
Abstract
Background:
The treatment of patellar instability in the setting of trochlear dysplasia is challenging.
Purpose/Hypothesis:
The purpose of this study was to evaluate outcomes for the treatment of recurrent patellar dislocations due to trochlear dysplasia using anteromedialization tibial tubercle osteotomy combined with medial patellofemoral ligament (MPFL) imbrication. We hypothesized that the treatment of patellar instability with tibial tubercle osteotomy and MPFL imbrication would result in improved patient satisfaction and decrease patellar instability events in patients with prior instability and trochlear dysplasia.
Study Design:
Case series; Level of evidence, 4.
Methods:
We performed a retrospective analysis of patients who underwent MPFL imbrication and concomitant anteromedialization tibial tubercle osteotomy for recurrent patellofemoral instability at a single institution. The minimum follow-up was 1 year. Patient demographic information including age at the time of surgery, sex, body mass index (BMI), tibial tubercle–trochlear groove (TT-TG) distance, and grade of trochlear dysplasia was collected along with relevant operative data. Postoperatively, recurrent dislocation events as well as Knee injury and Osteoarthritis Outcome Score (KOOS), Western Ontario and McMaster Universities Osteoarthritis Index, and Kujala scores were collected, and satisfaction was ascertained by asking patients whether they would undergo the procedure again.
Results:
A total of 37 knees from 31 patients (23 female) with a mean follow-up of 3.8 years (range, 1-8.9 years) were included. The mean patient age was 28.8 years (range, 14-45 years), the mean BMI was 24 kg/m2 (range, 20-38 kg/m2), and the mean preoperative TT-TG distance was 18.9 mm (range, 8.4-32.4 mm). Two knees were classified as low-grade trochlear dysplasia (Dejour A) and 35 as high-grade trochlear dysplasia (Dejour B-D). At final follow-up, patients reported mean KOOS subscale scores of 86.5 (Pain), 79.8 (Symptoms), 93.9 (Activities of Daily Living), 74.3 (Sports/Recreation), and 61.9 (Quality of Life), as well as a mean Kujala score of 81.3. Mean patient satisfaction was 8.3 of 10. The majority of knees (86.5%; 32/37) remained stable without recurrent instability after this procedure, while 13.5% (5 knees) suffered a recurrent dislocation, with 2 requiring revision surgery. Eight knees (21.6%) underwent subsequent hardware removal.
Conclusion:
Anteromedialization tibial tubercle osteotomy with MPFL imbrication can improve recurrent patellofemoral instability and provide significant clinical benefit to patients with trochlear dysplasia.
Keywords
Treatment strategies for recurrent patellar dislocations can be categorized into soft tissue procedures and bony procedures. Soft tissue procedures include reconstructing the medial patellofemoral ligament (MPFL) with an autograft or allograft as well as MPFL repair or tensioning with oversewing (imbrication) the ligament at its patellar insertion. Arthroscopic lateral parapatellar release may be performed independently or combined with medial procedures as well. Bony procedures for the treatment of patellofemoral instability include trochleoplasty and tibial tubercle osteotomy. A recent report detailed the increased frequency with which patella-stabilizing surgery is being performed, noting that between 2007 and 2014, the frequency of such procedures had almost doubled in a large private-payer insurance database. 2
A number of treatment algorithms have been developed and published to guide decision making in the treatment of patellar instability. 25 Several authors have published good results with MPFL reconstruction to help restore the medial checkrein, especially in the setting of a normal tibial tubercle–trochlear groove (TT-TG) distance. 15,22 However, in patients with a dysplastic trochlea, patella alta, and/or an elevated TT-TG distance, performing MPFL reconstruction does not address these anatomic abnormalities and may have a lower rate of success. 12 Steiner et al 19 suggested that MPFL reconstruction alone in the setting of trochlear dysplasia has excellent postoperative outcomes and no difference in redislocation rates. However, other studies have demonstrated an increased rate of redislocation after MPFL reconstruction or imbrication alone in the setting of trochlear dysplasia. 1,16,24
The clinical results of trochleoplasty have shown promising results including improved postoperative Kujala scores, with recurrence rates reported as low as zero in a series of 20 to 30 knees. 3,13 While trochleoplasty addresses an anatomic abnormality, it is technically challenging, and there are numerous reported complications including iatrogenic cartilage damage, leading to advanced arthrosis, patellar incongruence, overcorrection, and arthrofibrosis. 5,6 Long-term data regarding groove-deepening procedures are also still lacking. Therefore, in the patient with flat trochlear anatomy and/or an increased lateral vector caused by a high Q-angle and/or an elevated TT-TG distance, tibial tubercle osteotomy may be a powerful treatment option that avoids the risk of iatrogenic injuries to the trochlea. Further MPFL imbrication in the setting of tibial tubercle osteotomy may be advantageous to MPFL reconstruction, as it protects against potential iatrogenic injuries to the patella such as fractures.
The purpose of this study was to investigate the outcomes of tibial tubercle osteotomy and MPFL imbrication for the treatment of recurrent patellar dislocations in the setting of trochlear dysplasia. We hypothesized that MPFL imbrication and tibial tubercle osteotomy could successfully treat recurrent patellar dislocations in patients with trochlear dysplasia, leading to low recurrence rates and good patient-reported outcomes.
Methods
Participants
After institutional review board approval, a retrospective analysis was performed of patients who underwent MPFL imbrication and tibial tubercle osteotomy for the treatment of recurrent patellar dislocations from January 2009 to December 2015 at a single institution. The indication for the procedure was recurrent patellar instability due to trochlear dysplasia. Included in the study were patients who had undergone both MPFL imbrication and anteromedialization tibial tubercle osteotomy with a minimum 1-year postoperative follow-up and who completed outcome questionnaires. Exclusion criteria included revision procedures and treatment for patellofemoral arthritis rather than instability, as well as patellar instability caused by abnormal version as identified on the preoperative physical examination. Instability from a known diagnosis of a hypermobility disorder such as Ehlers-Danlos syndrome or a preoperative Beighton score greater than 4 was not considered an exclusion.
Demographic data including age at the time of surgery, sex, body mass index (BMI), and history of prior procedures, as well as operative data including concomitant procedures were collected, and postoperative and follow-up notes were reviewed. A survey was sent to each patient to measure outcomes and patient satisfaction. Follow-up time was calculated as the last clinic visit or survey completion date, whichever came later. The Knee injury and Osteoarthritis Outcome Score (KOOS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and Kujala scores were calculated after patients filled out the appropriate questionnaire. 9,14 Additionally, patients were asked whether they had experienced dislocation after surgery and whether they would undergo surgery again, and they were instructed to rate their overall satisfaction on a scale from 0 to 10 (best). We measured the TT-TG distance from patients’ preoperative magnetic resonance imaging. 4
Trochlear dysplasia was graded based on radiographic parameters as first described by Dejour and Saggin. 5 In type A, the crossing sign is present. The trochlea is shallower than normal but still concave and symmetrical. In type B, the crossing sign and trochlear spur are present on lateral radiography. The trochlea is flat or convex on axial images. In type C, there is a crossing sign and in addition the double contour sign, representing sclerosis of the subchondral bone of the medial hypoplastic facet. Here, the lateral facet is convex. Type D combines the crossing sign, supratrochlear spur, and double contour sign going below the crossing sign. A cliff pattern is seen on axial views for type D. Patients were stratified as low grade (Dejour classification A) or high grade (Dejour classification B-D) for analysis.
Surgical Technique
The same surgical technique was performed by 4 fellowship-trained orthopaedic sports medicine surgeons (B.T.F., C.R.A., C.B.M., A.L.Z.). The patient was positioned supine on a radiolucent table, and diagnostic arthroscopic surgery performed for each patient. Arthroscopic lateral release was performed if there was lateral tilt beyond neutral on the preoperative examination or lateral overhang diagnosed during arthroscopic surgery. After arthroscopic surgery, anteromedialization tibial tubercle osteotomy was performed. A longitudinal incision was made starting just medial to the tibial tubercle. The osteotomy site was marked on the medial aspect of the tibia, starting proximally next to the tubercle at a depth of 1.0 to 1.5 cm and continuing distal 5 cm. As the mark was extended distally, the bony shingle was thinned until there was a thickness of 2 to 4 mm of bone at the most distal aspect to avoid creating a step cut. This allowed the shingle to hinge and rotate medially with minimal prominence. After marking the medial side of the tibia, a bone cut was performed with a saw from medial to lateral, angling posteriorly. This allowed the tubercle to be translated anteriorly. The osteotomy site was then translated anteromedially and affixed with two 4.5-mm fully threaded cortical screws (Depuy Synthes) with a lag technique and countersinking to prevent screw-head prominence.
Imbrication was performed after osteotomy. A longitudinal incision was made at the medial aspect of the patella and deepened until the MPFL or its corresponding layer was encountered. If intact, the MPFL was transected in line with the incision, taking care to leave a 1-cm cuff of tissue attached to the patella. The MPFL was then imbricated by oversewing the tissue in a pants-over-vest manner, shortening the MPFL approximately 10 mm. A No. 2 FiberWire (Arthrex) was used to suture the imbricated MPFL. The knee was then brought through full range of motion to monitor patellar tracking and to evaluate for overconstraint. A clinical examination of patellar mobility at 0° and 30° was performed after each stage of the procedure and again before closure.
Postoperative Rehabilitation
Immediately after surgery, patients were allowed partial weightbearing while in extension. Range of motion was encouraged from 0° to 40° in the first 2 weeks, 0° to 60° during weeks 2 to 4, and 0° to 90° during weeks 4 to 6 postoperatively. Full weightbearing without crutches was allowed after 6 weeks or after radiographic evidence of healing at the osteotomy site, whichever came later.
Results
After the application of inclusion and exclusion criteria, we identified 31 patients who underwent MPFL imbrication and tibial tubercle osteotomy for patellar instability and had completed the institutional standard postoperative questionnaire. Six patients underwent bilateral procedures, for a total of 37 knees. A prior arthroscopic procedure had been performed in 12 knees (lateral release in 9, removal of loose body/debridement in 2, and MPFL imbrication alone in 1). The mean follow-up time was 3.8 ± 2.2 years (range, 1-8.9 years) at the time of survey completion. The mean age of patients was 28.8 ± 9.1 years (range, 14-45 years), and there were 23 women and 8 men in the cohort. The mean BMI was 24 ± 5 kg/m2 (range, 20-38 kg/m2), with a mean TT-TG distance of 18.9 ± 5.5 mm (range, 8.4-32.4 mm) (Table 1). The most common concomitant procedure was arthroscopic lateral release (n = 24 knees). In total, 33 of 37 knees underwent concomitant or prior lateral release. None of the patients were without radiographic evidence of trochlear dysplasia. Of the 37 knees, 2 were classified as having low-grade trochlear dysplasia (Dejour A), and the remaining 35 had high-grade trochlear dysplasia (Dejour B-D). Further details of trochlear dysplasia grading and Dejour classification are listed in Table 2.
Demographic Characteristics of Patients a

a BMI, body mass index; TT-TG, tibial tubercle–trochlear groove.
Dejour Classification a

a Type A: crossing sign present on lateral view; type B: crossing sign and trochlear spur present; type C: crossing sign and double contour sign present; and type D: crossing sign, trochlear spur, and double contour sign present.
Outcome data were collected on all 31 patients. The mean postoperative KOOS subscale scores were 86.5 for Pain, 79.8 for Symptoms, 93.9 for Activities of Daily Living, 74.3 for Sports/Recreation, and 61.9 for Quality of Life. The mean postoperative WOMAC scores were 89.8 for pain, 83.3 for stiffness, and 93.9 for function, and the mean postoperative Kujala score was 81.3. The mean patient satisfaction rating was 8.3, and 23 of 31 patients (74.2%) stated that they would undergo the procedure again. The outcomes are listed in Table 3.
Postoperative Patient-Reported Outcome Scores a
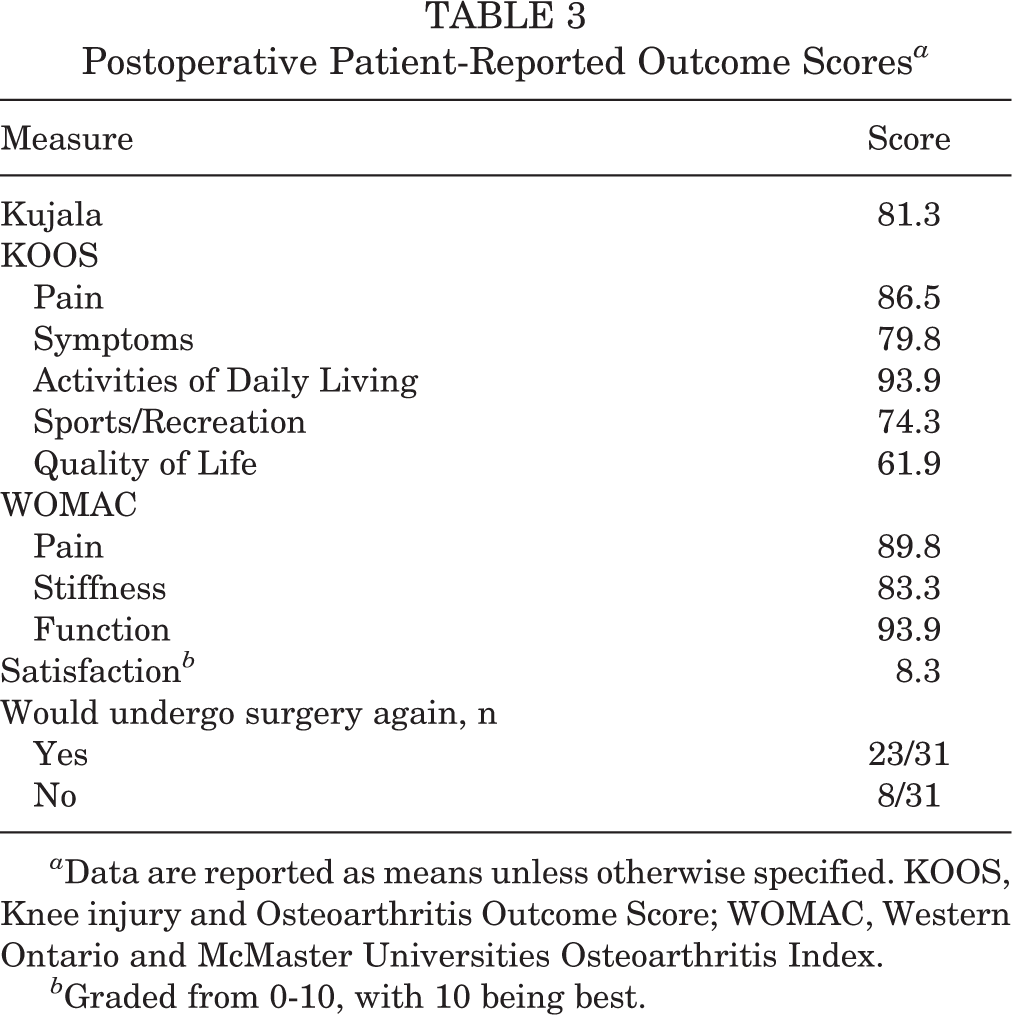
a Data are reported as means unless otherwise specified. KOOS, Knee injury and Osteoarthritis Outcome Score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Graded from 0-10, with 10 being best.
At the time of survey completion, 86.5% (32/37) of knees remained stable without recurrent instability after their surgery, while 5 knees in this cohort experienced a recurrent patellar dislocation. Two patients (each with 1 knee treated) had a diagnosis of Ehlers-Danlos syndrome; however, neither suffered a recurrent dislocation. All patients experiencing a recurrent dislocation were classified as having high-grade trochlear dysplasia. Further postoperative complications included 1 fracture, 1 loss of fixation, and removal of hardware in 8 of 37 knees (21.6%). No patient with or without a recurrent dislocation went on to undergo trochleoplasty. One patient went on to undergo MPFL reconstruction, and another underwent vastus medialis obliquus advancement. Further information on the patients who experienced recurrent dislocations can be found in Table 4.
Patients Who Suffered a Recurrent Dislocation After Procedure a

a Four patients (5 knees) suffered a redislocation after surgery. BMI, body mass index; MPFL, medial patellofemoral ligament; TT-TG, tibial tubercle–trochlear groove.
Discussion
The principal findings of this study show that in patients with patellar instability and trochlear dysplasia who undergo anteromedialization tibial tubercle osteotomy and MPFL imbrication, 86.5% did not suffer a subsequent patellar dislocation at a mean follow-up time of 3.8 years. Furthermore, the mean satisfaction score was 8.3 out of 10, and 74.2% of patients stated they would undergo the procedure again.
The surgical technique of tibial tubercle osteotomy combined with MPFL imbrication has multiple advantages. Tibial tubercle osteotomy allows for variable correction of the coronal alignment combined with bringing the tubercle to a more anterior position to offload the trochlea. When patella alta, or relative patella alta due to a short, dysplastic trochlea, is encountered, the tubercle may also be brought more distal to improve the range over which the patella encounters bony congruency with the trochlea. In addition, MPFL imbrication obviates the risk of patellar fractures as well as the need for anchors and either tendon harvesting or using an allograft seen in MPFL reconstruction. 18
However, data-driven algorithms for the treatment of patellar instability in the setting of trochlear dysplasia have been difficult to develop because of differing clinical opinions and varying data in the literature. Some authors have suggested MPFL reconstruction alone as a first-line treatment, while others have suggested combined surgical treatment of the medial stabilizers along with tibial tubercle osteotomy. 1,19,24 Hopper et al, 8 in their case series, found that in patients who had undergone MPFL reconstruction, 100% of the patients with high-grade trochlear dysplasia had experienced redislocation compared with 9.3% of those classified as having low-grade dysplasia. Schöttle et al 16 evaluated arthroscopic MPFL repair in relation to trochlear dysplasia and found that at a follow-up of 12 months, 0 of 26 knees redislocated in the no/mild trochlear dysplasia group versus 4 of 22 knees in the severe dysplastic group. Patient-reported outcomes also improved in the no/mild trochlear dysplasia group; however, only limited improvement was seen in the group with more severe trochlear dysplasia, suggesting that MPFL imbrication alone was not sufficient. 16
We sought to evaluate whether tibial tubercle osteotomy combined with MPFL imbrication could stabilize this difficult subset of patients. In our cohort of patients with high-grade trochlear dysplasia, recurrent dislocations occurred in 5 of 37 (13.5%) knees at a mean follow-up of 3.8 years. These results reflect similarly to those of Tsuda et al, 21 who reported patellar instability in 11.3% of patients after undergoing Fulkerson osteotomy for recurrent instability, although their study included predominantly lower grade trochlear dysplasia, with 50 of 62 knees being type A or B. Vivod et al 23 published long-term follow-up data on patients after patellofemoral realignment procedures without stratification for trochlear dysplasia, and their KOOS scores for Pain (81), Symptoms (77), Activities of Daily Living (85), Sports/Recreation (50), and Quality of Life (44) compare similarly with results using our technique. Mulliez et al 11 published clinical outcomes on MPFL reconstruction plus tibial tubercle osteotomy in patients without trochlear dysplasia, and the KOOS scores presented in their study are also similar to scores from our cohort.
Trochleoplasty has been described in the literature as early as the 1970s for the treatment of patellar instability. 10 Multiple techniques for the correction of a hypoplastic femoral trochlea have been described, modified, and adopted. Fucentese et al 7 described good improvements in the median Kujula score and instability with the procedure but unpredictable results with regard to pain, with some patients reporting worse pain at more than 2 years postoperatively compared with before the procedure. Trochleoplasty is a technically demanding procedure, with potential complications including continued instability, limited range of motion, worsening anterior knee pain, advanced arthrosis, patellar incongruence, overcorrection, and arthrofibrosis. 5,6,17 Complications of postoperative pain range as high as 28%, 5 with an overall complication rate of 13.4% according to a large meta-analysis. 17 Reporting on trochleoplasty, Donell et al 6 found a dismal 20% rate of return to full sport and a 59% reoperation rate, despite excluding removal of hardware from that calculation.
Testa et al 20 and Song et al 17 compared outcomes for both trochleoplasty-based and nontrochleoplasty-based treatments. In a systematic review, Testa et al’s 20 compared trochleoplasty to MPFL reconstruction and found no statistical difference in dislocation or instability events between the groups. Song et al 17 identified fewer recurrent dislocations (1% vs 16%, respectively) but worsened postoperative range of motion with trochleoplasty when compared with all nontrochleoplasty procedures. These results demonstrate similar redislocation rates for nontrochleoplasty-based treatments to our cohort. Therefore, based on our results and comparisons with previous literature, we believe that our technique of anteromedialization tibial tubercle osteotomy with MPFL imbrication is an alternative option that can be used in place of trochleoplasty-based procedures for the treatment of patellar instability due to trochlear dysplasia. When these surgical techniques fail, consideration should be taken to evaluate whether a competent MPFL exists and whether reconstruction is appropriate. Trochleoplasty may also be considered, as the proposed technique does not preclude future trochleoplasty.
There are limitations within our study. First, it is a retrospective review, and therefore, no direct comparison with a control group was possible. We also did not gather preoperative outcome scores to make a comparison postoperatively. However, our postoperative patient-reported outcome scores compare favorably with previously reported data. While the Kujala score has been reported for patellar instability, the KOOS and WOMAC have traditionally been used for knee cartilage injuries and arthritis; therefore, their application for patellar instability may be limited. We included patients from 4 different surgeons to increase the patient cohort in our study, but all shared a standard surgical technique. Finally, our study was underpowered to perform advanced statistical analysis such as multiple logistic regression, which could have given us information on preoperative risk factors for failure.
Conclusion
Anteromedialization tibial tubercle osteotomy with MPFL imbrication can improve recurrent patellofemoral instability and provide significant clinical benefit to patients with trochlear dysplasia.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: J.D.H. has received consulting fees from Elsevier and DePuy Synthes and educational support from DePuy Synthes. M.P.L. has received educational support from Arthrex and hospitality payments from Stryker. C.B.M. has received consulting fees from Zimmer and Linvatec; research support from Histogenics, Moximed, and Zimmer; and hospitality payments from Arthrex. A.L.Z. has received consulting fees from Stryker and hospitality payments from Arthrex and Zimmer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of California, San Francisco, Human Research Protection Program Institutional Review Board (No. 15-17796).