
Abstract
Background:
The benefits of hip arthroscopic surgery in the setting of femoroacetabular impingement (FAI) have been well established; however, some patients may experience a greater degree of improvement than others. Identifying positive and negative predictors of outcomes would assist the orthopaedic surgeon’s management algorithm for patients with FAI.
Purpose/Hypothesis:
The objective of this systematic review was to identify demographic, radiographic, and other operative predictors of positive and negative outcomes after hip arthroscopic surgery for patients with FAI. It was hypothesized that factors including FAI morphology, age, body mass index (BMI), sex, dysplasia, articular cartilage damage, radiographic joint space, and labral treatment would predict outcomes after hip arthroscopic surgery.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
This systematic review was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Three databases (Embase, PubMed, and Ovid [MEDLINE]) were searched on May 19, 2018, using terms including “hip,” “arthroscopy,” and “FAI.” Studies were screened and data extracted in duplicate.
Results:
A total of 39 studies were included in this systematic review, comprising 9272 hips with a mean age of 36.5 years (47.2% female). Younger age, male sex, lower BMI (<24.5 kg/m2), Tönnis grade 0, and preoperative pain relief from diagnostic intra-articular hip injections predicted positive outcomes. Female sex, older age (>45 years), longer duration of preoperative symptoms (>8 months), elevated BMI, increased Tönnis grade (≥1), chondral defects, decreased joint space (≤2 mm), increased Kellgren-Lawrence grade (>3), increased lateral center-edge angle (LCEA), and undergoing labral debridement alone were predictors of negative outcomes.
Conclusion:
In patients with FAI, younger age, male sex, lower BMI (<24.5 kg/m2), Tönnis grade 0, and pain relief from preoperative intra-articular hip injections are significantly more likely to achieve positive outcomes after hip arthroscopic surgery. On the other hand, older age (>45 years), female sex, elevated BMI, osteoarthritic changes, decreased joint space (≤2 mm), chondral defects, increased LCEA, and undergoing labral debridement compared with labral repair are associated with negative outcomes.
Femoroacetabular impingement (FAI) is increasingly recognized as a cause for hip and groin pain in the young, active patient. 19 The bony morphologies of FAI, classified as pincer-, cam-, or combined-type deformities, are often accompanied by chondrolabral abnormalities. Hip arthroscopic surgery is indicated to treat FAI and related defects including labral lesions, ligamentum teres injuries, and articular cartilage delamination. 37 Compared with open approaches, hip arthroscopic surgery may result in faster recovery, lower complication rates, less pain, and less morbidity. 4 Over the past decade, hip arthroscopic surgery rates have risen exponentially. 30 Hip arthroscopic surgery has reduced pain and improved function in patients in most age groups, body mass indices (BMIs), sexes, income levels, and activity levels. 44,61
Negative outcomes after hip arthroscopic surgery for FAI may be defined as persistent pain, looseness, and stiffness with reduced range of motion, refractory to nonsurgical treatment or reoperation. 13 Furthermore, dissatisfaction can result from an inability to return to desired activities. Failure rates for hip arthroscopic surgery range from 2.9% to 13.2%. 11,12,26 Residual or unaddressed FAI is the most common cause of negative outcomes in hip arthroscopic surgery. 3 Other potential causes of negative outcomes include unrecognized acetabular dysplasia, soft tissue laxity, and osteoarthritis. Positive outcomes after hip arthroscopic surgery usually involve achieving the minimal clinically important difference (MCID) or substantial clinical benefit (SCB) on patient-reported outcome measures (PROMs). 47,48 Negative outcomes after hip arthroscopic surgery for FAI are typically managed with revision arthroscopic surgery or open surgical hip dislocation but sometimes require total hip arthroplasty (THA). 3
Now that the benefits of hip arthroscopic surgery have been well established in the literature, the next logical step is to identify predictors of positive and negative outcomes in the setting of FAI. The previous identification of these factors in arthroscopic surgery has been important; for example, labral debridement versus labral repair as a predictor for negative outcomes has changed surgical strategies and techniques over the past decade. 34,54 Identifying such predictors would undoubtedly alter the orthopaedic surgeon’s management algorithm for patients with FAI. The objective of this systematic review was to identify clinical, radiographic, and demographic predictors of positive and negative outcomes after hip arthroscopic surgery for patients with FAI. It was hypothesized that factors including FAI type, age, BMI, sex, dysplasia cartilage damage, radiographic joint space, and labral treatment would predict outcomes after hip arthroscopic surgery.
Methods
Search Strategy
The methodology of the following systematic review was adopted from a previous study. 29 This systematic review was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Three online databases (Embase, PubMed, and Ovid [MEDLINE]) were searched from database inception until May 19, 2018, for studies investigating the predictors of clinical outcomes after hip arthroscopic surgery for FAI. The broad and inclusive search included the terms “hip,” “arthroscopy,” and “FAI” (Appendix Table A1).
Study Screening
The titles, abstracts, and full-text articles were screened by 2 reviewers (J.K., M.M.) independently and in duplicate. Disagreements during title and abstract screening moved onto the next stage for a more in-depth review. Any disagreements were discussed between the reviewers, and a senior author (O.R.A.) was consulted for any remaining discrepancies. The references of the included studies were subsequently manually screened for additional articles that may have eluded the initial search strategy.
Assessment of Study Eligibility
The research question and study eligibility criteria were established a priori. The inclusion criteria were English-language studies, studies investigating humans, studies with level of evidence 1 to 4, studies with a minimum follow-up of 6 months, those published after January 1, 2010, and those reporting the predictors of outcomes after the arthroscopic management of FAI. Exclusion criteria were animal studies, commentaries, book chapters, review articles, and technical studies.
Data Abstraction
Data were collected by 2 reviewers (O.A.S., A.S.) and recorded in an Excel spreadsheet (version 2007; Microsoft). Abstracted data included the author names, year of publication, study design, sample size, sex ratio, mean age, types of procedures performed, definitions of positive and negative outcomes, and clinical, radiographic, or intraoperative predictors assessed.
Quality Assessment
The methodological quality of the included studies was assessed using the Methodological Index for Non-Randomized Studies (MINORS) instrument. This tool was designed to assess the methodological quality of comparative and noncomparative, nonrandomized surgical studies. 59 Using the MINORS checklist, noncomparative studies are assigned a maximum score of 16, and comparative studies can achieve a maximum score of 24. The methodological quality of noncomparative studies was categorized a priori as follows: 0-4 indicated very low quality evidence, 5-7 indicated low quality, 8-12 indicated fair quality, and ≥13 indicated high quality. Furthermore, for comparative studies, the methodological quality was categorized as follows: 0-6 indicated very low quality, 7-10 indicated low quality, 11-15 indicated fair quality, 16-20 indicated good quality, and ≥21 indicated high quality.
Statistical Analysis and Assessment of Agreement
To assess interreviewer agreement, the kappa (κ) statistic was calculated for the title, abstract, and full-text screening stages. Agreement was categorized a priori as follows: κ/intraclass correlation coefficient (ICC) of ≥0.60, substantial agreement; κ/ICC of 0.21-0.59, moderate agreement; and κ/ICC of ≤0.20, slight agreement. 33 Given the nonuniform nature of the studies included in this systematic review in terms of techniques and outcome reporting, the results are presented in narrative summary fashion. Definitions of positive and negative outcomes were derived from the identified studies in this review. Descriptive statistics including means, proportions, standard deviations and 95% confidence intervals were calculated using Minitab statistical software (version 17; Minitab).
Results
Search Strategy
The initial search of the online databases resulted in 3026 total studies. A systematic screening and assessment of eligibility identified 39 full-text articles that satisfied the inclusion and exclusion criteria (Figure 1). The reviewers reached substantial agreement at the title (κ = 0.829 [95% CI, 0.798-0.860]), abstract (κ = 0.853 [95% CI, 0.821-0.885]), and full-text (κ = 1.00) screening stages.

PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) flow diagram demonstrating a systematic review of the literature for clinical, radiographic, and other operative predictors of positive and negative outcomes of hip arthroscopic surgery in the management of femoroacetabular impingement (FAI).
Study Quality
The 39 included studies (Table 1) comprised 19 case series (level of evidence 4), 9 case-control studies (level 4), 3 prognostic studies (level 2), and 8 prospective cohort studies (level 2). The 28 noncomparative studies had a mean MINORS score of 13 of 16 (range, 9-15), which corresponds to high quality of evidence. Also, 52% of studies did not report a blinded assessment of outcomes, and 3 studies had a loss to follow-up of >5%. All noncomparative studies included a clearly stated aim, included all patients fit for inclusion, prospectively collected data according to a protocol, and selected endpoints appropriate to the study. The 11 comparative studies had a mean MINORS score of 16 of 24 (range, 12-20), indicating good quality of evidence. In 2 studies, the control group did not have baseline equivalence.
Study Characteristics and Demographics a
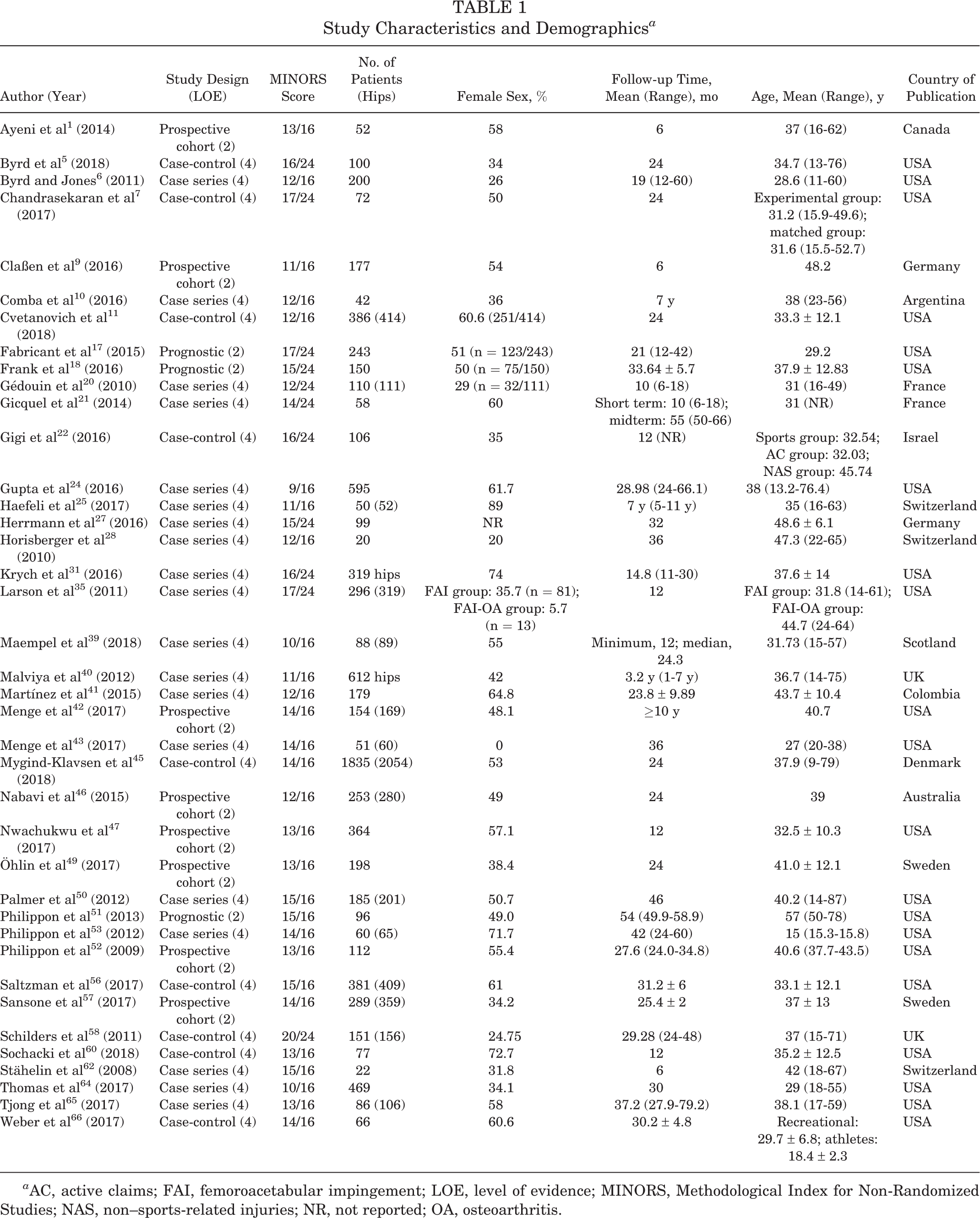
a AC, active claims; FAI, femoroacetabular impingement; LOE, level of evidence; MINORS, Methodological Index for Non-Randomized Studies; NAS, non–sports-related injuries; NR, not reported; OA, osteoarthritis.
Study Characteristics
Study investigators performed arthroscopic procedures in patients with FAI, including labral repair (82.9% of studies), labral debridement (75.6%), femoroplasty (75.0%), acetabuloplasty (51.0%), capsular plication (9.7%), microfracture (51.2%), removal of loose bodies (7.3%), and ligamentum teres debridement (14.6%). Twenty-seven studies provided a definition for negative outcomes. Outcomes after hip arthroscopic surgery were deemed negative if subsequent revision arthroscopic surgery, THA, or another operative procedure was required (50% of studies); hip pain and functional scores failed to meet the MCID or SCB (31%); patients could not return to work or sport (10%); there was a failure in the reduction of the alpha angle (3%); there was no postoperative functional improvement (3%); or if a patient’s death was reported (3%).
Sixteen studies provided a definition for positive outcomes. Of these 16 studies, 7 reported an improvement in postoperative scores meeting the MCID or SCB (Table 2). In the remaining studies, hip arthroscopic surgery outcomes were deemed positive if hip pain and functional scores improved and there was no conversion to THA or hip resurfacing procedure during the study period. Overall, hip arthroscopic surgery had positive outcomes in 1245 of 1723 hips (72.2%) in the population of studies that specified an MCID or SCB in their definitions of positive outcomes. Hip arthroscopic surgery had negative outcomes in 873 of 3968 hips (22.0%) in the population of studies that provided a definition of negative outcomes and reported these rates. The mean follow-up time for the 11 identified comparative studies was 22.4 months (range, 10-34 months). The remaining 28 noncomparative studies had a mean follow-up time of 40.8 months (range, 6-120 months). The key findings for each study reviewed are reported in Appendix Table A2.
Study Definitions and Details of Positive/Negative Outcomes, Operative Details, and Radiographic Details a

a AC, active claims; AIIS, anterior inferior iliac spine; EQ-5D, EuroQol–5 Dimensions; FAI, femoroacetabular impingement; HAGOS, Copenhagen Hip and Groin Outcome Score; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; iHOT, International Hip Outcome Tool; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; NAS, non–sports-related injuries; NR, not reported; NRS, numeric rating scale; OA, osteoarthritis; PASS, patient acceptable symptom state; PROM, patient-reported outcome measure; SCB, substantial clinical benefit; THA, total hip arthroplasty; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Clinical and Demographic Predictors of Positive Outcomes
Eleven studies examined clinical and demographic predictors of positive outcomes after hip arthroscopic surgery (Table 2). The most frequently reported demographic variables for positive outcomes were age, sex, and preoperative patient-reported outcomes. Three studies reported significant associations between undergoing surgery at a younger age and positive outcomes. Cvetanovich et al 11 found that younger age was associated with increased positive outcomes after arthroscopic surgery compared with older age (28.8 ± 11.1 vs 36.7 ± 11.7 years, respectively; P < .001). Two other studies used age in a regression model as continuous variables and found significant associations between younger age and positive outcomes; however, no binary cutoff was identified (Table 3). 24,47
Predictors of Positive Outcomes After Arthroscopic Surgery for FAI, Organized by Descending Level of Evidence a

a BMI, body mass index; FAI, femoroacetabular impingement; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; iHOT, International Hip Outcome Tool; LCEA, lateral center-edge angle; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; OR, odds ratio; PASS, patient acceptable symptom state; RR, rate ratio; SCB, substantial clinical benefit; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Studies reported a significant association between sex and positive outcomes after hip arthroscopic surgery (Table 3). Frank et al 18 found that male patients older than 45 years scored significantly higher than female patients older than 45 years on the Hip Outcome Score (HOS)–Sports-Specific Subscale (SSS) (P = .024) and modified Harris Hip Score (mHHS) (P = .042). Malviya et al 40 reported that male sex was a significant predictor for improvement after hip arthroscopic surgery (P < .001). Increases in preoperative patient-reported outcomes (>60 on the HOS–Activities of Daily Living [ADL]) were associated with patients having positive outcomes. Gupta et al 24 also identified increases in the preoperative Non-Arthritic Hip Score (NAHS) (rate ratio [RR], 0.980 [95% CI, 0.965-0.995]; P = .009) as associated with decreases in negative outcomes (Table 3), although a cutoff was not provided.
Cvetanovich et al 11 also investigated BMI and workers’ compensation status as predictors for patients after hip arthroscopic surgery. They found that a lower BMI (<24.5 kg/m2) was associated with successfully achieving the MCID on the HOS-SSS (odds ratio [OR], 0.92 [95% CI, 0.87-0.98]; P = .006). Patients who did not have workers’ compensation status were associated with achieving the MCID on the HOS-SSS (OR, 0.16 [95% CI, 0.03-0.75]; P = .02). Saltzman et al 56 also reported that patients with a normal BMI (18.5-24.9 kg/m2) had positive outcomes. Gigi et al 22 investigated and compared outcomes after arthroscopic surgery in patients with work-related active claims, sports injuries with no active claims, and non–sports-related injuries with no active claims pending. The sports injury group demonstrated a greater improvement on the mHHS, from a mean score of 67.01 (95% CI, 61.40-72.62) to 83.26 (95% CI, 78.22-88.29) (P < .001), than the active claims group, from a mean score of 59.62 (95% CI, 52.75-66.49) to 64.92 (95% CI, 52.65-72.19) (P < .042). This had a significant intergroup comparison of change in the mHHS (active claims vs sports injury; P = .019). Gupta et al 24 found that increased preoperative flexion was a significant predictor for decreased postoperative conversion to THA or a hip resurfacing procedure. They reported a mean preoperative flexion of 118.36° (range, 12°-160°) in their study population, with 9.1% of patients having negative outcomes (Table 3).
Clinical and Demographic Predictors of Negative Outcomes
Twenty-six studies examined clinical and demographic predictors for negative outcomes in hip arthroscopic surgery (Table 2). The most frequently reported demographic variables for negative outcomes in the included studies were age and sex. Older age was identified as a significant predictor for negative outcomes after hip arthroscopic surgery (Table 4). 9,10,18,24,42,45,52 Frank et al 18 similarly identified age and sex as predictors for negative outcomes. Female and male patients >45 years old scored significantly worse than younger female and male patients on postoperative PROMs (Table 4).
Predictors of Negative Outcomes After Arthroscopic Surgery for FAI, Organized by Descending Level of Evidence a
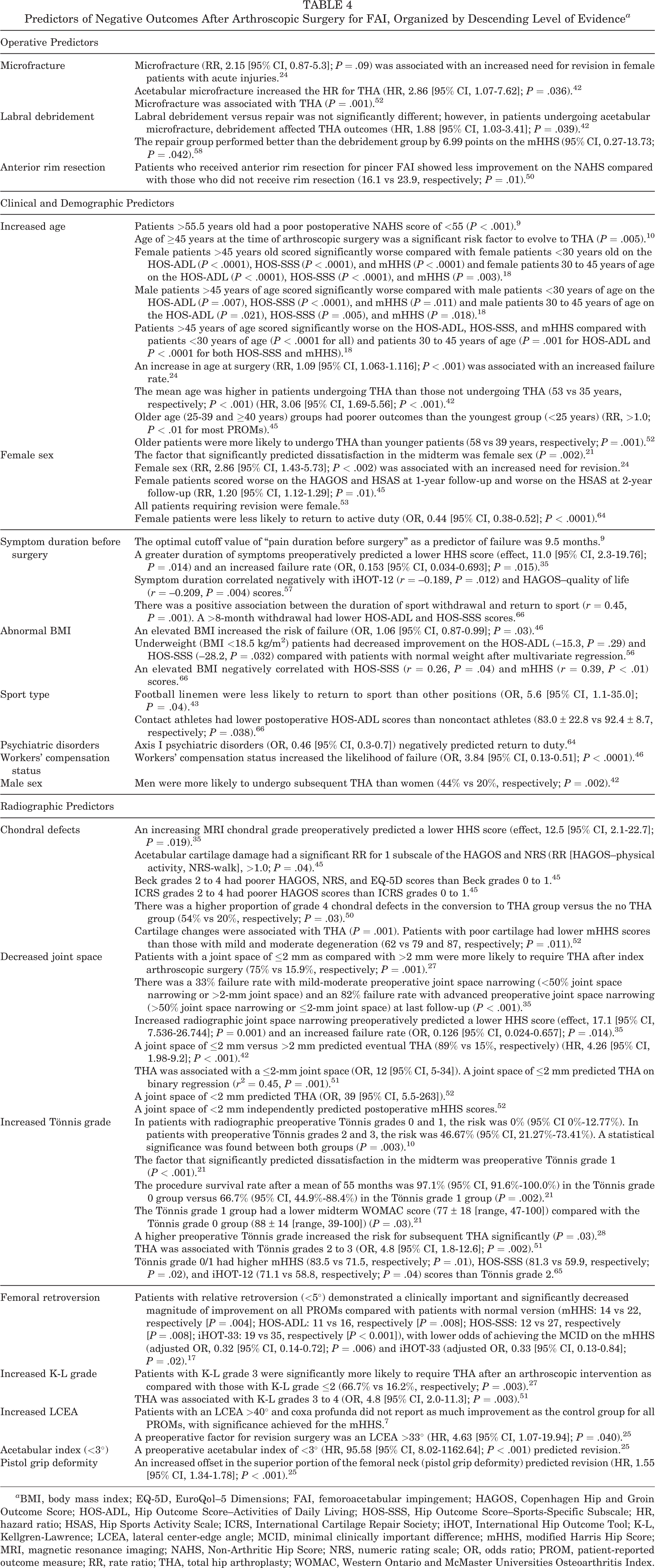
a BMI, body mass index; EQ-5D, EuroQol–5 Dimensions; FAI, femoroacetabular impingement; HAGOS, Copenhagen Hip and Groin Outcome Score; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; HR, hazard ratio; HSAS, Hip Sports Activity Scale; ICRS, International Cartilage Repair Society; iHOT, International Hip Outcome Tool; K-L, Kellgren-Lawrence; LCEA, lateral center-edge angle; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; MRI, magnetic resonance imaging; NAHS, Non-Arthritic Hip Score; NRS, numeric rating scale; OR, odds ratio; PROM, patient-reported outcome measure; RR, rate ratio; THA, total hip arthroplasty; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Menge et al 42 observed that men were more likely to undergo subsequent THA than women (44% vs 20%, respectively; P = .002). Mygind-Klavsen et al 45 reported that female patients scored worse on the postoperative Copenhagen Hip and Groin Outcome Score (HAGOS) and Hip Sports Activity Scale (HSAS) at 1-year follow-up and worse on the HSAS at 2-year follow-up (RR, 1.20 [95% CI, 1.12-1.29]; P = .01). Philippon et al 53 evaluated revision arthroscopic surgery as a negative outcome. All patients who required revision in their study were female. Overall, they observed that male patients had higher mHHS scores postoperatively than female patients (96 vs 88, respectively; P = .018). Thomas et al 64 assessed hip arthroscopic surgery for FAI in a military population. They observed that female patients (OR, 0.44 [95% CI, 0.38-0.52]; P < .0001) and patients with Axis I psychiatric disorders (OR, 0.46 [95% CI, 0.3-0.7]) were less likely to return to active duty. Finally, Gupta et al 24 reported that female sex was associated with an increased need for revision after hip arthroscopic surgery (RR, 2.86 [95% CI, 1.43-5.73]; P < .002). Overall, studies consistently identified the older female patient (>45 years) as the demographic at an increased risk for negative outcomes after hip arthroscopic surgery for FAI.
Four identified studies concurred that a longer duration of symptoms preoperatively (ranging from 8 months to 4 years) was a predictor for negative outcomes after hip arthroscopic surgery. 9,35,57,66 Menge et al 43 found that football linemen were less likely to return to sport compared with other position players (OR, 5.6 [95% CI, 1.1-35.0]; P = .04). Two studies reported that an elevated BMI increased the risk of negative outcomes. 46,66 More specifically, Nabavi et al 46 reported a mean BMI of 29 kg/m2 in their identified poor outcomes group. In addition, Weber et al 66 reported that contact athletes had a lower postoperative HOS-ADL score than noncontact athletes (83.0 ± 22.8 vs 92.4 ± 8.7, respectively; P = .038). Saltzman et al 56 found that underweight patients (BMI <18.5 kg/m2) had decreased improvement compared with patients with a normal BMI. Nabavi et al 46 also assessed workers’ compensation status and reported that it increased the likelihood of negative outcomes (OR, 3.84 [95% CI, 0.13-0.51]; P < .0001). Finally, Thomas et al 64 reported that patients with Axis I psychiatric disorders were associated with negative outcomes. These findings are summarized in Table 4.
Radiographic Predictors of Positive Outcomes
Eight studies examined radiographic predictors of positive outcomes after hip arthroscopic surgery (see Table 2). Four studies reported Tönnis grade 0 as a significant predictor for positive outcomes. 11,20,21,65 Cvetanovich et al 11 found that patients who were preoperatively determined to be Tönnis grade 0 achieved the MCID for the HOS-ADL (OR, 2.49 [95% CI, 1.13-5.44]; P = .022) and the patient acceptable symptom state (PASS) for the HOS-SSS (OR, 2.72 [95% CI, 1.22-6.33]; P = .014) relative to patients with Tönnis grade 1. In patients not requiring revision arthroplasty in the study by Gicquel et al, 21 the only factors associated significantly with the midterm Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score were preoperative Tönnis grade (P = .047) and midterm Tönnis grade (P = .03).
Gupta et al 24 investigated the center-edge angle as a predictor for positive outcomes and found that increases in the sagittal center-edge angle (SCEA) and lateral center-edge angle (LCEA) were associated with decreased negative outcomes. These authors reported a mean SCEA and LCEA of 58.0° ± 9.7° and 29.18° (range, 11°-49°), respectively. Cutoff angles were not reported. Nwachukwu et al 47 reported that lower Outerbridge grade (96.7% grade 0) (OR, 0.44 [95% CI, 0.15-0.94]) and lower acetabular version (OR, –0.95 [95% CI, 0.92-0.98]) were predictive of reaching positive outcomes after arthroscopic surgery.
An increased joint space was identified as a significant predictor for positive outcomes in 2 studies (Table 3). 11,24 Gupta et al 24 reported a mean central joint space of 3.46 mm (range, 1.3-6.7 mm), and Cvetanovich et al 11 reported a mean medial joint space of 4.1 ± 0.8 mm. No specific cutoffs for positive outcomes were reported. Overall, preoperatively determined Tönnis grade 0 with decreased chondral defects and an increased center-edge angle were associated with improved outcomes after arthroscopic surgery for FAI.
Radiographic Predictors of Negative Outcomes
Eighteen studies examined radiographic predictors of negative outcomes after hip arthroscopic surgery (see Table 2). The preoperatively determined Tönnis grade was reported in 8 studies. Numerous studies reported that a higher preoperatively determined Tönnis grade (≥1) led to more negative outcomes after hip arthroscopic surgery (Table 4). 10,21,28,51,65 The LCEA was also predictive of negative outcomes after hip arthroscopic surgery in 2 studies (Table 4). 7,25 More specifically, Chandrasekaran et al 7 reported a mean LCEA of 45.0° in their study and noted that although arthroscopic interventions significantly improved patient outcomes, patients with an LCEA >40° and coxa profunda did not report as much improvement in comparison with their matched control group with a mean LCEA of 31.3°. Additionally, Haefeli et al 25 reported an LCEA >33° (hazard ratio [HR], 4.63 [95% CI, 1.07-19.94]; P = .040) as a preoperative factor for revision surgery. They also found that a decreased acetabular index <3° (HR, 95.58 [95% CI, 8.02-1162.64]; P < .001) and increased offset in the superior portion of the femoral neck (pistol grip deformity) (HR, 1.55 [95% CI, 1.34-1.78]; P < .001) predicted negative outcomes.
Two studies investigated the Kellgren-Lawrence (K-L) grade and reported that a higher K-L grade (≥3) was significantly associated with negative outcomes after hip arthroscopic surgery (Table 4). 27,51 Furthermore, a lower preoperatively determined joint space (≤2 mm) was associated with negative outcomes after arthroscopic surgery (Table 4). 27,35,42,51,52 Fabricant et al 17 found that femoral retroversion (<5°) predicted negative outcomes. Finally, increased chondral defects were associated with negative outcomes (Table 4). 35,45,50,52 The constellation of degenerative changes and decreased joint space (≤2 mm) strongly predicted negative outcomes after arthroscopic surgery for FAI.
Other Operative Predictors of Positive Outcomes
Preoperative bupivacaine intra-articular hip injections tended to predict patients’ having positive outcomes after arthroscopic surgery for FAI (see Table 3). 1,31 Thomas et al 64 found that hip arthroscopic surgery performed by surgeons with sports fellowship training had a higher rate of return to active duty than patients treated by arthroplasty fellows (47% vs 32%, respectively; P < .0001).
Other Operative Predictors of Negative Outcomes
Acetabular microfracture was predictive of the progression to revision or THA in 3 studies. 24,42,52 Labral debridement was associated with poorer postoperative patient-reported outcomes. Schilders et al 58 investigated labral debridement versus labral repair and found that the repair group performed better by 6.99 points on the mHHS (range, 0.27-13.73; P = .042). Menge et al 42 found no difference between debridement and repair; however, in patients undergoing acetabular microfracture, debridement affected the THA outcome (HR, 1.88 [95% CI, 1.03-3.41]; P = .039). Six studies investigated labral repair as an operative predictor of negative outcomes. 42,47,50,52,53,58 None of them reported significant results. Palmer et al 50 performed arthroscopic surgery on a cohort of patients with cam FAI. Combined decompression was performed on 49 of 201 hips in their study. They reported that anterior rim resection for pincer FAI showed less improvement on the NAHS compared with patients who did not receive rim resection (16.1 vs 23.9, respectively; P = .01). Five of 13 conversions to THA originated from this subgroup.
Discussion
Clinical and demographic predictors of positive outcomes after hip arthroscopic surgery for FAI included younger age, male sex, and lower BMI (<24.5 kg/m2), and clinical and demographic predictors of negative outcomes included older age (>45 years), female sex, longer duration of preoperative pain symptoms (>8 months), and elevated BMI. Radiographic predictors of positive outcomes included Tönnis grade 0 and increased joint space. Higher Tönnis grade (≥1), LCEA >33°, chondral defects, higher K-L grade (≥3), and decreased joint space (≤2 mm) were common radiographic predictors of negative outcomes. Other identified operative predictors of positive outcomes were pain relief from preoperative intra-articular hip injections. Other operative predictors of negative outcomes were labral debridement compared with labral repair. Finally, the studies that reported an MCID or SCB in their definitions for positive outcomes found that relief from preoperative intra-articular hip injections, lower BMI (<24.5 kg/m2), younger age, Tönnis grade 0, and increased joint space predicted positive outcomes.
The predictors of positive and negative outcomes identified in our review are supported by existing literature on outcomes after hip arthroscopic surgery. Both male and female sex has been associated with positive outcomes after hip arthroscopic surgery. 12,44,55 However, female sex as an identifiable factor appears to be clearer as a negative predictor. Although there is no clear consensus, the role of soft tissue laxity in female patients, possibly leading to negative outcomes, could be postulated. This is a potential area for further investigation in future studies. Surgeons performing arthroscopic surgery in patients with FAI who are older than 45 years should proceed with caution, as this demographic was more likely to have negative outcomes regardless of sex. 15,43 Furthermore, in the setting of FAI, female and overweight patients (BMI >24.5 kg/m2) with a prolonged duration of preoperative pain may be prone to negative outcomes after arthroscopic surgery. Specifically, athletes with a longer preoperative withdrawal time (>8 months) from sports, and also football linemen in general, could be more prone to negative outcomes. 46,66
Osteoarthritic changes and pre-existing cartilage damage have been thought to be factors associated with negative outcomes after hip arthroscopic surgery. 8,12,28,44 The current study similarly identified osteoarthritic changes, as seen on preoperative imaging, as significant predictors of negative outcomes. Specifically, a decreased joint space (≤2 mm); the presence of cysts, osteophytes, and sclerosis as evidenced by an increased Tönnis grade (≥1); and K-L grade (≥3) predicted negative outcomes. As such, surgeons should counsel their patients on the potential negative impact that pre-existing degenerative changes can have on outcomes after arthroscopic surgery for FAI. Although no specific cutoff was identified, the overall mean follow-up time for the studies that identified degenerative changes was 48 months. Therefore, caution is warranted, as it is likely that the survivorship of the hip decreases in this cohort of patients.
Typically, acetabuli with an LCEA >39° to 40° and concomitant protrusion are classified as pincer-type FAI. 14,36,63 A higher preoperative LCEA was identified as a protective factor against eventual THA in 1 study. However, overall, it appears that practitioners can expect a decreased postoperative improvement in patients with an increased preoperative LCEA and decreased acetabular index (extrusion), both indicators of pincer-type FAI. Combined acetabular overcoverage with protrusion will not exhibit the same degree of improvement compared with hips without protrusion. 7 These findings may be related to procedural technical difficulties or differing patterns of labral damage. 8 Acetabular microfracture for chondral defects in the setting of FAI has generally led to positive outcomes. 38 We identified 3 studies that reported it as a risk factor for eventual conversion to THA, a finding that has been previously documented. 23 Similar to reports on the knee, it has been theorized that this technique exposes the subchondral bone, and if formation fails, fragility and subchondral bone cysts can develop, accelerating degenerative changes. 2 In the microfracture studies that we identified, patients were older (mean age, 58 years) and had a decreased joint space (≤2 mm) with chondral defects (Outerbridge grade 4). These cofactors must be considered when interpreting these results of microfracture after hip arthroscopic surgery, as previous literature has reported their association with negative outcomes. 16 Therefore, it is possible that microfracture should be avoided in the setting of the older patient with degenerative changes. Finally, studies have documented superior outcomes with labral repair compared with labral debridement, which supports our findings. 32,34
This review was primarily limited by the quality of reporting, varying levels of evidence, heterogeneity of variables assessed, and use of multiple PROMs across the included studies. Specifically, there was significant heterogeneity in the definition of “negative outcomes” after hip arthroscopic surgery. Definitions included conversion to THA/revision arthroscopic surgery, failure to achieve the SCB/MCID, failure to return to sport, and failure to achieve improvement on PROMs/radiographic findings. This heterogeneity in the definition of “negative outcomes” limits the generalizability of the findings of this systematic review and precluded the ability to perform a meta-analysis. Additionally, there were few reported MCIDs or SCBs for the PROMs used in the various definitions of “positive outcomes.” This can limit the external validity of the positive predictors that did not include these measures. However, the studies in this review had high and good quality of evidence, indicating that the predictors identified in this review likely contribute to outcomes in some form. A secondary limitation is that not all studies reported a mean LCEA or alpha angle in their patient populations. As established in the literature, these radiographic parameters can confound postoperative results. Finally, we were unable to identify a clear cutoff for younger age as a predictor for negative outcomes. Future investigations should be undertaken to provide clarity for this predictor.
This systematic review successfully identified clinical, radiographic, and other operative predictors of positive and negative outcomes after hip arthroscopic surgery in the setting of FAI. Hip arthroscopic surgery for FAI necessitates a comprehensive selection of suitable patients to maximize favorable postoperative outcomes. Future studies, including a prospective evaluation of a large sample size of patients with an accepted and uniform definition of positive and negative outcomes, are warranted. The information from these studies could provide clinical guidelines for orthopaedic surgeons to use when assessing patients with FAI for hip arthroscopic surgery.
Conclusion
In patients with FAI, younger age, male sex, lower BMI (<24.5 kg/m2), Tönnis grade 0, increased joint space and pain relief from preoperative intra-articular hip injections were significantly more likely to achieve positive outcomes after hip arthroscopic surgery. More specifically, pain relief from preoperative intra-articular hip injections, lower BMI (<24.5 kg/m2), younger age, Tönnis grade 0, and increased joint space were positive predictors defined by an MCID or SCB. On the other hand, older age (>45 years), female sex, longer duration of preoperative pain symptoms (>8 months) elevated BMI, osteoarthritic changes, decreased joint space (≤2 mm), chondral defects, increased LCEA, and undergoing of labral debridement versus labral repair were associated with negative outcomes.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: E.L.B. has received speaking fees from Pendopharm, Stryker, Smith & Nephew, ConMed, and Victhom and is an advisory board member for Bodycad. O.R.A. is an educational consultant for the speakers’ bureau of ConMed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
APPENDIX
Study Key Findings a

| Author (Year) | Primary Outcomes After Arthroscopic Surgery | Key Finding |
|---|---|---|
| Ayeni et al 1 (2014) | mHHS | A negative response from an intra-articular hip injection may predict a higher likelihood of having a negative result from surgery. |
| Byrd et al 5 (2018) | mHHS | There was an improvement on the mHHS after arthroscopic surgery regardless of the Tönnis grade. |
| Byrd and Jones 6 (2011) | mHHS | No predictors were investigated. |
| Chandrasekaran et al 7 (2017) | mHHS | Patients with overcoverage had improvement but did not do as well after arthroscopic surgery compared with matched controls. |
| Claßen et al 9 (2016) | NAHS, WOMAC | The date of surgery is an important predictor in avoiding the occurrence of chondral defects in patients with symptomatic cam-type FAI. |
| Comba et al 10 (2016) | WOMAC, mHHS | Patients with advanced osteoarthrosis and patients >45 years old had a higher risk of requiring THA. |
| Cvetanovich et al 11 (2018) | HOS-ADL, HOS-SSS | Younger age, a lower BMI, no workers’ compensation status, and a normal joint space correlated with higher postoperative PROM scores. |
| Fabricant et al 17 (2015) | HOS-ADL, HOS-SSS, iHOT-33, mHHS | Patients with relative retroversion (<5° of anteversion) had smaller, but clinically important, improvements on all PROMs compared with those with normal or increased version when controlling for relevant covariates in multiple regression analysis. Relative femoral retroversion should not be considered an absolute contraindication to surgical correction of FAI. |
| Frank et al 18 (2016) | HOS-ADL, HOS-SSS, mHHS | Age and sex were found to be significant independent predictors of PROM scores, with older age being the most influential predictor of worse scores. |
| Gédouin et al 20 (2010) | WOMAC, satisfaction | The presence of established osteoarthritis emerged as an important negative prognostic factor for functional results. |
| Gicquel et al 21 (2014) | WOMAC, satisfaction | Tönnis grade 1 hips should be managed with caution. In this population, arthroscopic treatment should be reserved for those patients at the severe end of the symptom spectrum, who should be informed of the increased risk of negative outcomes, particularly in the presence of incipient joint space narrowing. |
| Gigi et al 22 (2016) | mHHS, HOS | There was decreased improvement in postoperative outcomes in the active claims group compared with other groups. |
| Gupta et al 24 (2016) | NAHS, mHHS | Increased preoperative PROM scores, preoperative flexion, and central joint space were associated with decreased revision rates. Female sex, increased age, and microfracture were associated with an increased need for revision. |
| Haefeli et al 25 (2017) | Revision rate as a negative outcome | An LCEA >33° and pistol grip deformity were significant preoperative factors for revision surgery. |
| Herrmann et al 27 (2016) | Prognostic factors for early conversion to THA | An increased K-L grade and decreased joint space were significantly more likely to require THA. |
| Horisberger et al 28 (2010) | Conversion to THA, NAHS, VAS | A higher Tönnis grade significantly increased the risk for subsequent THA. |
| Krych et al 31 (2016) | HOS | Intra-articular anesthetic injections were weak predictors of outcomes after hip arthroscopic surgery. Patients with >50% relief had similar outcomes to those who showed no relief. |
| Larson et al 35 (2011) | Conversion to THA, <70 on mHHS | Identified negative predictors were a greater duration of symptoms preoperatively and increasing MRI chondral grade. |
| Maempel et al 39 (2018) | No definition; assessment of age, sex, and socioeconomic status on PROMs | There were no significant predictor findings. |
| Malviya et al 40 (2012) | NR | Preoperative quality of life and male sex predicted positive outcomes. |
| Martínez et al 41 (2015) | Revision arthroscopic surgery, open hip surgery | There was an association between higher preoperative WOMAC scores and negative outcomes after arthroscopic surgery. Osteochondroplasty was the only surgical procedure associated with positive outcomes. |
| Menge et al 42 (2017) | HOS-ADL, HOS-SSS, mHHS, SF-12 PCS | There was a high rate of conversion to THA in patients with a preoperative joint space of ≤2 mm. |
| Menge et al 43 (2017) | Return to sport | Linemen were less likely to return to sport. Microfracture was not associated. |
| Mygind-Klavsen et al 45 (2018) | HAGOS, HSAS, NRS, EQ-5D | Age >25 years and higher grade cartilage injuries (femoral head and acetabulum) negatively affected outcomes. |
| Nabavi et al 46 (2015) | mHHS, NAHS | An elevated BMI and workers’ compensation status predicted poor outcomes. |
| Nwachukwu et al 47 (2017) | HOS-ADL, HOS-SSS, iHOT-33, mHHS | Advanced age and Outerbridge grade negatively prognosticated the SCB. Preoperative HOS thresholds predicted the SCB. |
| Öhlin et al 49 (2017) | iHOT-12 | Preoperative iHOT-12 scores correlated with postoperative iHOT-12 scores (1 point higher = 0.65 points higher at 2-year follow-up). |
| Palmer et al 50 (2012) | NAHS, VAS, satisfaction | There was no difference in age. Cam hips had poorer outcomes compared with the rest of the study group. |
| Philippon et al 51 (2013) | K-L grade, Tönnis grade | A joint space of ≤2 mm best predicted negative outcomes in patients ≥50 years old. |
| Philippon et al 53 (2012) | HOS-SSS, mHHS | There was no difference between patients undergoing labral debridement and those undergoing labral repair. Female patients had worse outcomes. |
| Philippon et al 52 (2009) | mHHS, HOS-ADL, HOS-SSS, NAHS | A preoperative joint space of ≥2 mm and labral repair were associated with good outcomes. |
| Saltzman et al 56 (2017) | HOS-ADL, HOS-SSS, VAS, mHHS | No associations were observed between BMI and clinical outcomes after multivariate analysis. |
| Sansone et al 57 (2017) | iHOT-12, HAGOS, HSAS, VAS, EQ-5D | A long symptom duration was correlated with inferior outcomes. There was no correlation between age, cartilage status, and outcomes. |
| Schilders et al 58 (2011) | mHHS | Labral repair was favored over resection. |
| Sochacki et al 60 (2018) | BDI-II, HOS, iHOT-33 | Preoperative moderate and severe depression predicted poorer outcomes compared with mild/moderate depression. |
| Stähelin et al 62 (2008) | Range of motion, VAS, NAHS | Offset correction was not correlated with clinical outcomes. |
| Thomas et al 64 (2017) | VAS, SANE, return to duty | Return to duty was negatively affected by female sex, Axis I psychiatric disorders, a low rank, and pelvic pain. Special forces and infantry experienced better outcomes. |
| Tjong et al 65 (2017) | mHHS, iHOT-12, HOS-SSS | Patients with degenerative changes (Tönnis grade 2) demonstrated lower scores. There was no correlation between the alpha angle and PROM scores. |
| Weber et al 66 (2017) | mHHS, HOS-SSS, HOS-ADL | A longer preoperative withdrawal from sport predicted a longer time for return to sport. A higher BMI predicted poorer outcomes. |
a BDI-II, Beck Depression Inventory–II; BMI, body mass index; EQ-5D, EuroQol–5 Dimensions; FAI, femoroacetabular impingement; HAGOS, Copenhagen Hip and Groin Outcome Score; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; HSAS, Hip Sports Activity Scale; iHOT, International Hip Outcome Tool; K-L, Kellgren-Lawrence; LCEA, lateral center-edge angle; mHHS, modified Harris Hip Score; MRI, magnetic resonance imaging; NAHS, Non-Arthritic Hip Score; NR, not reported; NRS, numeric rating scale; PROM, patient-reported outcome measure; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; SF-12 PCS, 12-Item Short Form Health Survey physical component summary; THA, total hip arthroplasty; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.