
Abstract
Background:
Hip arthroscopic surgery has become an increasingly common surgical technique to diagnose and treat various hip abnormalities. While increased efficacy has been reported, debate remains regarding appropriate surgical indications. Multiple factors including patient demographics, surgical procedure, and underlying disease have been associated with poor surgical outcomes. Preoperative diagnostic and treatment interventions including physical therapy and injections may affect surgical indications and outcomes.
Purpose:
To identify patient characteristics and preoperative factors associated with an increased risk of early revision surgery and/or extended postoperative medical care after index hip arthroscopic surgery.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Utah’s All Payer Claims Database, a state-mandated registry containing data from all payers, including private insurance, Medicare Advantage, and Medicaid, was queried to identify patients who underwent hip arthroscopic surgery during a 3-year period (January 1, 2013, to December 31, 2015). Demographics, comorbidities, nonoperative care modalities, pain medications, and revision procedures were collected using claims data at 6 months preoperatively and 12 months postoperatively.
Results:
A total of 1283 patients who underwent primary hip arthroscopic surgery were analyzed, of whom 57.6% (n = 739) were female. Within 1 year of index surgery, 7.8% and 2.1% of patients underwent revision hip arthroscopic surgery and conversion to total hip arthroplasty (THA), respectively. Patients older than 60 years and male patients were more likely to undergo revision arthroscopic surgery (odds ratio [OR], 0.89; P < .001 and OR, 1.59; P = .04, respectively) and convert to THA (OR, 1.03; P = .01 and OR, 2.25; P = .05, respectively). Preoperative opioid use was significantly associated with increased odds of revision surgery (OR, 1.64; P = .05) and THA (OR, 2.70; P = .03). No significant relationship existed between preoperative physical therapy or intra-articular hip injections and revision hip arthroscopic surgery (OR, 1.20; P = .45 and OR, 1.18; P = .52, respectively) or conversion to THA (OR, 0.89; P = .79 and OR, 0.71; P = .46, respectively).
Conclusion:
This study showed that predictable patient factors can effectively guide preoperative decision making and may improve prognosis. Certain patient pools require optimization preoperatively, and a subset of patients appears to require additional surgical indications.
Hip arthroscopic surgery allows the treatment of many hip abnormalities, including femoroacetabular impingement (FAI), chondral defects, labral tears, and loose bodies, among others. 1,17,20,26,34 Despite the steep learning curve, its minimally invasive nature, low complication rate, and quick recovery have led to a rapid increase in utilization over the past 10 years. 4,8,23,25,29,36 While good efficacy and increased patient satisfaction occur in many populations, 8 the debate continues regarding surgical indications. 8,26 Poor outcomes include revision hip arthroscopic surgery, limited function, continued pain, and conversion to total hip arthroplasty (THA). 35,37 Negative predictors include specific demographics and procedures performed, workers’ compensation status, persistent structural abnormalities, labral deficiency, chondral damage, capsular instability, and preoperative osteoarthritis. 4,7,30,32,35
Preoperative physical therapy (PT) and diagnostic intra-articular (IA) injections have been identified as potential prognostic indicators. Insurers frequently require preoperative PT for approval, suggesting a perceived importance for surgical indications, despite a paucity of supporting data. In a small, randomized controlled pilot study, patients diagnosed with FAI were randomized to 7 weeks of supervised exercise with manual therapy versus activity modification counseling and a home exercise program. 45 Both cohorts reported significant improvements in pain and range of motion, suggesting that some hip abnormalities may be amenable to conservative management. 45 However, this study concluded that while PT may improve short-term pain and function, it does not address the underlying osseous morphology. This was supported by larger randomized clinical trial data suggesting that while PT can improve symptoms, hip arthroscopic surgery had more significant, clinically important improvements. 15
Imaging-guided IA injections may also assist surgical decision making, including the evaluation of IA versus extra-articular hip pain sources. In fact, some insurance guidelines also require these injections for approval, with guidelines based on data demonstrating that a negative response to an IA injection may be associated with a poor surgical outcome. 3 Thus, over 80% of patients undergoing hip arthroscopic surgery report receiving IA injections before surgery. 21 However, studies have contradicted these findings, 22 and minimal data exist correlating preoperative IA injections to increased postoperative revision or care.
The goals of this study were to identify demographic variables, comorbidities, and preoperative evaluation modalities (PT, IA injection) that may be associated with early revision hip arthroscopic surgery, conversion to THA, other surgical procedures, extended medical care, and prolonged pain medication usage after index hip arthroscopic surgery.
Methods
With institutional review board (#98713) approval, Utah’s All Payer Claims Database (APCD) was queried to include a 3-year period between January 1, 2013, and December 31, 2015. Patients were identified using Current Procedural Terminology (CPT) codes and included if they were ≥14 years old, continuously insured, and had claims information at 6 months preoperatively and 12 months postoperatively. Utah’s APCD is a state-mandated registry that contains claims data from all private and public payers (Medicare Advantage and Medicaid), representing 2.4 million persons and 80% of Utah’s population beginning in the year 2013. 41,43 The APCD provided 3-year longitudinal data, affording the ability to correlate large-volume preoperative factors with postoperative management in a fashion not available with other hip arthroscopic surgery studies using a large database. 19
With the date of surgery as the index date, common diagnostic indicators and conservative interventions were collected at 6 months preoperatively and 12 months postoperatively using CPT codes (Appendix Table A1). Revision hip arthroscopic surgery, conversion to THA, lumbosacral surgery, and abdominal surgery were included to capture procedures that could indicate a failure of the index surgery to satisfactorily relieve symptoms. The concern was that patients who underwent abdominal or lumbosacral surgery shortly after the index arthroscopic surgery were not properly diagnosed before the initial arthroscopic procedure was performed. Preoperative and postoperative PT, IA hip injections, epidural/facet lumbosacral injections, and pain medications (opioids, nonsteroidal anti-inflammatory drugs [NSAIDs], and skeletal muscle relaxants) were also identified and analyzed using CPT codes, National Drug Code data, and medication names.
Baseline demographic data, insurance type, urban or rural regional designation indicating where the patient lived at the time of surgery, and comorbidities were identified. Age was measured in years at index surgery, and age squared was included in the regression models because of a significant nonlinear trend in this variable’s effect on postoperative interventions. Sex was dichotomized as male or female. Comorbidities were binary and identified based on International Classification of Diseases, Ninth Revision (ICD-9), codes (Appendix Table A1). Insurance type was categorized as commercial/private or government funded (Medicaid or Medicare). Patients with dual Medicaid/Medicare enrollment (n = 11) were excluded from the analysis.
Descriptive statistics, including means, standard deviations, frequencies, and percentages, were used to describe the sample. To identify factors that were associated with the outcomes, multivariate logistic regression was used, and odds ratios (ORs) and P values were reported in the regression table. The significance level was set at .05 for all analyses using Stata statistical software (v 14; StataCorp).
Results
The analyzed sample included 3443 patients who underwent hip arthroscopic surgery between January 1, 2013, and December 31, 2015. Patients were excluded from the final analysis for the following reasons: lacked 1-year follow-up data after index surgery (n = 1030), were not continuously enrolled in insurance during the study period (n = 1028), were missing demographic data (n = 68), or were younger than 14 years at the time of index surgery (n = 34).
A total of 1283 patients who underwent primary hip arthroscopic surgery, 57.6% (n = 739) female and 42.4% (n = 544) male, were included in the final analysis (Table 1). Patients were more likely to have private insurance than Medicare or Medicaid (89.1% vs 10.9%, respectively) and live in urban rather than rural regions (88.5% vs 11.5%, respectively). Common comorbidities, identified by ICD-9 codes, included depression (23.3%), smoking (11.9%), obesity (11.6%), and diabetes (10.0%) (Table 2).
Patient Demographics (N = 1283)

Comorbidities
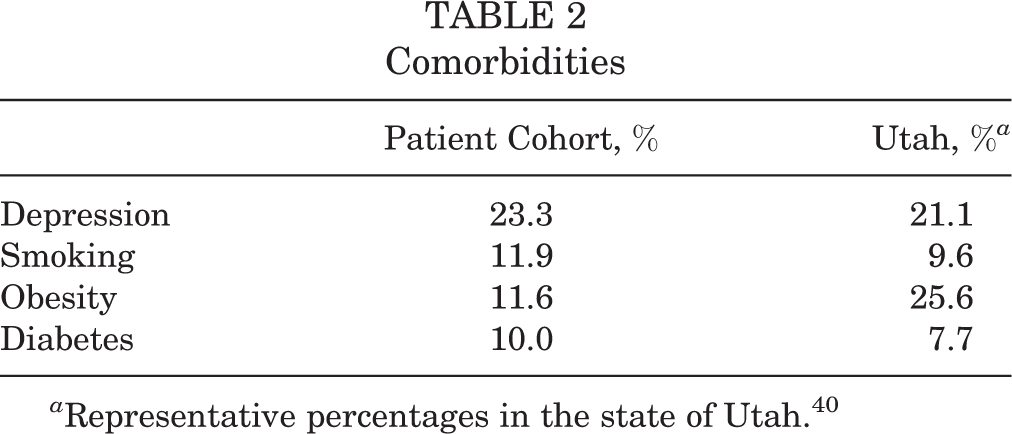
a Representative percentages in the state of Utah. 40
Of the patients included, 7.8% underwent revision arthroscopic surgery, and 2.1% converted to THA within 1 year of hip arthroscopic surgery. Additionally, 2.4% and 1.2% of patients underwent lumbosacral surgery and abdominal surgery, respectively, within 1 year of hip arthroscopic surgery (Table 3).
Additional Surgical Interventions

Injections were prevalent in the preoperative and postoperative settings (46.7% and 34.3%, respectively). IA hip injections were most common, with 45.1% and 29.5% of patients receiving at least 1 injection preoperatively and postoperatively, respectively. Lumbosacral epidural or facet joint injections increased from 1.6% preoperatively to 4.8% postoperatively (Table 4).
Preoperative and Postoperative Conservative Interventions a

a Data are reported as n (%). NSAID, nonsteroidal anti-inflammatory drug.
Preoperative PT occurred in 32.0% of patients. Extended postoperative PT occurred in 29.6% and 12.8% of patients at 4 to 6 months and 10 to 12 months, respectively. Pain medications were routinely prescribed preoperatively, with 34.4% of patients receiving opioids, 26.3% receiving NSAIDs, 10.4% receiving steroids, and 9.6% receiving skeletal muscle relaxants. Continued postoperative use of prescription opioids and NSAIDs, in particular, remained common, with 18.7% of patients still receiving opioids and 14.3% receiving NSAIDs at 4 to 6 months and 16.5% and 12.0% of patients receiving opioids and NSAIDs at 10 to 12 months, respectively (Table 4).
Both demographics and comorbidities demonstrated significant associations with postoperative interventions. As previously mentioned, the effect of age on postoperative interventions was nonlinear. Age (OR, 0.89; P < .001) and age squared (OR, 1.01 [95% CI, 1.000128-1.00167]; P = .02) indicated that as patients aged, they were significantly less likely to undergo revision arthroscopic surgery, but a threshold effect occurred at age 60 years, after which patients were significantly more likely to undergo revision arthroscopic surgery. Older age was associated with increased odds of conversion to THA (OR, 1.03 [95% CI, 1.0076-1.0613]; P = .01), lumbosacral surgery (OR, 1.03 [95% CI, 1.0043-1.0615]; P = .02), and abdominal surgery (OR, 1.38; P = .01). Male patients were more likely than female patients to undergo both revision arthroscopic surgery (OR, 1.59; P = .04) and conversion to THA (OR, 2.25; P = .05). Obese patients were significantly more likely to convert to THA (OR, 3.40; P = .02), and diabetic patients were significantly more likely to undergo lumbosacral surgery (OR, 3.60; P = .01).
Preoperative opioid use was the only medication found to be associated with increased odds of revision arthroscopic surgery (OR, 1.64; P = .05), THA (OR, 2.70; P = .03), and lumbosacral surgery (OR, 2.44; P = .04). The utilization of preoperative conservative treatments such as PT and injections was not significant (Table 5).
Results of Multivariate Logistic Regression a

a The age-squared variable was not statistically significant in total hip arthroplasty and lumbosacral surgery. Thus, we excluded the age-squared variable in these 2 regressions. N/A, not applicable; NSAID, nonsteroidal anti-inflammatory drug; OR, odds ratio.
b Significant at α = .05.
Discussion
Hip arthroscopic surgical indications are multifactorial and rely on a comprehensive patient evaluation. This study demonstrated that (1) there were preoperative patient variables, including age and sex, that affected prognosis; (2) preoperative interventions, including PT and IA injections, did not influence revision or conversion rates; (3) patients with obesity, diabetes, and opioid use were associated with higher revision and conversion rates; and (4) a subset of patients potentially required additional surgical interventions based on underlying comorbidities.
A prior large, population-based study documented an increased risk of conversion to THA within 2 years of arthroscopic surgery among patients with osteoarthritis, obesity, or treatment in a low-volume hip arthroscopic surgery institution. 35 Age and sex have also been implicated, with increased conversion to THA after hip arthroscopic surgery occurring in older patients and female patients. 25,36 However, other data have suggested that female and male patients younger than 45 years have equivalent outcomes. 14 Age and articular cartilage health appear to have a critical role; among 8.7% of patients who converted to THA within 24 months, 17.1% were between 50 and 59 years old, and 16.5% were older than 60 years. 36 Over 99% of these patients had preoperative osteoarthritis, regardless of age. 36 Conversely, improved outcomes after hip arthroscopic surgery in older populations, despite an elevated conversion rate, 10 have highlighted this controversy.
In our cohort, age and sex significantly correlated with postoperative revision hip arthroscopic surgery and conversion to THA. The age of 60 years was the threshold above which the risk for revision hip arthroscopic surgery significantly increased, in contrast to published data that suggested a 40-year age threshold. 19,34 We believe that this increased age threshold reflects an improved understanding of the importance of articular cartilage health in hip arthroscopic surgery decision making. On the other hand, conversion to THA displayed an age-based linear trend, with patients being more at risk for eventual conversion as they increased in age. This likely indicates the progressive nature of osteoarthritis that may ultimately influence the failure of the index arthroscopic procedure. 9,18,19,35,36 These data suggest a correlation of articular cartilage health to the revision rate. Prior studies 2,5,6,31 have suggested this preliminary relationship, but further research is necessary. Future prognostic studies should consider including magnetic resonance imaging or other specific measures of articular cartilage health.
Interestingly, male sex demonstrated higher rates of arthroscopic revision and conversion to THA (OR, 1.59 and 2.25, respectively). This contrasts with previous data 33,36 documenting worse outcomes in female patients but no sex difference in patients younger than 45 years. 45 It is possible that male and female patients differ in their desire to undergo surgery, perceived acceptable level of functional impairment, and risk aversion. Women undergoing orthopaedic procedures have documented worse preoperative functional status compared with men, suggesting an advanced disease at the time of the index procedure. 16 Male patients after total knee arthroplasty reported decreased 36-Item Short Form Health Survey physical scores, while female patients had lower general health scores, thus suggesting that physical and mental health might be more interrelated for female patients. 44 Male patients also had greater postoperative improvement in social function, physical role function, pain scores, energy, and mental health. 12,27 Thus, it may be possible that male patients inherently seek and benefit from earlier surgical interventions and that female patients delay before pursuing surgery and may benefit less.
Diabetic patients undergoing hip arthroscopic surgery had a greater risk of subsequent lumbosacral surgery, and obese patients were more likely to have conversion to THA. Patients in these categories could benefit from counseling to optimize glucose control and weight loss before surgery, which may affect this revision rate. A 1.2% subset of patients underwent additional abdominal surgery, suggesting that multiple causes of hip pain exist and are not always identified before hip arthroscopic surgery. Finally, preoperative opioid use was significantly associated with revision arthroscopic surgery, conversion to THA, and lumbosacral surgery. Implementing alternative pain management strategies before and after hip arthroscopic surgery may reduce these postoperative revision rates.
Our data revealed no relationship between preoperative PT or IA injections and revision surgery or extended postoperative medical care. These data may suggest that some patients who undergo hip arthroscopic surgery may have an anatomic issue that is not correctable via preoperative PT. While it is likely that patients who responded to PT and did not undergo surgery were not included in our analysis, we believe that this should make the 32.0% of the patients who had preoperative PT a more selective population that theoretically may have a more optimal postoperative course. However, this was not found. Rather, the lack of significant differences in the aforementioned variables between patients who did or did not undergo preoperative PT should represent a worst-case scenario in which patients who had no preoperative PT were compared with those who did. The lack of difference suggests that patients with underlying mechanical pathomorphology may not respond to preoperative PT and that surgical indications should be based on other factors such as history, physical examination results, and radiographic findings, among others.
A study by Mansell et al 24 in 2018 found no significant difference between patients with FAI allocated to surgery versus rehabilitation, suggesting a primary role for PT in FAI. However, their study had an unusually high rate of crossover, an underpowered “as-treated” analysis, and very small improvements in patient-reported outcomes after surgery inconsistent with previous literature, 13 making the results difficult to interpret. Our data suggest that while PT plays a role in preoperative management, it does not ultimately significantly influence outcomes in terms of the need for revision surgery or other intervention. Given this, it does not seem that PT has a primary role in managing this particular abnormality, and it is worth considering if PT should be focused during postoperative care. This could potentially reduce costs overall, avoid limiting PT visits prematurely secondary to insurance restrictions, and solve the issue of PT failure influencing surgical indications. We suggest that PT may be best allocated to postoperative recovery and advocate for re-evaluation of insurance coverage criteria that mandate preoperative PT.
Interestingly, preoperative IA injections did not significantly correlate with increased revision surgery or extended postoperative interventions. While it is possible that patients who received a negative response to IA injections did not undergo surgery and thus were not included, this would increase the difference between the IA and non-IA injection cohorts, but no significant correlation existed. Our data support previous data that documented a limited prognostic benefit to the ubiquitous use of IA injections. 22 Nevertheless, the selective use of preoperative diagnostic IA injections may remain important for patients with increased complexity and multiple pain generators, in which a negative response to injections helps steer them from surgical interventions.
The type of insurance was not significantly related to the need for revision hip arthroscopic surgery, THA, or lumbosacral surgery. Those with private insurance had an OR of 1.75 to undergo revision hip arthroscopic surgery (P = .24), an OR of 1.38 to undergo THA (P = .65), and an OR of 1.17 to undergo lumbosacral surgery (P = .76). The trend appeared to be that those with private insurance were more likely to eventually need an additional procedure, although this was not significant. There were significantly decreased odds of undergoing abdominal surgery with private insurance (OR, 0.09; P < .001). The reason for this relationship was not abundantly clear, although it is reasonable to surmise that those with public insurance have a wider range of health disparities and medical concerns and ultimately experience different postoperative hospital courses, including an increased length of stay. 11 The relationship between public insurance and overall outcome is a complex topic and one that we did not seek to address in this study. Further investigation is clearly warranted regarding whether type of insurance serves as an overall indicator of patient health status as well as the role that type of insurance plays in determining clinical outcomes.
Limitations
Our data are affected by the inherent limitations that exist with a large database analysis. 28 The APCD relies on the accuracy of CPT and ICD-9 coding by surgeons and billers in Utah, and coding errors may affect the accuracy of these data. Patients captured included those who were continuously insured and had claims information at 6 months before and 12 months after surgery. Following data beyond the 1-year mark postoperatively could provide even more insight into revision surgery and treatment utilization. However, our ability to capture data at 6 months preoperatively and 12 months postoperatively should include the majority of early failures and complications.
Furthermore, we restricted our data search to patients aged ≥14 years, and thus, these data may not be applicable to very young populations. However, hip arthroscopic surgery is rarely indicated in skeletally immature populations, and thus, we believe that our data remain generalizable. Uninsured patients and patients with fee-for-service Medicare may represent a unique subset with different outcomes that we were unable to capture within the scope of our research. However, our ability to include commercial insurance payers, Medicaid, and Medicare Advantage should provide reasonable generalizability of these results to the majority of patients. It is possible that patients may have moved to Utah State immediately before or shortly after their index surgery, which may affect data accuracy. However, the APCD is not restricted by state but rather by insurance carrier. Given this, procedures that were performed in a different state but collected by the same insurance provider would be included, thereby limiting the frequency of these events.
In addition, we were unable to evaluate individual cases, including the specific details of imaging and arthroscopic surgery. Thus, subtleties such as dysplasia and early osteoarthritis seen at the time of arthroscopic surgery could not be collected. Subtleties among variables such as degree of obesity and severity of diabetes could also not be determined because of the binary nature of ICD-9 coding. Additionally, our 1-year follow-up inevitably did not include failures and revisions that occur later than this time period. Our database does not evaluate the surgical volume of providers, as this was not available. Finally, we did not have data on whether the “index” procedure may have been a revision of a surgical procedure performed before the data set query. Despite the aforementioned limitations, the large sample size and 3-year data capture provide the unique ability to risk-stratify many patient variables. Finally, it is not possible to identify laterality of the surgical procedure (both index and revision) utilizing CPT and ICD-9/10 codes. This is a limitation in that we did not know with certainty that the revision procedure was performed on the ipsilateral limb. Our assumption, given the practices of our institution, is that a revision procedure on the ipsilateral side is more likely than an additional index procedure on the contralateral side.
Conclusion
A relationship analysis among patient demographic and postoperative variables allows the development of a preoperative surgical algorithm to optimize outcomes and guide patient expectations. Patient selection for hip arthroscopic surgery should consider other causes of hip pain, including intra-abdominal abnormalities and lumbosacral spine disease. Patients aged 40 to 60 years and especially those over 60 years may benefit from advanced preoperative imaging to evaluate articular cartilage health. Our findings encourage a comprehensive preoperative assessment including HbA1c and body mass index, and particular focus should be placed on opioid usage identification and nonopioid pain strategies. The identification of factors that may increase future revision will hopefully improve patient outcomes and reduce revisions and extended postoperative medical care.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: T.G.M. is a paid speaker/presenter for Arthrex and has received hospitality payments from Arthrex and Aesculap Biologics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the University of Utah Institutional Review Board.
APPENDIX
ICD-9 and CPT Codes and Descriptions a

| Code | Description |
|---|---|
| ICD-9 | |
| 296.0-296.99 | Episodic mood disorders |
| 309.0-309.9 | Adjustment reaction disorders |
| 311.0 | Depressive disorder, not elsewhere classified |
| 250.0-250.93 | Diabetes mellitus |
| 278.0-278.8 | Overweight, obesity, and other hyperalimentation |
| 305.1 | Tobacco use disorder |
| V15.82 | Personal history of tobacco use |
| CPT | |
| Surgical: hip | |
| 27130 | Arthroplasty, acetabular and proximal femoral prosthetic replacement (total hip arthroplasty), with or without autograft or allograft |
| 29861 | Hip arthroscopic surgery with removal of loose or foreign body |
| 29862 | Hip arthroscopic surgery with chondroplasty |
| 29914 | Hip arthroscopic surgery with femoroplasty |
| 29915 | Hip arthroscopic surgery with acetabuloplasty |
| 29916 | Hip arthroscopic surgery with labral repair |
| 29999 | Unlisted arthroscopic surgery |
| Surgical: general surgery | |
| 27299 | Other procedures on pelvis or hip joint |
| 49505 | Repair of initial inguinal hernia, age ≥5 years; reducible |
| 49568 | Implantation of mesh or other prosthesis for open incisional or ventral hernia repair or mesh for closure of debridement for necrotizing soft tissue infection |
| 49659 | Unlisted laparoscopy procedure, hernioplasty, herniorrhaphy, herniotomy |
| 49999 | Unlisted procedure, abdomen, peritoneum, and omentum |
| Surgical: gynecological/urological/colorectal | |
| 45560 | Repair procedures on colon and rectum |
| 52000 | Endoscopy-cystoscopy, urethroscopy, cystourethroscopy procedures on bladder |
| 52005 | Cystourethroscopy, with ureteral catheterization, with or without irrigation, instillation, or ureteropyelography, exclusive of radiological service |
| 52204 | Cystourethroscopy, with biopsy(s) |
| 52276 | Cystourethroscopy, with direct vision internal urethrotomy |
| 52281 | Cystourethroscopy, with calibration and/or dilation of urethral stricture or stenosis, with or without meatotomy, with or without injection procedure for cystography, male or female |
| 52310 | Cystourethroscopy, with removal of foreign body, calculus, or ureteral stent from urethra or bladder (separate procedure); simple |
| 52317 | Litholapaxy: crushing or fragmentation of calculus by any means in bladder and removal of fragments; simple or small (<2.5 cm) |
| 52318 | Litholapaxy: crushing or fragmentation of calculus by any means in bladder and removal of fragments; complicated or large (>2.5 cm) |
| 52335 | Cystourethroscopy with ureteroscopy and/or pyeloscopy |
| 52336 | Cystourethroscopy with ureteroscopy and/or pyeloscopy, with removal or manipulation of calculus (including ureteral stent) |
| 52337 | Cystourethroscopy with ureteroscopy and/or pyeloscopy, with lithotripsy (including ureteral stent) |
| 53200 | Biopsy of urethra |
| 53210 | Total urethrectomy, female |
| 53215 | Total urethrectomy, male |
| 53410 | Urethroplasty, 1-stage, of male anterior urethra |
| 54500 | Biopsy of testis, needle |
| 54505 | Biopsy of testis, incisional |
| 54530 | Orchiectomy, radical, for tumor; inguinal approach |
| 54600 | Reduction (surgical) of testis torsion |
| 54800 | Biopsy of epididymis, needle |
| 54900 | Epididymovasostomy (unilateral) |
| 55400 | Vasovasostomy |
| 55530 | Excision of varicocele or ligation of spermatic veins for varicocele |
| 55700 | Needle biopsy of prostate, single or multiple |
| 55859 | Transperineal catheter placement into prostate for brachytherapy |
| 57240 | Anterior colporrhaphy, repair of cystocele with or without repair of urethrocele |
| 57250 | Posterior colporrhaphy, repair of rectocele with or without perineorrhaphy |
| 57260 | Combined anteroposterior colporrhaphy |
| 57265 | Combined anteroposterior colporrhaphy, with enterocele repair |
| 57267 | Insertion of mesh or other prosthesis for repair of pelvic floor defect, each site (anterior, posterior compartment), vaginal approach |
| 57268 | Repair of enterocele, vaginal approach |
| 57270 | Repair of enterocele, abdominal approach |
| 57280 | Colpopexy, abdominal approach |
| 57282 | Colpopexy, vaginal; extraperitoneal approach (sacrospinous, iliococcygeus) |
| 57283 | Colpopexy, vaginal; intraperitoneal approach (uterosacral, levator myorrhaphy) |
| 57284 | Paravaginal defect repair (including repair of cystocele, if performed); open abdominal approach |
| 57285 | Paravaginal defect repair (including repair of cystocele, if performed); vaginal approach |
| 57288 | Sling operation for stress incontinence (eg, fascia or synthetic) |
| 57295 | Revision (including removal) of prosthetic vaginal graft; vaginal approach |
| 57423 | Laparoscopic paravaginal defect repair (including repair of cystocele, if performed) |
| 57425 | Laparoscopic sacrocolpopexy |
| 57426 | Laparoscopic revision (including removal) of prosthetic vaginal graft |
| 58263 | Vaginal hysterectomy, for uterus ≤250 g; with removal of tube(s), and/or ovary(s), with repair of enterocele |
| 58270 | Vaginal hysterectomy, for uterus ≤250 g; with repair of enterocele |
| 58280 | Vaginal hysterectomy, with total or partial vaginectomy; with repair of enterocele |
| 58292 | Vaginal hysterectomy, for uterus >250 g; with removal of tube(s) and/or ovary(s), with repair of enterocele |
| 58294 | Vaginal hysterectomy, for uterus >250 g; with repair of enterocele |
| 58541 | Laparoscopy, surgical, supracervical hysterectomy, for uterus ≤250 g |
| 58542 | Laparoscopy, surgical, supracervical hysterectomy, for uterus ≤250 g; with removal of tube(s) and/or ovary(s) |
| 58543 | Laparoscopy, surgical, supracervical hysterectomy, for uterus >250 g |
| 58544 | Laparoscopy, surgical, supracervical hysterectomy, for uterus >250 g; with removal of tube(s) and/or ovary(s) |
| 58548 | Laparoscopy, surgical, with radical hysterectomy, with bilateral total pelvic lymphadenectomy and para-aortic lymph node sampling (biopsy), with removal of tube(s) and ovary(s), if performed |
| 58550 | Laparoscopy, surgical, with vaginal hysterectomy, for uterus ≤250 g |
| 58552 | Laparoscopy, surgical, with vaginal hysterectomy, for uterus ≤250 g; with removal of tube(s) and/or ovary(s) |
| 58553 | Laparoscopy, surgical, with vaginal hysterectomy, for uterus >250 g |
| 58554 | Laparoscopy, surgical, with vaginal hysterectomy, for uterus >250 g; with removal of tube(s) and/or ovary(s) |
| 58570 | Laparoscopy, surgical, with total hysterectomy, for uterus ≤250 g |
| 58571 | Laparoscopy, surgical, with total hysterectomy, for uterus ≤250 g; with removal of tube(s) and/or ovary(s) |
| 58572 | Laparoscopy, surgical, with total hysterectomy, for uterus >250 g |
| 58573 | Laparoscopy, surgical, with total hysterectomy, for uterus >250 g; with removal of tube(s) and/or ovary(s) |
| 76872 | Ultrasound, transrectal |
| Surgical: lumbosacral | |
| 0195T | Arthrodesis, presacral interbody technique, disc space preparation, discectomy, without instrumentation, with image guidance (including bone graft, when performed); L5-S1 interspace |
| 0196T | Arthrodesis, presacral interbody technique, disc space preparation, discectomy, without instrumentation, with image guidance (including bone graft, when performed); L4-L5 interspace |
| 0200T | Percutaneous sacral augmentation (sacroplasty), unilateral injection(s) (including use of balloon or mechanical device, when used), ≥1 needles (including imaging guidance and bone biopsy, when performed) |
| 0201T | Percutaneous sacral augmentation (sacroplasty), bilateral injections (including use of balloon or mechanical device, when used), ≥2 needles (including imaging guidance and bone biopsy, when performed) |
| 0202T | Posterior vertebral joint arthroplasty (eg, facet joint replacement) (including facetectomy, laminectomy, foraminotomy, and vertebral column fixation, injection of bone cement, when performed), including fluoroscopy, single level, lumbar spine |
| 0219T | Placement of posterior intrafacet implant(s), unilateral or bilateral, including imaging and placement of bone graft(s) or synthetic device(s), single level: cervical |
| 0220T | Placement of posterior intrafacet implant(s), unilateral or bilateral, including imaging and placement of bone graft(s) or synthetic device(s), single level: thoracic |
| 0221T | Placement of posterior intrafacet implant(s), unilateral or bilateral, including imaging and placement of bone graft(s) or synthetic device(s), single level: lumbar |
| 0222T | Placement of posterior intrafacet implant(s), unilateral or bilateral, including imaging and placement of bone graft(s) or synthetic device(s): each additional vertebral segment |
| 0274T | Percutaneous laminotomy/laminectomy (interlaminar approach) for decompression of neural elements (with or without ligamentous resection, discectomy, facetectomy, and foraminotomy), any method, under indirect image guidance (eg, fluoroscopic, CT) with or without use of endoscope, single or multiple levels, unilateral or bilateral; cervical or thoracic |
| 0275T | Percutaneous laminotomy/laminectomy (interlaminar approach) for decompression of neural elements (with or without ligamentous resection, discectomy, facetectomy, and foraminotomy), any method, under indirect image guidance (eg, fluoroscopic, CT) with or without use of endoscope, single or multiple levels, unilateral or bilateral; lumbar |
| 0309T | Arthrodesis, presacral interbody technique, including disc space preparation, discectomy, with posterior instrumentation, with image guidance (including bone graft, when performed), lumbar, L4-L5 interspace |
| 22100 | Partial excision of posterior vertebral component (eg, spinous process, lamina or facet) for intrinsic bony lesion, single vertebral segment; cervical |
| 22101 | Partial excision of posterior vertebral component (eg, spinous process, lamina or facet) for intrinsic bony lesion, single vertebral segment; thoracic |
| 22102 | Partial excision of posterior vertebral component (eg, spinous process, lamina or facet) for intrinsic bony lesion, single vertebral segment; lumbar |
| 22103 | Partial excision of posterior vertebral component (eg, spinous process, lamina or facet) for intrinsic bony lesion, single vertebral segment; each additional segment |
| 22110 | Partial excision of vertebral body, for intrinsic bony lesion, without decompression of spinal cord or nerve root(s), single vertebral segment; cervical |
| 22112 | Partial excision of vertebral body, for intrinsic bony lesion, without decompression of spinal cord or nerve root(s), single vertebral segment; thoracic |
| 22114 | Partial excision of vertebral body, for intrinsic bony lesion, without decompression of spinal cord or nerve root(s), single vertebral segment; lumbar |
| 22116 | Partial excision of vertebral body, for intrinsic bony lesion, without decompression of spinal cord or nerve root(s), single vertebral segment; each additional vertebral segment |
| 22206 | Osteotomy of spine, posterior or posterolateral approach, 3 columns, 1 vertebral segment (eg, pedicle/vertebral body subtraction); thoracic |
| 22207 | Osteotomy of spine, posterior or posterolateral approach, 3 columns, 1 vertebral segment (eg, pedicle/vertebral body subtraction); lumbar |
| 22208 | Osteotomy of spine, posterior or posterolateral approach, 3 columns, 1 vertebral segment (eg, pedicle/vertebral body subtraction); each additional vertebral segment |
| 22210 | Osteotomy of spine, posterior or posterolateral approach, 1 vertebral segment; cervical |
| 22212 | Osteotomy of spine, posterior or posterolateral approach, 1 vertebral segment; thoracic |
| 22214 | Osteotomy of spine, posterior or posterolateral approach, 1 vertebral segment; lumbar |
| 22216 | Osteotomy of spine, posterior or posterolateral approach, 1 vertebral segment; each additional vertebral segment |
| 22220 | Osteotomy of spine, including discectomy, anterior approach, single vertebral segment; cervical |
| 22222 | Osteotomy of spine, including discectomy, anterior approach, single vertebral segment; thoracic |
| 22224 | Osteotomy of spine, including discectomy, anterior approach, single vertebral segment; lumbar |
| 22226 | Osteotomy of spine, including discectomy, anterior approach, single vertebral segment; each additional vertebral segment |
| 22532 | Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); thoracic |
| 22533 | Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); lumbar |
| 22534 | Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); thoracic or lumbar, each additional vertebral segment |
| 22548 | Arthrodesis, anterior transoral or extraoral technique, clivus-C1-C2 (atlas-axis), with or without excision of odontoid process |
| 22551 | Arthrodesis, anterior interbody, including disc space preparation, discectomy, osteophytectomy, and decompression of spinal cord and/or nerve roots; cervical below C2 |
| 22552 | Arthrodesis, anterior interbody, including disc space preparation, discectomy, osteophytectomy, and decompression of spinal cord |
| 22554 | Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); cervical below C2 |
| 22556 | Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); thoracic |
| 22558 | Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); lumbar |
| 22585 | Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); each additional interspace |
| 22586 | Arthrodesis, presacral interbody technique, including disc space preparation, discectomy, with posterior instrumentation, with image guidance (including bone graft, when performed), L5-S1 interspace |
| 22590 | Arthrodesis, posterior technique, craniocervical (occiput-C2) |
| 22595 | Arthrodesis, posterior technique, atlas-axis (C1-C2) |
| 22600 | Arthrodesis, posterior or posterolateral technique, single level; cervical below C2 |
| 22610 | Arthrodesis, posterior or posterolateral technique, single level; thoracic (with or without lateral transverse technique) |
| 22612 | Arthrodesis, posterior or posterolateral technique, single level; lumbar (with or without lateral transverse technique) |
| 22614 | Arthrodesis, posterior or posterolateral technique, single level; each additional vertebral segment |
| 22630 | Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar |
| 22632 | Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; each additional interspace |
| 22633 | Arthrodesis, combined posterior or posterolateral technique with posterior interbody technique, including laminectomy and/or discectomy sufficient to prepare interspace |
| 22634 | Arthrodesis, combined posterior or posterolateral technique with posterior interbody technique, including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; each additional interspace and segment |
| 22800 | Arthrodesis, posterior, for spinal deformity, with or without cast; ≤6 vertebral segments |
| 22802 | Arthrodesis, posterior, for spinal deformity, with or without cast; 7-12 vertebral segments |
| 22804 | Arthrodesis, posterior, for spinal deformity, with or without cast; ≥13 vertebral segments |
| 22808 | Arthrodesis, anterior, for spinal deformity, with or without cast; 2-3 vertebral segments |
| 22810 | Arthrodesis, anterior, for spinal deformity, with or without cast; 4-7 vertebral segments |
| 22812 | Arthrodesis, anterior, for spinal deformity, with or without cast; ≥8 vertebral segments |
| 22818 | Kyphectomy, circumferential exposure of spine and resection of vertebral segment(s) (including body and posterior elements); 1-2 segments |
| 22819 | Kyphectomy, circumferential exposure of spine and resection of vertebral segment(s) (including body and posterior elements); ≥3 segments |
| 22830 | Exploration of spinal fusion |
| 22840 | Posterior nonsegmental instrumentation (eg, Harrington rod technique, pedicle fixation across 1 interspace, atlantoaxial transarticular screw fixation, sublaminar wiring at C1, facet screw fixation) |
| 22850 | Removal of posterior nonsegmental instrumentation (eg, Harrington rod) |
| 22852 | Removal of posterior segmental instrumentation |
| 22855 | Removal of anterior segmental instrumentation |
| 22859 | Insertion of intervertebral biomechanical device to intervertebral disc space or vertebral body defect without interbody arthrodesis, each contiguous defect |
| 22867 | Insertion of interlaminar/interspinous process stabilization/distraction device, without fusion (including image guidance, when performed), with open decompression, lumbar; single level |
| 22868 | Insertion of interlaminar/interspinous process stabilization/distraction device, without fusion (including image guidance, when performed), with open decompression, lumbar; second level |
| 22869 | Insertion of interlaminar/interspinous process stabilization/distraction device, without open decompression or fusion (including image guidance, when performed), lumbar; single level |
| 22870 | Insertion of interlaminar/interspinous process stabilization/distraction device, without open decompression or fusion (including image guidance, when performed), lumbar; second level |
| 22899 | Unlisted procedure, spine |
| 63001 | Laminectomy, with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy, or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; cervical |
| 63003 | Laminectomy, with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy, or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; thoracic |
| 63005 | Laminectomy, with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy, or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis |
| 63011 | Laminectomy, with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy, or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; sacral |
| 63012 | Laminectomy, with removal of abnormal facets and/or pars interarticularis, with decompression of cauda equina and nerve roots for spondylolisthesis, lumbar (Gill-type procedure) |
| 63015 | Laminectomy, with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy, or discectomy (eg, spinal stenosis), >2 vertebral segments; cervical |
| 63016 | Laminectomy, with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy, or discectomy (eg, spinal stenosis), >2 vertebral segments; thoracic |
| 63017 | Laminectomy, with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy, or discectomy (eg, spinal stenosis), >2 vertebral segments; lumbar |
| 63020 | Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy, and/or excision of herniated intervertebral disc, including open and endoscopically assisted approaches; 1 interspace, cervical |
| 63030 | Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy, and/or excision of herniated intervertebral disc, including open and endoscopically assisted approaches; 1 interspace, lumbar |
| 63035 | Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy, and/or excision of herniated intervertebral disc, including open and endoscopically assisted approaches; each additional interspace, cervical or lumbar |
| 63040 | Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy, and/or excision of herniated intervertebral disc, re-exploration, single interspace; cervical |
| 63042 | Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy, and/or excision of herniated intervertebral disc, re-exploration, single interspace; lumbar |
| 63050 | Laminoplasty, cervical, with decompression of spinal cord, ≥2 vertebral segments |
| 63055 | Transpedicular approach, with decompression of spinal cord, cauda equina, and/or nerve root(s) (eg, herniated intervertebral disc), single segment; thoracic |
| 63056 | Transpedicular approach, with decompression of spinal cord, cauda equina, and/or nerve root(s) (eg, herniated intervertebral disc), single segment; lumbar (including transfacet or lateral extraforaminal approach) (eg, far lateral herniated intervertebral disc) |
| 63057 | Transpedicular approach, with decompression of spinal cord, cauda equina, and/or nerve root(s) (eg, herniated intervertebral disc), single segment; each additional segment, thoracic or lumbar |
| 63064 | Costovertebral approach, with decompression of spinal cord or nerve root(s) (eg, herniated intervertebral disc), thoracic; single segment |
| 63066 | Costovertebral approach, with decompression of spinal cord or nerve root(s) (eg, herniated intervertebral disc), thoracic; each additional segment |
| 63075 | Discectomy, anterior, with decompression of spinal cord and/or nerve root(s), including osteophytectomy; cervical, single interspace |
| 63076 | Discectomy, anterior, with decompression of spinal cord and/or nerve root(s), including osteophytectomy; cervical, each additional interspace |
| 63077 | Discectomy, anterior, with decompression of spinal cord and/or nerve root(s), including osteophytectomy; thoracic, single interspace |
| 63078 | Discectomy, anterior, with decompression of spinal cord and/or nerve root(s), including osteophytectomy; thoracic, each additional interspace |
| 63081 | Vertebral corpectomy (vertebral body resection), partial or complete, anterior approach, with decompression of spinal cord and/or nerve root(s); cervical, single segment |
| 63082 | Vertebral corpectomy (vertebral body resection), partial or complete, anterior approach, with decompression of spinal cord and/or nerve root(s); cervical, each additional segment |
| 63085 | Vertebral corpectomy (vertebral body resection), partial or complete, transthoracic approach, with decompression of spinal cord and/or nerve root(s); thoracic, single segment |
| 63086 | Vertebral corpectomy (vertebral body resection), partial or complete, transthoracic approach, with decompression of spinal cord and/or nerve root(s); thoracic, each additional segment |
| 63087 | Vertebral corpectomy (vertebral body resection), partial or complete, combined thoracolumbar approach, with decompression of spinal cord, cauda equina, or nerve root(s), lower thoracic or lumbar; single segment |
| 63088 | Vertebral corpectomy (vertebral body resection), partial or complete, combined thoracolumbar approach, with decompression of spinal cord, cauda equina, or nerve root(s), lower thoracic or lumbar; each additional segment |
| 63090 | Vertebral corpectomy (vertebral body resection), partial or complete, transperitoneal or retroperitoneal approach, with decompression of spinal cord, cauda equina, or nerve root(s), lower thoracic, lumbar, or sacral; single segment |
| 63091 | Vertebral corpectomy (vertebral body resection), partial or complete, transperitoneal or retroperitoneal approach, with decompression of spinal cord, cauda equina, or nerve root(s), lower thoracic, lumbar, or sacral; each additional segment |
| 63101 | Vertebral corpectomy (vertebral body resection), partial or complete, lateral extracavitary approach, with decompression of spinal cord and/or nerve root(s) (eg, for tumor or retropulsed bone fragment); thoracic, single segment |
| 63102 | Vertebral corpectomy (vertebral body resection), partial or complete, lateral extracavitary approach, with decompression of spinal cord and/or nerve root(s) (eg, for tumor or retropulsed bone fragment); lumbar, single segment |
| 63103 | Vertebral corpectomy (vertebral body resection), partial or complete, lateral extracavitary approach, with decompression of spinal cord and/or nerve root(s) (eg, for tumor or retropulsed bone fragment); thoracic or lumbar, each additional segment |
| 63170 | Laminectomy with myelotomy (eg, Bischof or DREZ type), cervical, thoracic, or thoracolumbar |
| 63172 | Laminectomy with drainage of intramedullary cyst/syrinx; to subarachnoid space |
| 63173 | Laminectomy with drainage of intramedullary cyst/syrinx; to peritoneal or pleural space |
| 63180 | Laminectomy and section of dentate ligaments, with or without dural graft, cervical; 1-2 segments |
| 63182 | Laminectomy and section of dentate ligaments, with or without dural graft, cervical; >2 segments |
| 63185 | Laminectomy with rhizotomy; 1-2 segments |
| 63190 | Laminectomy with rhizotomy; >2 segments |
| 63191 | Laminectomy with section of spinal accessory nerve |
| 63194 | Laminectomy with cordotomy, with section of 1 spinothalamic tract, 1 stage; cervical |
| 63200 | Laminectomy with release of tethered spinal cord, lumbar |
| 63250 | Laminectomy for excision or occlusion of arteriovenous malformation of spinal cord; cervical |
| 63251 | Laminectomy for excision or occlusion of arteriovenous malformation of spinal cord; thoracic |
| 63252 | Laminectomy for excision or occlusion of arteriovenous malformation of spinal cord; thoracolumbar |
| 63265 | Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; cervical |
| 63267 | Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; lumbar |
| 63268 | Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; sacral |
| 63270 | Laminectomy for excision of intraspinal lesion other than neoplasm, intradural; cervical |
| 63271 | Laminectomy for excision of intraspinal lesion other than neoplasm, intradural; thoracic |
| 63272 | Laminectomy for excision of intraspinal lesion other than neoplasm, intradural; lumbar |
| 63286 | Laminectomy for biopsy/excision of intraspinal neoplasm; intradural, intramedullary, thoracic |
| 63300 | Vertebral corpectomy (vertebral body resection), partial or complete, for excision of intraspinal lesion, single segment; extradural, cervical |
| 63308 | Vertebral corpectomy (vertebral body resection), partial or complete, for excision of intraspinal lesion, each additional segment |
| Physical therapy | |
| 92507 | Treatment of speech, language, voice, communication, and/or auditory processing disorder; individual |
| 97001 | Physical therapy evaluation |
| 97010 | Hot or cold pack application |
| 97012 | Mechanical traction |
| 97014 | Electrical stimulation (unattended) |
| 97016 | Vasopneumatic devices |
| 97022 | Whirlpool |
| 97026 | Infrared |
| 97032 | Electrical stimulation (manual) (15 minutes) |
| 97033 | Iontophoresis (15 minutes) |
| 97035 | Ultrasound (15 minutes) |
| 97039 | Unlisted modality (specify type and time if constant attendance) |
| 97110 | Therapeutic exercises to develop strength and endurance, range of motion, and flexibility (15 minutes) |
| 97112 | Neuromuscular re-education of movement, balance, coordination, kinesthetic sense, posture, and/or proprioception for sitting and/or standing activities (15 minutes) |
| 97113 | Aquatic therapy with therapeutic exercises (15 minutes) |
| 97116 | Gait training (including stair climbing) (15 minutes) |
| 97124 | Massage, including effleurage, petrissage, and/or tapotement (stroking, compression, percussion) (15 minutes) |
| 97140 | Manual therapy techniques (eg, connective tissue massage, joint mobilization and manipulation, and manual traction) (15 minutes) |
| 97150 | Group therapeutic procedure(s) (≥2 participants) |
| 97250 | Myofascial release (no longer a CPT code but billable under California workers’ compensation system in lieu of 97140) |
| 97530 | Dynamic activities to improve functional performance, direct (one-on-one) with patient (15 minutes) |
| 97535 | Self-care/home management training (eg, activities of daily living and compensatory training, meal preparation, safety procedures, and instructions in use of assistive technology devices/adaptive equipment), direct one-on-one contact (15 minutes) |
| 98960 | Education and training for patient self-management by a qualified, nonphysician health care professional using a standardized curriculum, face-to-face with individual patient (could include caregiver/family) (30 minutes) |
| Injection | |
| 20610 | Arthrocentesis, aspiration, and/or injection; major joint or bursa (hip) |
| 20611 | Arthrocentesis, aspiration, and/or injection; major joint or bursa (hip): ultrasound guided |
| 77002/77002-26 | Fluoroscopic guidance of needle |
a CPT, Current Procedural Terminology; CT, computed tomography; ICD-9, International Classification of Diseases, Ninth Revision.