
Abstract
Background:
Recently, interest has increased in incorporating the National Institutes of Health Patient-Reported Outcomes Measurement Information System (PROMIS) outcomes into clinical and research applications in sports medicine. The PROMIS forms have not been studied in pediatric and adolescent sports medicine patients.
Purpose/Hypothesis:
The goal of this study was to determine the correlation between PROMIS Computer Adaptive Test (CAT) forms measuring physical function, pain interference, and depression in pediatric and adolescent patients seen in the ambulatory sports medicine clinic. We hypothesized that there would be a negative correlation between physical function and pain interference as well as depression, as has been demonstrated in adult patient populations.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
All patients aged 8 to 17 years seen by 3 shoulder and sports medicine providers were included in this study. Patients completed a series of PROMIS CAT forms at clinic visits, including the PROMIS-PF and PROMIS-UE (Physical Function and Upper Extremity; depending on the nature of the complaint), PROMIS-PI (Pain Interference), and PROMIS-Depression subscales. Pearson correlation coefficients were calculated between the PROMIS forms as well as with other patient demographic data.
Results:
A total of 236 patient visits (152 patients) were included in the study, comprising 712 total PROMIS CAT forms. A negative correlation was found between PROMIS-PF and both PROMIS-Depression (R = –0.34) and PROMIS-PI (R = –0.76). These correlations with PROMIS-Depression and PROMIS-PI were –0.21 and –0.75, respectively, when considering the PROMIS-UE CAT. Patient demographic information had minimal impact on PROMIS scores as well as on correlations between scores.
Conclusion:
Correlations between physical function, pain interference, and depression were found to be similar in pediatric patients as they are in adult patients, as measured by PROMIS CAT forms.
A significant proportion of patients in ambulatory sports medicine clinics are pediatric and adolescent patients between the ages of 8 and 17 years. Numerous recent studies have documented the well-publicized increase in rates of sports-related and overuse injuries. 3,6,8 In this patient population, the goal of treatment is to improve pain and restore functional and athletic capabilities. Although return to sport remains an important milestone in the assessment of treatment efficacy, 12,13 patient-reported outcome (PRO) scores comprise a valuable tool in quantitatively measuring response to treatment.
Despite the mainstream use of PRO scores in clinical and research sports medicine, little research has been performed on application of PRO scores in the pediatric sports medicine population. In fact, in a 2017 review of studies of pediatric anterior cruciate ligament reconstruction, Brusalis and colleagues 4 identified pediatric-focused PRO scores as comprising a very small proportion of documented PRO scores. Moreover, in a 2018 study regarding outcome reporting in pediatric orthopaedics, the authors noted that nonpediatric validated PRO scores continue to be used with frequency in this patient population. 16
Recently, increased attention has been paid to the National Institutes of Health Patient-Reported Outcomes Measurement Information System (PROMIS) scores and their incorporation into modern orthopaedics from a clinical and research perspective. In particular, PROMIS Computer Adaptive Testing (CAT) forms tailor the questions posed to the patient by using previous responses and a bank of questions. This allows for accurate responses in fewer questions answered. Numerous studies have demonstrated improved efficiency when using these scores compared with traditional, lengthier PRO scores, without loss of psychometric properties. 7 The use of these scores in the pediatric and adolescent sports medicine population has not been extensively studied, however. 17 In a recent validation study of PROMIS Physical Function (PROMIS-PF) and Upper Extremity (PROMIS-UE) forms in patients with glenohumeral instability, the researchers included pediatric and adolescent patients (age range of 12-54 years in the total patient cohort) and found that younger patients demonstrated a higher likelihood of ceiling effect with the PROMIS-UE form. 1 Therefore, the need for dedicated study of these increasingly popular PROMIS forms in pediatric and adolescent patients is justified.
The goal of this study was to examine the correlation of PROMIS-PF, PROMIS Pain Interference (PROMIS-PI), and PROMIS-Depression CAT forms in pediatric and adolescent patients in the ambulatory sports medicine clinic. We hypothesized that there will be an inverse correlation between physical function and both pain interference and depression scores, as has been found in numerous studies in adult patients. 5,9,10,15,20
Methods
All patients 17 years of age or younger presenting to an orthopaedic sports medicine ambulatory clinic of 3 providers were recruited for the study. Recruitment was done at a single, multisite institution between July 2017 and November 2017. Surveys were administered upon check-in for the office visit prior to the evaluation. Survey forms were completed on a tablet computer (iPad tablet; Apple). Those patients or guardians who could not communicate (read and write) in English or who refused participation were excluded from the study.
All study data were collected and managed through use of Research Electronic Data Capture (REDCap), a secure, web-based application designed to support data capture for research studies hosted at our institution. These surveys included an intake form asking for the name of the patient’s provider and location of pain followed by a CAT set consisting of PROMIS-PF for patients with lower extremity concerns or PROMIS-UE for patients with upper extremity concerns, PROMIS-PI, and PROMIS-Depression (Table 1).
PROMIS Domain Definitions a

a PROMIS, Patient-Reported Outcomes Measurement Information System. Data are from Northwestern University. 11
Patient sex, age, race, ethnicity, body mass index (BMI), tobacco use, employment status, and the diagnosis of the presenting concern were retrospectively collected from the electronic medical record (EMR). Tobacco use, including any form, was recorded as never, current, or former use. Employment status was recorded as employed or unknown. Patients with documented employment were designated as employed, while those listed as unemployed or without EMR employment documentation were collectively categorized as unknown. Median household income (MHI) was recorded as the MHI of the patient’s ZIP code. This information was publicly available online (https://factfinder.census.gov/faces/nav/jsf/pages/community_facts.xhtml?src=bkmk). Primary diagnosis and chronicity were determined from a chart review of the clinic visit during which the survey was collected. The chronicity of the diagnosis was recorded as acute (if present for ≤6 weeks) or chronic (if present for >6 weeks).
Statistical Analysis
All statistical analysis was conducted by one of the authors who was trained in statistics (J.S.). Continuous data, consisting of PROMIS outcomes, were compared between groups by use of 1-way analyses of variance and independent t tests, with P ≤ .05 denoted as a statistically significant difference. All analyses were performed using Stata, version 14. Pearson correlations were performed to investigate the relationships between PROMIS scores. Correlation coefficients were interpreted based on previously published medical statistics literature, with absolute values of 0.00 to 0.30 representing a negligible correlation, 0.31 to 0.50 a weak correlation, 0.51 to 0.70 a moderate correlation, 0.71 to 0.90 a strong correlation, and 0.91 to 1.00 a very strong correlation. 14
Results
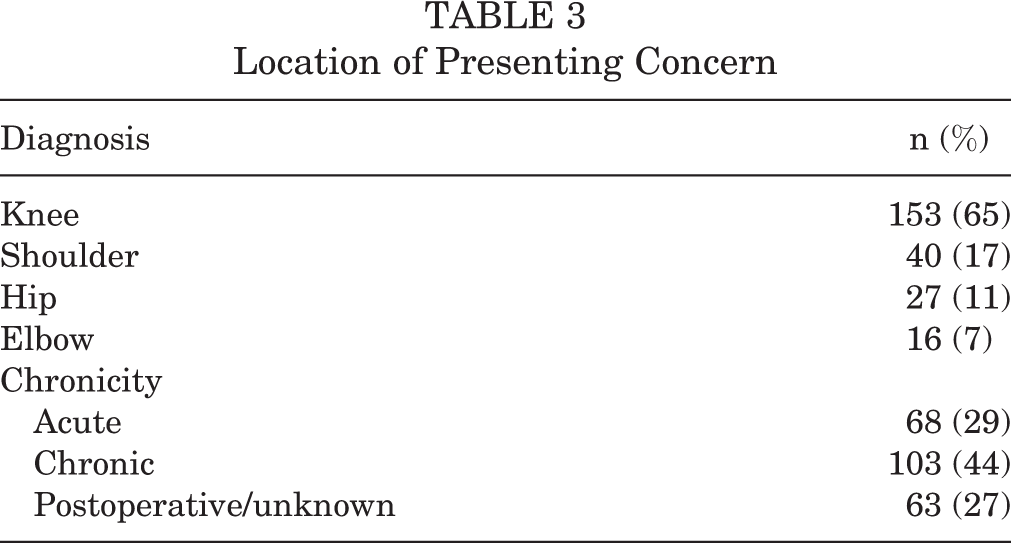
A total of 236 CAT questionnaire sets (PROMIS-PF and/or PROMIS-UE, PROMIS-PI, and PROMIS-Depression) were collected and analyzed from 152 unique patients (Table 2), totaling 712 PROMIS forms. In 4 instances, a patient identified an upper and a lower extremity concern, resulting in the completion of both PROMIS-PF and PROMIS-UE. The mean ± SD age of the patients surveyed was 15.5 ± 1.5 years (range, 8-17 years), with 58% male and 42% female participants. The MHI was $67,326 ± $24,504 (range, $20,891-$130,699). The average BMI of our population was 24.6 ± 4.6 kg/m2 (range, 15.5-39.4 kg/m2), and 58% of the patients identified as white, with the predominant ethnicity being non-Hispanic (68%). A total of 11 (5%) of the questionnaire sets were completed by patients with documented employment. The majority of patient surveys (96%) stated they had never used tobacco. The most frequent presenting concerns were those of the knee, followed by the shoulder, hip, and elbow (Table 3).
Patient Demographic Characteristics a

a Values are expressed as mean ± SD (range) or n (%). Data are derived from 236 questionnaire sets from 152 patients.
Location of Presenting Concern
Patients were asked to answer the most questions while taking the PROMIS-Depression (7.6 ± 3.8). This was followed by PROMIS-UE, PROMIS-PI, and PROMIS-PF. The average number of questions completed per PROMIS domain is shown in Table 4.
Number of Questions Completed Per PROMIS Domain a

a PROMIS, Patient-Reported Outcomes Measurement Information System.
Table 5 summarizes PROMIS correlations as each domain relates to the other domains, age, BMI, and MHI. PROMIS-PF was found to have a strong negative correlation with PROMIS-PI (R = –0.76, P < .001) and a weak correlation with PROMIS-Depression (R = –0.34, P < 0.001). The stronger correlation between PROMIS-PF and PROMIS-PI suggests that these domains are more closely represented by a linear relationship compared with that of PROMIS-PF and PROMIS-Depression. PROMIS-UE also had a strong negative correlation with PROMIS-PI (R = –0.75, P < .001). PROMIS-PI was weakly correlated with PROMIS-Depression (R = 0.45, P < .001).
Correlations Between PROMIS Domains a

a BMI, body mass index; MHI, median household income; PF, Physical Function; PI, Pain Interference; PROMIS, Patient-Reported Outcomes Measurement Information System; UE, Upper Extremity.
b No correlation because of only 4 pairings.
c Denotes a statistically significant finding (P ≤ .05).
Data were analyzed for each patient’s first survey administration. Table 6 summarizes PROMIS correlations as each domain relates to the other domains for the first PROMIS CAT set completed by each patient. PROMIS-PF was found to have a moderate negative correlation with PROMIS-PI (R = –0.69, P < .001). PROMIS-UE had a strong negative correlation with PROMIS-PI (R = –0.79, P < .001) and was weakly correlated with PROMIS-Depression (R = –0.32, P < .05). PROMIS-PI had a weak positive correlation with PROMIS-Depression (R = 0.45, P < .001).
Correlations Between PROMIS Domains on First Questionnaire Set a
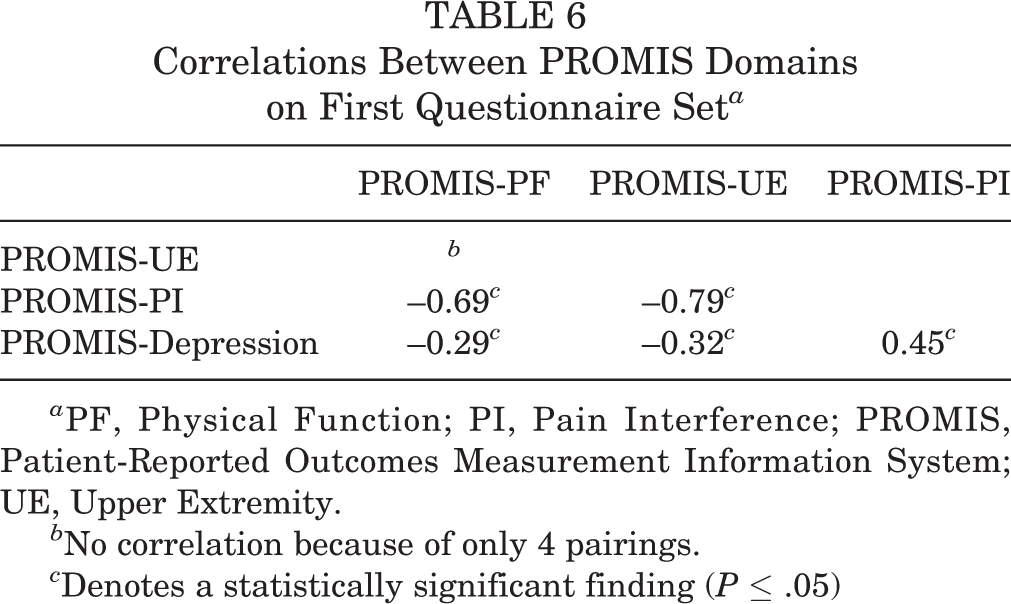
a PF, Physical Function; PI, Pain Interference; PROMIS, Patient-Reported Outcomes Measurement Information System; UE, Upper Extremity.
b No correlation because of only 4 pairings.
c Denotes a statistically significant finding (P ≤ .05)
When the sample was stratified by patient demographics, black patients had significantly higher PROMIS-UE scores compared with white patients and the patient group “Other” (49.6, 38.5, and 37.1, respectively; P < .05). No statistically significant differences in scores were found between sexes, acute and chronic conditions, or age, BMI, and MHI quartiles across all PROMIS domains. These relationships are represented in Table 7.
Impact of Patient-Centric Factors on PROMIS a

a Data are expressed as mean ± SD unless otherwise noted. BMI, body mass index; MHI, median household income; PF, Physical Function; PI, Pain Interference; PROMIS, Patient-Reported Outcomes Measurement Information System; UE, Upper Extremity.
b Denotes a statistically significant finding (P ≤ .05).
Table 8 summarizes PROMIS correlations stratified by sex, race, and the chronicity of presenting concern. PROMIS-PF was found to strongly negatively correlate with PROMIS-PI in both males and females (R = –0.72 and –0.80 respectively, P < .001). PROMIS-UE had a strong negative correlation with PROMIS-PI in males (R = –0.76, P < .001) while having a moderate negative correlation in females (R = –0.58, P < .05). Female patients had a moderate positive correlation between PROMIS-PI and PROMIS-Depression, while this was a weak correlation in males (R = 0.52 and 0.39, respectively; P < .001).
Correlations Between PROMIS Domains Stratified by Patient-Centric Factors a

a PF, Physical Function; PI, Pain Interference; PROMIS, Patient-Reported Outcomes Measurement Information System; UE, Upper Extremity.
b No correlation because of only 4 pairings.
c Denotes a statistically significant finding (P ≤ .05).
Black patients had a moderate negative correlation between PROMIS-PF and PROMIS-PI (R = –0.68, P < .001), while this correlation was stronger in white patients and all other/unknown races (R = –0.77 and –0.76, respectively; P < .001). Similarly, the correlation between PROMIS-UE and PROMIS-PI was of moderate strength in black patients but was stronger in white patients (R = –0.61 and –0.80, respectively; P < .05). PROMIS-PF was found to have a moderately negative correlation with PROMIS-Depression in nonwhite/black patients (R = –0.53, P < .001), while the correlation between PROMIS-UE and PROMIS-Depression was moderately positive (R = 0.66, P < .05). PROMIS-PI had a moderately positive correlation with PROMIS-Depression regardless of race.
Both acute and chronic presenting concerns were found to have strong negative correlations between PROMIS-PF and PROMIS-PI, moderate negative correlations between PROMIS-UE and PROMIS-PI, and weak positive correlations between PROMIS-PI and PROMIS-Depression (P ≤ .05 for all).
Discussion
The results of this study demonstrate inverse correlations between pain interference and physical function, as well as with depression and physical function, in pediatric and adolescent sports medicine patients completing PROMIS CAT forms. These findings confirm the original study hypothesis and resemble relationships between these domains found in the adult orthopaedic literature.
There is increasing interest in understanding baseline and recovery of physical function in orthopaedic patients in relation to mental health and pain interference. Several studies in adult patients have demonstrated correlation between these domains. In a recent study of patients with spinal pain, Kendall and colleagues 10 reported a strong negative correlation between PROMIS-PI and PROMIS-PF (Pearson correlation value of –0.717). 10 Similarly, in a study of patients with nonshoulder upper extremity pain, Kazmers and colleagues 9 reported Pearson correlation coefficients between PROMIS-PI and both PROMIS-PF and PROMIS-UE of –0.60 and –0.65, respectively. 9 Similar findings were reported in patients with hallux valgus, in which PROMIS-PI and PROMIS-PF demonstrated a correlation of –0.76, compared with a correlation of –0.44 between PROMIS-Depression and PROMIS-PF. 15 These 3 studies included a largely adult-aged population. In comparison, patients in our study were between the ages of 8 and 17 years, and we found a correlation of –0.76 between PROMIS-PI and PROMIS-PF and –0.75 between PROMIS-PF and PROMIS-UE. The correlation between PROMIS-Depression and PROMIS-PF was –0.34 (and –0.21 for PROMIS-UE). Therefore, these results are similar to correlations found in the adult literature. These findings indicate that PROMIS CAT forms may be relevant to the pediatric and adolescent patient population.
The relevance of PROMIS forms in the pediatric population has been studied in non–sports medicine applications. These investigations have demonstrated usefulness of pediatric PROMIS forms in this patient population. In 1 study of 33 patients aged 6 to 17 years with congenital hand conditions, good correlation was noted between the pediatric PROMIS-UE CAT and objective measures of grip strength and pinch strength (0.60 and 0.52, respectively). The correlation between the PROMIS-UE CAT and the Michigan Hand Questionnaire (MHQ) (overall function) was noted to be 0.46, and a strong negative correlation was found between the PROMIS-UE CAT and the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire (–0.87). Although the pediatric PROMIS form was used in that study, the correlations were noted with the standard MHQ and DASH forms. Other studies in hand surgery have similarly used the pediatric PROMIS scores. 2,18,19
Our study examined standard PROMIS forms in the pediatric and adolescent population. In addition to the correlations observed and reported above, we examined the role of patient-centric factors on PROMIS score outcomes. We found that chronicity of symptoms had minimal impact on score outcomes (in patients with acute vs chronic symptom duration). We also noted minimal impact on PROMIS scores with the other metrics recorded, such as age, BMI, MHI, and race (with the exception of higher PROMIS-UE scores in black patients compared with white patients).
One additional important finding from this study was the positive correlation between PROMIS-PI and PROMIS-Depression in this patient population. Across the entire cohort, the correlation was found to be 0.45, which is considered a weak correlation. However, if stratified by sex, the correlation was significantly higher in female patients compared with male patients (0.52 compared with 0.39, respectively). In contrast, patient race and symptom chronicity had little impact on this correlation. To date, this relationship has not been studied extensively in the pediatric population. Trentacosta et al 17 previously described detrimental impacts of knee ligament surgery performed on school-aged patients, but their study did not focus on depression and pain interference in this patient population. Therefore, the findings from our study highlight the relationship between pain interference and depression, along with the potential adverse impact on physical function, in pediatric and adolescent sports medicine patients.
There are important limitations to this study. First, the data were collected according to standard clinical PRO collection procedures. Therefore, we did not document whether the patient had assistance (eg, from a family member) when completing the survey forms. Because the forms were administered in the pediatric and adolescent population, prospectively collected data about assistance would have been helpful in order to determine whether parental or guardian assistance in PRO completion had any impact on PROMIS outcomes. Second, we used the adult version of the PROMIS score. In our clinic, we use a standardized set of PROMIS forms and do not distinguish according to age. Future comparative studies between the adult and pediatric versions of the PROMIS CAT forms may be useful. Third, we did not validate the PROMIS CAT forms against legacy PRO scores or against objective outcomes. Because the purpose of this study was to investigate the correlations between pain interference, depression, and physical function in this patient population, such validation measures, while helpful, were not in the scope of the study.
Conclusion
Both pain and depression demonstrated a negative correlation with physical function as measured by PROMIS CAT forms in the pediatric and adolescent sports medicine patient population. Patient demographics and socioeconomic factors had minimal impacts on this correlation. This study justifies continued study of PROMIS CAT forms in the pediatric and adolescent sports medicine patient populations.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: E.C.M. has received educational support from Pinnacle and Smith & Nephew, receives royalties from Springer, and has received hospitality payments from Smith & Nephew and Stryker. S.M. is a consultant for DePuy Synthes and Exactech, has received educational support from Arthrex, and has received hospitality payments from Arthrex, Biomet, Conventus Orthopaedics, DePuy Synthes, Exactech, Tornier, and Zimmer. V.M. has received educational support from Arthrex and Pinnacle and has received hospitality payments from Arthrex, Pinnacle, and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Henry Ford Health System Institutional Review Board (No. 10820 and 10821).