
Abstract
Background:
There is significant discrepancy in the reported vascularity within the meniscus, and a progressively diminishing blood supply may indicate a differential healing capacity of tears that is dependent on the affected meniscal zone.
Purpose:
To examine the outcomes after inside-out meniscal repair in all 3 meniscal vascularity zones.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients were included if they underwent inside-out meniscal repair by a single surgeon between 2010 and 2014 and had a minimum 2-year follow-up. Patients were divided into 3 groups based on the meniscal tear location (red-red, red-white, and white-white zones) as determined during an intraoperative assessment. Patient-reported outcome scores were obtained at final follow-up.
Results:
A total of 173 patients (mean age, 33.6 ± 14.3 years) were included, with a mean follow-up of 2.9 ± 0.9 years. All patients demonstrated significant improvements with inside-out meniscal repair from preoperatively to postoperatively, regardless of the meniscal tear location. Patients who underwent meniscal repair in the red-red and red-white zones had significantly increased postoperative Tegner, Lysholm, and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores compared with patients who underwent meniscal repair in the white-white zone (P < .05). Patients who underwent acute repair (≤6 weeks) demonstrated significantly higher improvements on the Tegner activity scale (acute: 5.8 ± 2.2; chronic: 4.6 ± 2.2; P = .001) and Lysholm score (acute: 85.6 ± 13.3; chronic: 80.8 ± 13.5; P = .025) compared with patients treated beyond 6 weeks from injury, regardless of the meniscal tear zone. Patients with grade IV femoral condyle chondral lesions at the time of surgery had significantly inferior outcomes compared with patients with grade I through III chondral lesions, regardless of the meniscal tear zone. Three patients (1.7%) subsequently underwent revision inside-out repair, and 3 (1.7%) underwent partial meniscectomy.
Conclusion:
Patients who underwent inside-out meniscal repair demonstrated significant improvements on subjective outcome measures at a minimum 2-year follow-up, regardless of the meniscal tear zone. Inside-out meniscal repair is recommended for potentially reparable meniscal tears in all 3 vascular zones; however, improved outcomes can be achieved when performed acutely, in the absence of full-thickness femoral condyle chondral injuries, and in the red-red and red-white zones.
Meniscal tears are the most common knee abnormality, with a mean annual incidence of 66 per 100,000 people. 16 The importance of the meniscus cannot be understated because approximately 40% to 60% of the tibiofemoral load is transmitted onto the menisci, 31 potentially increasing up to 90% of the load in deep knee flexion. 4,19,23,33 It is widely reported that osteoarthritis progresses more rapidly in the absence of a functional meniscus. 14 Therefore, it is important to promptly identify and repair meniscal tears when possible because these could significantly affect the longevity of the joint. 26 Recent studies have demonstrated excellent clinical outcomes after the repair of vertical and more complex meniscal tears. 10,24
The reported blood supply for the medial meniscus involves 20% to 30% of the periphery, while the vascular supply for the lateral meniscus is 10% to 25% of its periphery. 1 The central 70% to 75% of both menisci has been reported to receive nutrition via diffusion only. 1 Consequently, there is significant variability in the reported vascularity within the meniscus, with the peripheral tissue (“red-red” and “red-white” zones) being more vascular than the central zone (“white-white” zone). 3,27,28,30 This progressively diminishing blood supply thereby indicates a differential healing capacity of tears, dependent on the affected meniscal tear zone.
Animal models have demonstrated that meniscal tears heal in a manner similar to other connective tissue. 2,5,20 Theoretically, these tears require vascularization to provide the biological factors necessary for tissue repair. However, animal studies have also demonstrated that meniscal tissue may be able to heal without significant vascular contributions. In this regard, prior studies have demonstrated that meniscal repair outcomes were comparable in patients with and without a concomitant ligamentous injury, 6,10,11 which further demonstrates that patients undergoing meniscal repair can achieve good outcomes (with a concomitant ligamentous injury) and without (no concomitant ligamentous injury) biological enhancement. Therefore, tear extension into the avascular zone is not a contraindication for repair, particularly in the young and active patient, because of the clinical benefits of meniscal preservation. 11
The majority of the current literature has examined the outcomes of meniscal repair in the red-red and/or red-white zones. The purpose of this study was to examine the outcomes after inside-out meniscal repair in all 3 meniscal vascularity zones. Our hypothesis was that there would be no difference in outcomes between the different meniscal zones repaired.
Methods
Study Design
This study was approved by the Vail Valley Medical Center Institutional Review Board. All data were queried from a prospectively collected data registry. Patients were included if they underwent inside-out meniscal repair by the senior author (R.F.L.) between 2010 and 2014 and had a minimum 2-year follow-up. Additionally, patients were included if they underwent anterior cruciate ligament reconstruction (ACLR) during the same surgical procedure because previous literature has demonstrated outcomes of ligament reconstruction with and without meniscal repair to be comparable. Patients were also excluded from this study if they underwent prior ipsilateral or contralateral knee surgery, partial meniscectomy, and meniscal root or radial tear repair. Patients were also excluded if they presented with an associated fracture or underwent concomitant multiligament knee reconstruction, posterior cruciate ligament reconstruction (PCLR), cartilage resurfacing procedures, or osteotomy.
Patients were divided into 3 groups based on the meniscal tear location: red-red, red-white, or white-white zones (Figure 1). Acute injuries were defined as occurring ≤6 weeks from injury to surgery; chronic injuries were defined as being >6 weeks from injury to surgery. Patients with degenerative meniscal tears were excluded. The senior author determined and documented the tear type and location at the time of arthroscopic surgery.

Illustration of a lateral meniscus demonstrating the classic 3 zones according to the reported vascularity. R-R, red-red; R-W, red-white; W-W, white-white.
Surgical Techniques
Inside-out meniscal repair with vertical mattress sutures was performed in all cases. Meniscal repair was performed using a posterolateral or posteromedial approach according to a previously reported technique, depending on whether the tear was on the lateral or medial meniscus. 4 A self-delivery device fitted with a cannula (Ivy Sports Medicine) was used to pass double-loaded nonabsorbable No. 2-0 sutures into the meniscus. To pass the sutures, the knee was positioned in 20° of flexion, and the meniscal needle was advanced approximately 1 cm through the superior or inferior aspect of the meniscus; then, the knee was flexed to 70° to 90° while the needle was further advanced to help the assistant retrieve the needle through the previously made incision. The same process was repeated adjacent to the previous suture with the second needle penetrating the joint capsule, such that the sutures were placed on both the superior and the inferior borders of the meniscus between 3 to 4 mm apart to create a vertical mattress pattern. If another tear configuration was encountered, horizontal mattress sutures were utilized to maintain perpendicularity of the tear-suture complex. With the knee flexed to 90°, all sutures were tied, being cautious to not overtighten the tissue or entrap nearby soft tissue structures.
For medial meniscal repair, a vertical incision was made posterior to the medial collateral ligament, and dissection was performed to enter the interval between the medial head of the gastrocnemius and the direct arm of the semimembranosus, where a retractor was placed. For lateral meniscal repair, an incision was made along the inferior aspect of the iliotibial band, and the interval between the lateral gastrocnemius tendon and the posterolateral capsule, proximal to the biceps femoris, was entered, where a retractor was placed (Figure 2). All sutures were tied directly over the joint capsule. 8 The ACLR technique used in this study has been previously reported and validated. 6,7 Grade IV chondral lesions were treated with chondroplasty if the edges were unstable.

Arthroscopic image of a right knee demonstrating inside-out meniscal repair in the red-white zone of the meniscus.
Patient-Reported Outcomes, Patient Satisfaction, and Failure Rates
At a minimum of 2 years after the index surgery, patients were administered a subjective questionnaire that included the following clinical outcome measures: the Lysholm score, the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), the 12-Item Short Form Health Survey (SF-12) Physical Component Summary (PCS), the Tegner activity scale, and patient satisfaction with the outcome. Patient satisfaction was measured on a 1-to-10 scale, with 1 being very unsatisfied and 10 being very satisfied. Demographic characteristics were also recorded, such as age, sex, body mass index (BMI), previous surgery, tear zone (Figure 3), and meniscus of interest (medial or lateral). Meniscal repair failure was defined as any subsequent surgery for recurrent meniscal tears. Retear rates were calculated by dividing the number of patients requiring additional meniscal surgery in each zone of injury by the total number of patients in each zone of injury. Complications were recorded, including deep vein thrombosis or arthrofibrosis requiring lysis of adhesions.
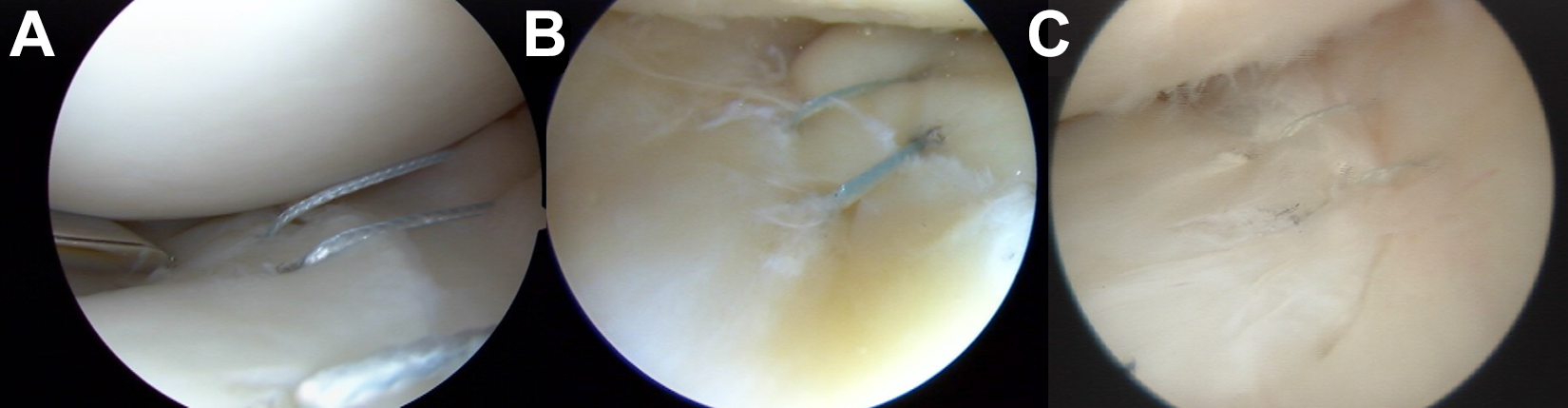
Arthroscopic view of inside-out meniscal repair with vertical mattress sutures performed on the 3 different vascularity zones: (A) white-white, (B) red-white, and (C) red-red.
Rehabilitation
For all patients, physical therapy began within 24 hours after surgery to initiate early range of motion (ROM), muscle reactivation, and edema control. For patients who had undergone isolated meniscal repair, all were nonweightbearing for 6 weeks in a knee immobilizer after surgery. ROM outside the immobilizer was restricted from 0° to 90° for the first 2 weeks, followed by a progressive increase in knee ROM. Stationary cycling began at week 6, with generalized knee strengthening focused on endurance and progressing to strength and hypertrophy. The time to return to full activities after isolated meniscal repair was from 5 to 6 months postoperatively. For rehabilitation after meniscal repair with concomitant ACLR, patients were weightbearing as tolerated with the use of crutches for 2 weeks. ROM was not restricted, and patients were allowed to progress in knee ROM as tolerated. Patients returned to full activities around 7 to 9 months after combined meniscal repair and ACLR after passing a functional sports test. 12
Statistical Analysis
A power analysis was performed a priori. Assuming an alpha of 0.05 and an independent-samples t test, 23 patients per group was sufficient to detect an effect size of d = 0.85 with 80% statistical power. Data were tested for normal distribution using the Kolmogorov-Smirnov Z test. For preoperative versus postoperative comparisons of dependent variables, the paired-samples t test was utilized for normally distributed data, and the Wilcoxon signed-rank test was utilized for nonnormally distributed data. The pre- and postoperative SF-12 PCS scores for patients in each meniscal tear zone were analyzed with analysis of variance. The pre- and postoperative Lysholm, Tegner, and WOMAC scores for patients in each meniscal tear zone were analyzed using the Kruskal-Wallis test. Comparisons of categorical data, including age, sex, BMI, and tear pattern, were performed using the chi-square test and Fisher exact test. All P values were 2-tailed, and P values of <.05 were considered statistically significant. A post hoc analysis utilizing the Tukey honest significant difference test was performed after finding any statistically significant results. All statistical analyses were performed using SPSS version 9.4 (IBM).
Results
Demographics and Meniscal Injury Patterns
Between 2010 and 2014, there were 185 patients identified as eligible for this study; 12 patients were lost to follow-up. Thus, 173 patients were included in the analysis: 112 male and 61 female patients with a mean age of 33.6 ± 14.3 years (range, 16-65 years) and a mean follow-up of 2.9 ± 0.9 years (range, 2-6.3 years). There were 60 patients (34.7%) with meniscal tears in the red-red zone, 80 patients (46.2%) with meniscal tears in the red-white zone, and 33 patients (19.1%) with meniscal tears in the white-white zone. A total of 86 patients (49.7%) underwent isolated meniscal repair, while 87 patients (50.3%) underwent combined meniscal repair and ACLR. There was no significant difference in the frequency of concurrent ACLR between the 3 zones of meniscal injury (P = .189). The majority of patients (n = 108; 62.4%) had an acute injury (≤6 weeks), while 65 patients (37.6%) had a chronic injury (>6 weeks). There was no correlation between acuity of the tear and its location. There were 25 patients (14.5%) with a grade IV chondral lesion present on the distal femur (medial or lateral femoral condyle) at the time of meniscal repair.
There were no significant differences among the 3 study groups regarding patient sex (P = .078) or BMI (P = .546). Patient demographics and clinical characteristics are presented in Table 1. The mean number of sutures used for repair was 7.7 (range, 2-18) in the red-red zone, 8.9 (range, 2-22) in the red-white zone, and 3.8 (range, 2-8) in the white-white zone.
Patient Demographics and Characteristics by Meniscal Tear Location a

a Data are shown as n (%) unless otherwise indicated.
b Statistically significant difference in the rate of each demographic analyzed (P < .05).
Analysis by Zone and Morphology of Meniscal Tear
Overall, there was a significant difference in the frequency of each meniscal tear type (vertical, horizontal, and bucket-handle) in the different zones (P = .039). Specifically, we observed a significantly greater number of horizontal tears in the white-white zone compared with the red-white and red-red zones (both P < .001). However, there were no significant differences between the 3 tear zones with respect to the frequency of bucket-handle or vertical tears (P > .05). A detailed post hoc analysis of patient-specific outcomes for each meniscal tear zone is provided in Table 2.
Post Hoc Analysis Comparing Outcomes by Meniscal Tear Location a

a SF-12 PCS, 12-Item Short Form Health Survey Physical Component Summary; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Statistically significant difference when comparing the red-white and white-white zones (P < .05).
c Statistically significant difference when comparing the red-red and white-white zones (P < .05).
All patients demonstrated significant improvements in their outcome scores from preoperatively to postoperatively, regardless of the zone of meniscal injury (P < .001) (Table 3). Subjective outcomes after inside-out repair of meniscal tears in the red-red and red-white zones were significantly improved compared with the outcomes of patients with tears in the white-white zone (P < .05). The preoperative to postoperative improvement in subjective outcome scores for all 3 meniscal tear zones met the minimal clinically important difference (MCID) for the SF-12 PCS (4.5), 34 WOMAC (11.5), 34 and Lysholm score (10.1). 34
Preoperative and Postoperative Outcome Scores by Meniscal Tear Location a
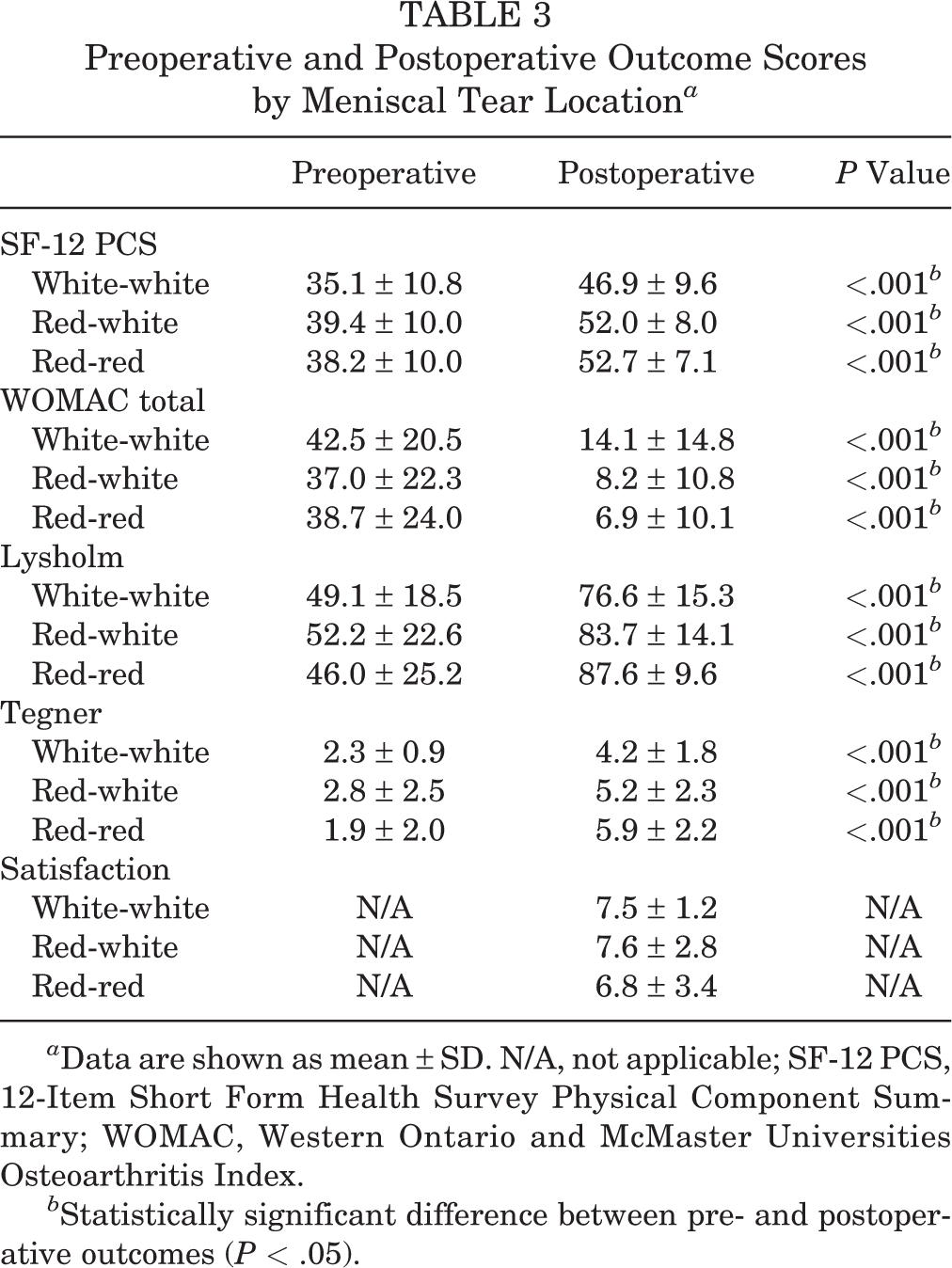
a Data are shown as mean ± SD. N/A, not applicable; SF-12 PCS, 12-Item Short Form Health Survey Physical Component Summary; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Statistically significant difference between pre- and postoperative outcomes (P < .05).
Concurrent ACLR Analysis
A subgroup analysis was performed to evaluate the effect of ACLR (n = 87; 50.3%) on postoperative outcomes by zone of meniscal injury (Table 4). In both the red-red and red-white zones, there was no significant difference in outcomes between patients who underwent isolated meniscal repair and those who underwent concurrent meniscal repair and ACLR (both P > .05). Given the small sample size of repairs in the white-white zone, there was insufficient power to subanalyze these patients.
Postoperative Outcome Scores by Meniscal Repair Location, Stratified by the Presence or Absence of Concurrent ACLR a

a Data are shown as mean (range). ACLR, anterior cruciate ligament reconstruction; N/A, not applicable; SF-12 PCS, 12-Item Short Form Health Survey Physical Component Summary; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Chronicity of Meniscal Repair Analysis
Across all zones of meniscal injury, there was a significantly greater number of meniscal repairs performed in the acute phase than the chronic phase (P = .004). There was a significantly greater number of red-red zone repairs performed acutely compared with white-white zone repairs (P = .005). Patients who underwent acute repair (≤6 weeks) demonstrated significantly higher improvements on the Tegner activity scale (acute: 5.8 ± 2.2; chronic: 4.6 ± 2.2; P = .001) and Lysholm score (acute: 85.6 ± 13.3; chronic: 80.8 ± 13.5; P = .025) compared with patients treated beyond 6 weeks from injury, regardless of the meniscal tear zone. Patients who underwent acute meniscal repair had superior outcomes compared with those who underwent chronic meniscal repair (P = .003) (Table 4).
Grade IV Chondral Lesion Analysis
There was a significantly greater number of grade IV chondral lesions in patients with tears in the white-white zone versus the red-red zone (P = .004). However, there were no significant differences in the number of grade IV chondral lesions between the red-white zone and either the white-white (P = .028) or red-red (P = .058) zones. Regardless of the meniscal tear zone, patients without grade IV femoral condyle chondral lesions displayed significant improvements in outcomes on the SF-12 PCS (grade IV: 47.2 ± 8.9; no grade IV: 52.6 ± 7.5; P = .027) and WOMAC total (grade IV: 16.2 ± 16.0; no grade IV: 7.5 ± 7.3; P = .048) compared with patients with grade IV chondral lesions.
Complications/Failures
Complications and/or failures were reported in 19 patients (11.0%) after their index surgery: 9 patients (5.2%) underwent lysis of adhesions for arthrofibrosis, 6 patients (3.5%) underwent a second surgical procedure for failed inside-out meniscal repair (Table 5), 3 patients (1.7%) underwent revision ACLR, and 1 patient underwent PCLR (0.6%). All patients who underwent surgery for arthrofibrosis had undergone concomitant ACLR and meniscal repair at the time of their index surgery. Failures were noted in 6 patients (3.5%) at a mean of 22 months from the time of repair to the retear; all failures occurred in repairs of the medial meniscus. A reinjury (n = 4) was the most common reason for meniscal retears; of these, 2 patients underwent revision inside-out meniscal repair, while the other 2 underwent partial meniscectomy (Table 5). All 3 patients who underwent revision ACLR reported a new injury at a mean of 31 ± 7.7 months after primary ACLR. The 1 patient who underwent PCLR reported a new injury 3 years after primary meniscal repair and ACLR; the anterior cruciate ligament graft and meniscal repair site were intact during the second surgical procedure.
Patients With Failed Inside-Out Meniscal Repair a

a All retears were noted in the medial meniscus. Acute: ≤6 weeks; chronic: ≥6 weeks. MM, medial meniscus; PMM, partial medial meniscectomy.
Discussion
The most important finding of this study was that patient-reported outcomes improved significantly at a minimum of 2 years after inside-out meniscal repair, regardless of the vascular zone of the meniscal tear. However, patients who underwent meniscal repair in the red-red and red-white zones displayed significantly improved outcomes compared with patients who underwent meniscal repair in the white-white zone. Furthermore, patients who underwent acute meniscal repair had significantly improved outcome scores compared with patients who underwent chronic meniscal repair, regardless of the tear location. Finally, the presence of grade IV femoral condyle cartilage lesions at the time of surgery predicted worse outcomes after repair.
The preoperative to postoperative improvement in subjective outcome scores for all 3 meniscal tear zones met the MCID for the SF-12 PCS (4.5), WOMAC (11.5), and Lysholm score (10.1). 34 These findings are supported by previous studies that reported significant improvements in outcome scores, greater than or equal to their respective MCID, regardless of tear morphology. 10,24 Two recent systematic reviews found meniscal repair to yield superior long-term results with low failure rates (10%). 25,26 Moreover, long-term outcomes become more important when considering that meniscal tears are often seen in young patients. The current literature, coupled with the findings of this study, indicates that inside-out repair should be attempted for all potentially reparable meniscal tears, regardless of the zone of the tear or the morphology of the tear. Of note also is that resecting less meniscal tissue with a tear in the white-white zone has less of a biomechanical impact on the development of osteoarthritis compared with tears in the red-red or red-white zone.
The peripheral meniscal vascularity has been reported to diminish and become more peripheral with age. 29 Therefore, the healing potential of the meniscus depends largely on the location of the lesion and the age of the patient. 1,18 Because of their higher vascularity, peripheral meniscal tears (red-red zone and peripheral part of red-white zone) have been reported to have the greatest potential for healing, 18 and they are typically treated with repair. In contrast, tears in the white-white zone have often been treated with debridement and partial meniscectomy, given the lower likelihood of successful healing of repair in avascular tissue. 13 However, recent studies have demonstrated that the repair of meniscal tears in the avascular white-white zone yielded satisfactory outcomes either in the setting of concomitant ACLR 21 or a marrow venting procedure. 11,22 The addition of marrow venting and tunnel reaming may increase intra-articular growth factors that enhance meniscal healing.
In the present study, there were low meniscal repair failure rates, with only 6 patients (3.5%) undergoing a second surgical procedure for failed meniscal repair. Noyes et al 28 reported that 62% (18/29) of inside-out meniscal repairs in the red-white zone had normal or nearly normal characteristics for pain, swelling, jumping, and the Cincinnati score, while 38% (11/29) were documented as failures at a mean follow-up of 16.8 years. Taken with the findings of the present study, clinicians can expect improved outcomes with low revision rates after inside-out meniscal repair for a range of tear morphologies 10,24 and zones.
The results of the present study suggest that patient-specific factors, including chronicity of the mensical injury and the presence of grade IV chondral lesions, may be of more clinical importance than the meniscal injury location. In a systematic review by Barber-Westin and Noyes, 3 a total of 637 meniscal repairs were evaluated. The range in the healing rates was high; however, age, chronicity of injury, involved tibiofemoral compartment, sex, and ACLR were not demonstrated to adversely affect the results.
This study has some limitations. Patients were only available for 2-year clinical follow-up, absent of examinations by second-look arthroscopic surgery or magnetic resonance imaging, and no multivariate analysis was performed to identify potential confounding variables. Patients did not return for follow-up magnetic resonance imaging, which previous studies have shown to be useful in the evaluation of meniscal repair healing. 9,15,17,32 The lower number of meniscal repairs in the white-white zone weakens the direct comparison with patients who underwent meniscal repair in the red-white and red-red zones. However, this mimics the clinical scenario, in which most reparable meniscal tears are in the red-red and red-white zones. Furthermore, 50.3% of patients in this study underwent concomitant ACLR; this may influence the generalizability of meniscal repair outcomes.
Conclusion
Patients who underwent inside-out meniscal repair demonstrated significant improvements in subjective outcome scores and a low revision rate at a minimum 2-year follow-up, regardless of the tear zone. Although worse outcomes were observed in the white-white zone relative to the others, inside-out meniscal repair is recommended for potentially reparable meniscal tears in all 3 vascular zones; however, improved outcomes can be achieved when repair is performed acutely and in the absence of full-thickness femoral condyle chondral injuries.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.F.L. is a consultant for and receives royalties from Arthrex, Ossur, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Vail Valley Medical Center Institutional Review Board (protocol 2002-03).