
Abstract
Background:
Osteoarthritis that develops after traumatic anterior shoulder instability is known as dislocation arthropathy, but its frequency and characteristics are still unclear.
Purpose:
To evaluate glenoid osteophytes in shoulders with traumatic anterior instability by using computed tomography (CT) and to elucidate the influence of instability on the progression of dislocation arthropathy in different age groups.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This study involved 214 unoperated patients with unilateral instability who underwent CT of both shoulders. The patients were divided into 2 groups according to age at the time of CT: ≤30 years (younger group; n = 172) and ≥31 years (older group; n = 42). Patient demographics as well as the presence, size, and location of glenoid osteophytes were compared between the 2 groups and also between patients with and without osteophytes. Furthermore, patients with osteophytes in the older group were divided into 2 subgroups according to age at the time of the initial injury: as a teenager (early-onset subgroup; n = 9) or at ≥31 years (late-onset subgroup; n = 14), and the same assessments were conducted.
Results:
Osteophytes were significantly more frequent on the affected side of the older group compared with the younger group (71.4% vs 13.9%, respectively; P < .001). In the younger group, patients with osteophytes had more multiple-instability events (P = .002) and a longer interval from injury to CT (P < .001) than those without osteophytes. Although there was no difference in osteophyte size between the 2 groups, most osteophytes were located at the anteroinferior part of the glenoid in the younger group, while osteophytes were usually circumferential around the glenoid in the older group. A comparison between the early- and late-onset subgroups in older patients with osteophytes revealed that the osteophytes were more frequently located at the anteroinferior glenoid region in the early-onset subgroup.
Conclusion:
CT allowed a detailed evaluation of glenoid osteophytes, revealing that osteophytes were not uncommon in younger patients. Instability itself might influence the progression of osteoarthritic changes in younger patients, while aging seems to have a greater effect in older patients.
Keywords
Computed tomography (CT) has become an essential imaging tool for the management of traumatic anterior shoulder instability. The size of the glenoid bone defect and the presence of a Hill-Sachs lesion or bony Bankart lesion are factors that influence the outcome of surgical treatment, and they must be assessed carefully by CT before performing surgery. 3 –5,10 When CT is used for the evaluation of these features in shoulders with traumatic anterior instability, we sometimes detect osteoarthritic (OA) changes of the glenohumeral joint. OA is often found in patients with recurrent anterior shoulder instability or older patients, and we have also noticed OA changes in some younger patients with anterior shoulder instability. OA that develops after a shoulder dislocation is known as dislocation arthropathy, 16 and it has usually been evaluated by the Samilson-Prieto radiographic classification, 16 although CT has since become a popular imaging method. There have been many reports about the radiographic features of dislocation arthropathy before and after shoulder stabilization surgery, 1,2,6,8,9,11,14,19,20 but only a few studies have assessed preoperative OA by CT in patients with traumatic anterior shoulder instability. 12,13 CT allows for a more detailed evaluation compared with plain radiography and can be employed to assess the characteristics of OA, such as minute osteophytes that cannot be detected on plain radiographs.
In this study, we focused on glenoid osteophytes as a feature of OA in unoperated shoulders with traumatic anterior instability. Because the influence of aging should be taken into account when assessing OA, we divided the patients into different age groups. However, our hypothesis was that osteophytes would be more frequent in the affected shoulder than the unaffected shoulder regardless of the patient’s age, because instability itself influences the development of OA. We also hypothesized that OA changes of the glenoid secondary to anterior instability would occur preferentially around the anterior part of the glenoid rim. Therefore, this study was designed to use CT for the evaluation of the frequency and characteristics of glenoid osteophytes in unoperated shoulders with traumatic anterior instability stratified by age.
Methods
Patients
Patients who presented to our institution with the chief complaint of traumatic anterior shoulder instability and had unilateral anterior instability on physical examination were eligible for this study. The exclusion criteria were as follows: bilateral shoulder instability, posterior or multidirectional instability, other associated shoulder injuries such as a rotator cuff tear or greater tuberosity fracture, atraumatic injuries, and any previous shoulder surgery. We investigated a total of 214 patients who underwent bilateral shoulder CT before treatment. The majority of these patients underwent surgical intervention after the CT examination. This study was approved by our institutional review board, and informed consent to participate was obtained from all of the patients.
Demographic Data
Patient demographic data included age at the time of CT, time from the initial injury to CT, total number of dislocations/subluxations, and presence/absence of glenoid bone defects. Patients were classified into 4 categories based on the total number of dislocations/subluxations (instability events): 1 event, 2-5 events, 6-9 events, and ≥10 events. While patients demonstrated various patterns of a traumatic injury, most of the patients were athletes, and they were initially injured during high-energy sporting activities. The size of the glenoid bone defect was measured on the face of the glenoid fossa by 3-dimensional CT and was calculated as a percentage of the defect width to the maximum glenoid diameter obtained by assuming that the glenoid fossa was circular. 17 In the present study, the assessment was based on age at CT; the breakdown of patients by age was as follows: 123 patients aged ≤20 years, 49 patients aged 21-30 years, 16 patients aged 31-40 years, 13 patients aged 41-50 years, and 13 patients aged ≥51 years.
Computed Tomography Protocol
CT was performed with an Aquilion scanner (Canon Medical Systems Corporation). Coronal and axial CT images were obtained perpendicular to the glenoid surface, while oblique sagittal images were obtained parallel to the glenoid surface at a slice thickness of 0.5 mm. The CT data were used for 3-dimensional reconstruction of a glenoid model so that the bone morphology of the glenoid face could be evaluated. 17 All patients underwent CT of the affected and unaffected shoulders by the same protocol. Bilateral shoulder CT only exposed patients to the same radiation dose as unilateral shoulder CT because our protocol allowed imaging of both shoulders simultaneously, which means that there was no adverse influence of excess radiation on the patients. All of the imaging evaluations were conducted by the first author (T.H.).
Definition and Measurement of Osteophytes
In this study, osteophytes were defined as bony protrusions from the rim of the glenoid fossa. 18 The size of each osteophyte was measured as the maximum distance between the glenoid rim and the osteophyte tip in any CT plane (Figure 1A). If there was glenoid bone loss, the glenoid defect was also included in the evaluation, and bony protrusions from the border of the defect were defined as osteophytes.
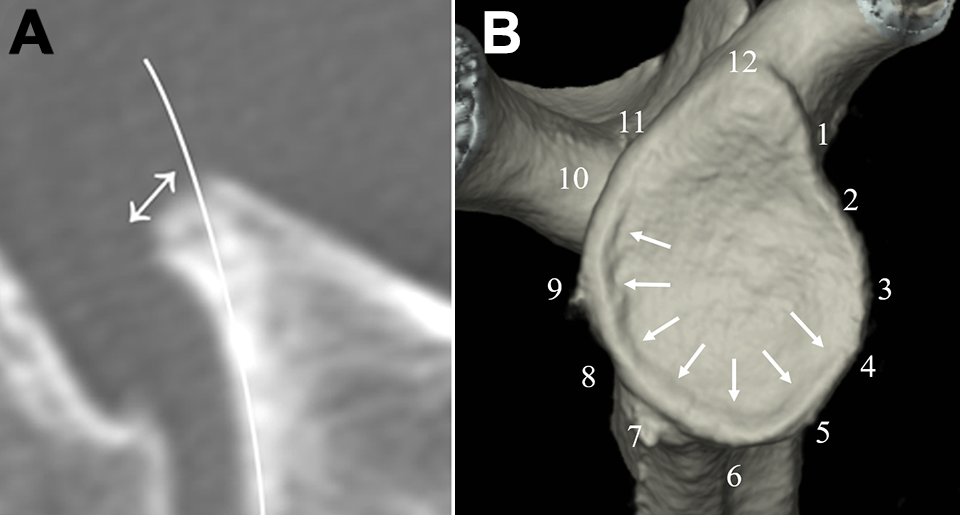
Measurement of the size and localization of glenoid osteophytes. (A) The size of the glenoid osteophyte was defined as the maximum distance between the glenoid rim and the osteophyte tip (arrow). (B) An example of consecutive osteophytes extending around the glenoid rim from 4 o’clock to 10 o’clock (arrows).
Localization of Osteophytes
In all shoulders, the location of each osteophyte was described using its clockface position (Figure 1B), and the number of shoulders with osteophytes at each position from 12 o’clock to 11 o’clock was calculated. When describing the clockface position of each osteophyte, the clockface for the left shoulder was adjusted to correspond to the right shoulder.
Comparative Evaluations
The frequency of osteophytes was compared among the different patient age groups. Next, we divided patients into a younger group (age ≤30 years) and an older group (age ≥31 years), and the demographic data of patients with and without osteophytes on the affected side were compared. Patients with osteophytes on the affected side were then assigned to a younger OA group (age ≤30 years) and an older OA group (age ≥31 years), and demographic data were compared between these groups to identify the factors related to osteophyte formation. Differences in osteophyte characteristics, including size and location, were also assessed. Finally, the older OA group was divided into 2 subgroups according to age at the time of the initial injury: as a teenager (early-onset subgroup) or at ≥31 years (late-onset subgroup), and these 2 groups were compared in the same way. All evaluations, including analysis of CT scans, were conducted by the first author, who was blinded to patient information, including the intraoperative findings of those who underwent surgical treatment.
Statistical Analysis
The normality of data was assessed using the Shapiro-Wilk test. Based on the result of this test and the sample size, different statistical methods were selected for comparative analysis. In brief, differences in the frequency of glenoid osteophytes were assessed by the chi-square test and Fisher exact test; differences in osteophyte size and the time from initial injury to CT were determined by the Student t test; and differences in osteophyte location, instability events, and glenoid bone defects were investigated by the Mann-Whitney U test. Statistical analysis was performed with JMP software (version 13.1.0; SAS Institute). In all analyses, statistical significance was accepted at P < .05.
Results
Frequency of Osteophytes on Affected and Unaffected Sides
Table 1 shows the breakdown by age group of osteophytes on the affected side of all study patients (N = 214) as well as those on the unaffected side among patients with osteophytes on the affected side. The osteophyte-positive rate was ≥50.0% in all patients aged ≥31 years, and osteophytes were also frequently detected on the unaffected side among these patients. When the patients were divided into those aged ≤30 years (n = 172) versus ≥31 years (n = 42), the frequency of osteophytes on the affected side was significantly higher in the older group than in the younger group (71.4% [30/42] vs 13.9% [24/172], respectively; P < .001), although osteophytes were not uncommon in the younger group. In addition, the frequency of osteophytes on the unaffected side among patients with osteophytes on the affected side was also significantly higher, 66.7% (20/30) in the older OA group versus 12.5% (3/24) in the younger OA group (P < .001), demonstrating that older patients often had bilateral glenoid osteophytes.
Frequency of Glenoid Osteophytes

Profile of Patients With Osteophytes
Among the patients with osteophytes on the affected side, the younger OA group included 22 male and 2 female patients. Their mean age was 23.1 ± 4.3 years (range, 16-30 years) at CT and 18.8 ± 3.8 years (range, 14-28 years) at initial injury, while the mean interval from initial injury to the CT examination was 4.0 ± 3.8 years (range, 0-13 years). The total number of instability events was 1 in 1 patient, 2-5 in 10 patients, 6-9 in 5 patients, and ≥10 in 8 patients. The older OA group comprised 22 male and 8 female patients, with a mean age of 49.1 ± 12.2 years (range, 31-82 years) at CT and 35.7 ± 18.9 years (range, 14-75 years) at initial injury. The mean interval from initial injury to the CT examination was 13.3 ± 11.4 years (range, 0-33 years) for this group, and the total number of instability events was 1 in 9 patients, 2-5 in 11 patients, 6-9 in 6 patients, and ≥10 in 4 patients. Although the total number of instability events was significantly higher in the younger OA group than in the older OA group (P < .02), there was no significant difference in the interval from initial injury to CT between these 2 groups (P = .09). The mean glenoid bone defect size was 10.9% ± 7.0% (range, 0%-21.3%) in the younger OA group and 10.0% ± 9.9% (range, 0%-30.8%) in the older OA group; this difference was not significant (P = .84).
Comparison of Shoulders With and Without Osteophytes
Demographic data were compared between patients with and without osteophytes to investigate factors related to osteophyte formation (Table 2). The mean interval from initial injury to CT was significantly longer for patients with versus without osteophytes in the younger group (4.0 vs 0.9 years, respectively; P < .001) but not in the older group. Similarly, there was a significant difference in the number of multiple-instability events in younger patients with versus without osteophytes (P = .002). In both groups, the glenoid bone defect was larger in patients with versus without osteophytes, but this difference was only significant for the younger group (P = .02).
Profile of Patients With and Without Osteophytes a

a Data are reported as mean ± SD (range) unless otherwise indicated. “With” and “without” refer to osteophytes found on the affected side. CT, computed tomography.
Characteristics of Osteophytes
On the affected side, the mean osteophyte size was 2.3 ± 1.1 mm (range, 1.0-5.6 mm; SE = 0.23 mm) in the younger OA group and 2.5 ± 0.9 mm (range, 1.0-4.8 mm; SE = 0.18 mm) in the older OA group; there was no significant difference between the 2 groups (P = .51). Figure 2A is a radar chart showing the total number of affected shoulders with osteophytes at each clockface position. In the younger OA group, osteophytes tended to be localized to the anteroinferior part of the glenoid (3 to 6 o’clock) (Figure 2B). In contrast, osteophytes were detected circumferentially around the glenoid in the older OA group, and several patients had osteophytes at the posterior glenoid (6 to 9 o’clock) (Figure 2C).

Localization of osteophytes. (A) The total number of affected shoulders with osteophytes at each clockface position is shown for the younger (solid line) and older (dotted line) OA groups. (B) An anterior glenoid osteophyte at 3 o’clock to 5 o’clock in a 23-year-old patient (arrows). (C) A circumferential glenoid osteophyte in a 51-year-old patient. OA, osteoarthritis.
Influence of Initial Injury Onset in Older OA Group
The early- and late-onset subgroups of the older OA group are compared in Table 3. The mean age at CT was 56.4 ± 14.2 years in the late-onset subgroup versus 42.9 ± 4.9 years in the early-onset subgroup, showing a significant difference (P = .01). While the total number of instability events was significantly higher in the early-onset compared with the late-onset subgroup (P < .001), there was no significant difference in glenoid bone defect size between the 2 groups (P = .89).
Patients With Osteophytes in the Older OA Group by Age at Initial Injury a
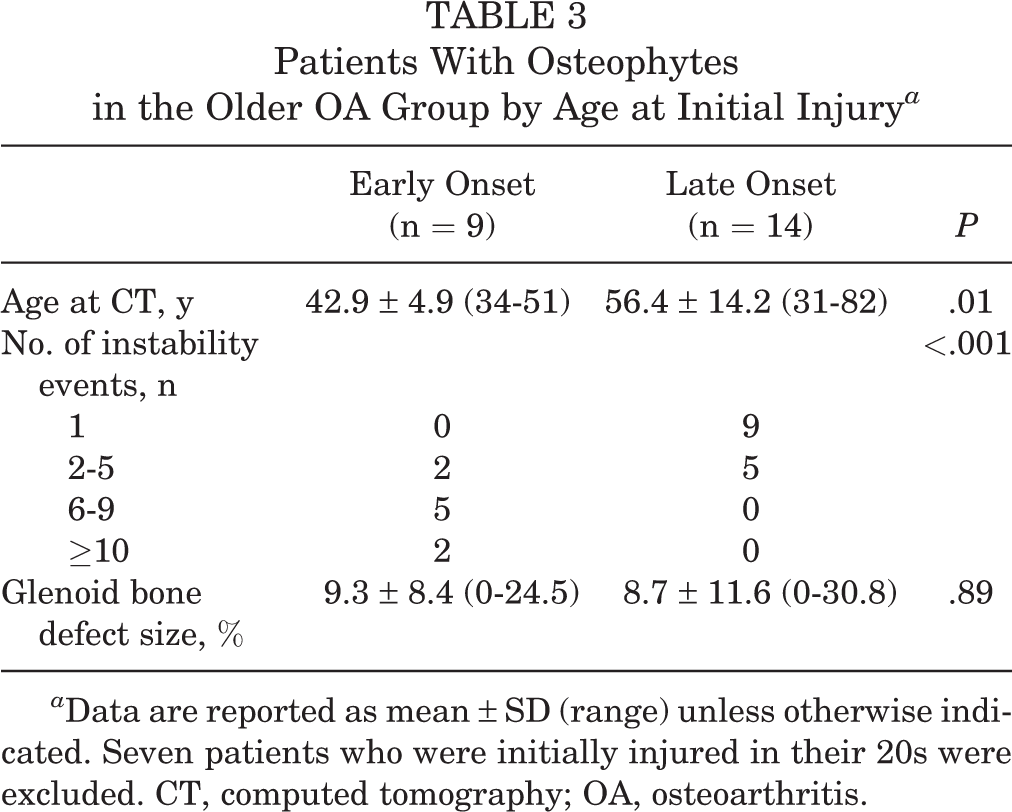
a Data are reported as mean ± SD (range) unless otherwise indicated. Seven patients who were initially injured in their 20s were excluded. CT, computed tomography; OA, osteoarthritis.
There were 4 (44.4%) patients with osteophytes on the unaffected side in the early-onset subgroup versus 11 patients (78.6%) in the late-onset subgroup, but this difference was not significant (P = .11). The mean osteophyte size was 2.2 ± 1.2 mm in the early-onset subgroup and 2.7 ± 1.1 mm in the late-onset subgroup, also showing no significant difference (P = .22). In the late-onset subgroup, osteophytes were relatively circumferential around the glenoid except at the 11-o’clock position, while osteophytes were more likely to be located at the anteroinferior glenoid in the early-onset subgroup (Figure 3).

The total number of affected shoulders with osteophytes at each clockface position is shown for the early-onset (solid line) and late-onset (dotted line) subgroups of the older osteoarthritis group.
Discussion
In this study, we used CT to evaluate the frequency and characteristics of osteophytes in unoperated shoulders with traumatic anterior instability. We demonstrated that the prevalence of osteophytes was high in the affected shoulders among older patients, while it was also not low among younger patients. When the patients were divided into older and younger groups, we found that 13.9% of younger patients and 71.4% of older patients had osteophytes on the affected side. Therefore, this CT-based study identified a higher frequency of osteophytes on the affected side in both groups.
Niskanen et al 11 investigated the radiographs of 52 unoperated shoulders with anterior instability and reported OA changes such as joint space narrowing or osteolysis in only 6 shoulders. Several other investigations of OA in unstable shoulders based on radiographs have found a prevalence of less than 20%, 2,8,19 while Rachbauer et al 15 and Hawkins and Hawkins 7 detected no OA changes preoperatively. While we only focused on glenoid osteophytes in this study, the frequency of identifying such osteophytes by CT was higher than by an investigation using radiographs, suggesting that a precise CT evaluation is more effective for the diagnosis of OA in shoulders with traumatic anterior instability.
To our knowledge, there has only been 1 previous report about CT of OA in shoulders with anterior instability. Ogawa et al 12 compared the diagnosis of OA by CT and radiography in unoperated shoulders with unilateral instability. They detected OA changes on radiographs in only 32 patients (11.3%), while OA changes were detected by CT in 88 patients (31.2%), corresponding to our higher OA diagnosis rate using CT. However, they only investigated the anteroinferior part of the humeral head and did not evaluate the glenoid. Thus, the present study is the first CT investigation of the characteristics of OA changes affecting the glenoid in shoulders with traumatic anterior instability.
Our comparison of demographic data between the younger and older patients with osteophytes only identified a significant difference in the total number of instability events, with younger patients who had osteophytes on the affected side suffering more episodes of dislocation/subluxation during the period before CT compared with the older patients. In the younger group overall, the 24 patients with osteophytes had a significantly longer interval from initial injury, more total instability events, and larger glenoid bone defects than the 148 patients without osteophytes. These results suggest that anterior shoulder instability itself may influence the formation of osteophytes around the glenoid. On the other hand, there were no significant differences in these factors between patients with and without osteophytes in the older group, suggesting that the influence of shoulder instability on osteophyte formation might be smaller among older patients. Osteophytes were already present in some patients with the initial injury, indicating the occurrence of dislocations in shoulders with pre-existing OA and suggesting that aging might contribute more to OA changes than instability events in older patients.
In the present study, we assessed the detailed characteristics of osteophytes among patients stratified by age, including frequency, predisposing factors, size, and location. There was no significant difference in osteophyte size between the younger and older OA groups, which implied that age did not influence the growth of osteophytes. In other words, osteophytes caused by shoulder instability grew to a certain size, irrespective of whether the patient was younger or older. However, osteophyte location demonstrated a different trend compared with that of osteophyte size. In the younger OA group, osteophytes were frequently detected at the anteroinferior part of the glenoid, while osteophytes were detected circumferentially around the glenoid except at the 11-o’clock position in the older OA group. These results seem to indicate the importance of anteroinferior instability in the formation of osteophytes among younger patients, while the influence of aging is a major factor in older patients.
Interestingly, our additional comparison among older patients with osteophytes based on the timing of the initial injury revealed a difference in osteophyte location between the early- and late-onset subgroups, with osteophytes being more frequently detected around the anteroinferior part of the glenoid in the early-onset subgroup. This finding can be explained as follows. Anterior instability presumably existed for a longer period in the early-onset subgroup compared with the late-onset subgroup, leading to long-term adverse effects of various stresses on the shoulder joint, such as impingement between the anteroinferior part of the glenoid and the humeral head or tension from capsular ligaments. The mean size of the glenoid bone defect was 9.3% ± 8.4% in the early-onset subgroup and 8.7% ± 11.6% in the late-onset subgroup, showing no significant difference, which suggests that instability had an important influence on osteophyte formation because the bone morphology was similar in both groups.
The clinical relevance of identifying osteophytes in shoulders with anterior instability before stabilizing surgery is still controversial. Ogawa et al 13 evaluated osteophytes in preoperative and postoperative unstable shoulders by using both radiographs and CT. They concluded that osteophytes could be detected postoperatively by radiography in only 6 of 123 shoulders without osteophytes on preoperative CT, while osteophytes became detectable by radiography after surgery in 12 of 32 shoulders with osteophytes on preoperative CT. In other words, it seems that few new osteophytes are formed after shoulder stabilization surgery and that most postoperative osteophytes represent enlarged preoperative osteophytes, suggesting the importance of detecting the presence of osteophytes before surgical treatment. We consider that preoperative osteophyte formation might be an indicator of OA progression, which could continue during postoperative follow-up, and that especially younger patients with osteophytes should undergo shoulder stabilization surgery as soon as possible.
Some limitations of this study need to be considered. First, there was a possibility of including some cases with a healed osseous Bankart lesion because of the definition of osteophytes as bony protrusions from the rim of the glenoid fossa. In fact, especially during the assessment of cases with a tiny bony protrusion from the glenoid rim, we could not determine whether it was a degenerative osteophyte or bone fragment malunion. Second, the evaluation of imaging findings was conducted by a single author, and we did not assess the intraobserver or interobserver reliability of the imaging evaluations. We considered that there was a potential risk of bias due to a single examiner, especially with regard to the evaluation of osteophyte size. Third, there was a significant difference in the mean age at CT between the early- and late-onset subgroups, which could have reduced the reliability of our comparative analysis of these 2 subgroups. Finally, we did not evaluate patient activity levels and outcomes, including pain and functional limitations, in this study. We considered that the influence of early OA changes on functional outcomes in patients with anterior shoulder instability should be assessed in further investigations in the future.
Although the results need to be interpreted in light of the abovementioned limitations, to our knowledge, this is the first CT-based evaluation of OA changes affecting the glenoid in shoulders with traumatic anterior instability. Therefore, these findings should provide useful new information about OA of the shoulder in patients with anterior instability.
Conclusion
CT facilitated the detailed evaluation of glenoid osteophytes in patients with traumatic anterior shoulder instability and revealed that osteophyte formation was not uncommon among younger patients. In particular, we often detected osteophytes around the anteroinferior part of the glenoid on the affected side in younger patients, with a large number of instability events and a long interval from initial injury to the CT evaluation. Among patients aged ≥31 years, those with an initial shoulder injury as teenagers were more likely to have osteophytes around the anteroinferior part of the glenoid than those with an initial shoulder injury during or after their 30s. These findings suggest that the presence of anterior instability itself might influence the development and progression of OA changes in younger patients, while aging might have a greater influence on OA changes than instability in older patients.
Footnotes
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Yukioka Hospital Institutional Review Board.