 4.55 from 2002 to 2004, and 4.35 in 2006. In our study, we found a slightly higher time-loss IIR (5.13 per 1000 AEs), but the overall IIR was lower. The fact that the time-loss IIRs have remained stable, despite a decrease in the overall number of injuries, may be explained by higher physical demands of the competition, changes to the competition rules and scoring system, and corresponding changes in tactics. With the upcoming qualification for the first karate tournaments in the history of the Olympic Games, athletes may be faster and stronger than ever before, which makes them more able to inflict injuries on their opponents. It is possible that the new scoring system, with additional points awarded to kicking (3 points) and sweeping techniques (3 points) has caused competitors to use them more frequently and that these techniques could cause more severe injuries because of the greater impact energy of the body segments involved (lower limb vs upper limb). 19 Alternatively, the reduction in the overall injury incidence could be related to the introduction of new compulsory protective equipment (ie, shin pads and foot protection) in 2005; that is, new protective equipment may have contributed to reducing the incidence of minor injuries without having had any impact on time-loss injuries (eg, nasal fractures, wrist fractures, and shoulder dislocations).
Previous studies have focused mainly on overall IIRs without specific research on time-loss injuries sustained during top-level competitions. Halabchi et al 13 reported a similar time-loss IIR among female athletes competing at national-level championships in Iran (4.4 per 1000 AEs), whereas Boostani et al 7 found a higher incidence of moderate and severe injuries among male athletes competing in an Iranian national team selection tournament (24.1 per 1000 AEs). It is unclear why the reported incidence of time-loss injuries is higher in Iranian karate competitions compared with the WKF World Karate Championships. Perhaps there are differences in study methodologies, or perhaps the difference in the injury risk is related to differences in competitiveness, risk-taking behavior, competition styles, or tactics.
In karate, any scoring technique must be applied to a scoring area, appropriately controlled with regard to the area being attacked, and must satisfy 6 scoring criteria. One of them is correct distance, which means that punches and kicks must be delivered to between skin “touch” contact and 5 cm from the face, head, or neck to be valid. For senior competitors, noninjurious, light, controlled “touch” contact to the face, head, and neck is allowed. This fact may lead to the low concussion incidence rate. The concussion incidence rate in top-level karate (0.6 per 1000 AEs) is smaller than in other contact or collision sports such as taekwondo (4.9 per 1000 AEs), 16 football (2.3 per 1000 AEs), 18 and ice hockey (1.5 per 1000 AEs) 18 and similar to that in soccer (0.5 per 1000 AEs) 18 and wrestling (0.5 per 1000 AEs). 18 However, it is important to note that the duration or length of an AE may vary across different sports. Thus, the relative risk of concussions may be after accounting for the actual time at risk.
In the current study, the most commonly injured anatomic region was the head and face (41%), followed by the upper extremities (39%). This particular distribution of injuries is probably related to the fact that top-level karate athletes use upper limb techniques more frequently than lower limb techniques and that blows are more frequently delivered to the head region than to the trunk. 23
We found that the time-loss IIRME was significantly lower for team competitions compared with individual competitions. Because team competitions allow athletes with different body weights to compete against each other, one might think that the injury risk is greater in team competitions compared with individual competitions. However, our results suggest the opposite. Perhaps allowing athletes with different body weights to compete against each other, and bouts to end in a tie, change the tactics of the game and, along with it, the injury risk profiles. For instance, lighter weight athletes facing heavier weight athletes might adopt a more defensive style, avoiding contact and accepting a tie or even losing by a minimum score, giving advantage to the team and reducing the risk of injuries. Also, excessive strength in the hits of the heavier athlete could lead to penalties that might hinder the chances of winning the match, imposing an extra level of control during the fight.
With regard to the methodology followed for injury recording on-site by the WKF Medical Commission, the fact that referees call for a doctor every time to assess an athlete during the competition, even for minor injuries, and that all injuries are recorded, no matter how minor, offer the advantage of not relying on information provided by each national federation’s medical team. This system minimizes loss of information, a problem detected when analyzing the injuries that took place during the Rio Olympic Games, 21 where only 6% of the injuries were detected by both the national Olympic committees and the Rio staff and only 59% of the injuries were reported by the national Olympic committees.
It must be stressed that there are different martial arts with different competition rules and that, even within karate itself, there are different associations that run their own championships under different rules in terms of protective equipment allowed and the degree of contact tolerated by the referees, which makes a comparison of published data difficult.
The protection of athletes’ health by preventing injuries is an important task for international sports federations and for the International Olympic Committee. 15 A standardized assessment of sport injuries provides important epidemiological information, directions for injury prevention programs, and the opportunity for monitoring long-term changes in the frequency of injuries. 11 Junge and colleagues 15 established an injury-reporting system for multisport events (for team sports tournaments and for individual sports). Moreover, Finch and colleagues 10 stated that injury surveillance during sporting events should be a part of the duty of care to the participants to help make future events safer.
Injury definition is a key element of any injury surveillance system. It is well known that injury classification according to its effect on the injured athlete’s performance (ie, days lost from training or match participation) can yield differences between sports and even teams and observers within the same sport. 9 Different sports and sport settings require different injury recording protocols and possibly different injury classification methods: the same injury (ie, a fractured metacarpal bone) could have a different impact in the capacity to train or compete for a soccer player than a team handball player, but still anatomically, it would be the same injury; in many sports, when injuries take place during championships, it is usually difficult to track the athletes once they leave the stadium to know exactly how many days they spend away from training because of the injury, as often there is a low training or even rest period after championships, and keeping in touch with the athletes or their representatives is difficult, especially in case of international competitions. For that reason, an injury classification system based on the medical diagnosis (similar to OSICS-10) was adopted by the WKF Medical Commission in 1992.
Limitations
There are limitations to the current study. First, injuries may be underreported, as it is possible that some injured athletes did not seek medical attention or care or that referees may have failed to call on the doctor when an athlete was injured. However, the degree of underreporting of injuries is likely to be small because the scoring system stipulates that valid techniques should not cause harm or injury to the opponent, which means that athletes have an incentive to disclose all injuries, and referees are instructed to call on the doctor when a potentially injurious incident occurs. Second, the severity of injuries in terms of the actual number of days lost to participation was not measured in this study. However, in large international championships, it is not feasible to follow up with individual athletes who return to their respective countries after the conclusion of the tournament. Third, because we did not know the age of each athlete competing at the championships, we were not able to investigate whether the injury risk varied by age. We recommend future studies to investigate the potential effect of age.
Conclusion
During 4 consecutive WKF World Karate Championships, a total of 506 injuries were recorded, of which 51 (10%) were time-loss injuries. Overall, 1.4% of athletes sustained a time-loss injury. The time-loss IIRAE was 5.13 (95% CI, 3.82-6.74), which is slightly higher than previously reported time-loss IIRs in karate. The most frequently injured anatomic region was the head and face (41%), followed by the upper extremities (39%). The most common type of time-loss injury was a fracture (41%), followed by a dislocation (20%) and a concussion (12%). Female athletes had a lower rate of time-loss injuries compared with male athletes. Athletes in team competitions had a slightly lower time-loss injury rate compared with athletes in individual competitions. These findings may be used as a yardstick for future studies to evaluate the impact of any future rule changes or preventive measures in karate.
Footnotes
Acknowledgment
The authors thank the Medical Commission of the WKF for its support and cooperation.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Ethics Committee of the Faculty of Physical Education and Sports, Comenius University (reference No. 06/2017).