
Abstract
Background:
Lateral meniscal tears in the stable knee are rare. There are few comparative studies evaluating functional and radiological outcomes of vertical longitudinal and bucket-handle lateral meniscal tears.
Purpose:
To evaluate the midterm clinical and radiological outcomes of arthroscopically repaired traumatic vertical longitudinal and bucket-handle lateral meniscal tears.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 43 full-thickness lateral meniscal repairs, including 22 (51.2%) for vertical longitudinal tears and 21 (48.8%) for bucket-handle tears, were evaluated. A clinical assessment was performed according to the Barrett criteria, and patient outcomes were measured with the Lysholm knee score, Tegner activity scale, and overall satisfaction scale. Magnetic resonance imaging was used as the radiological re-examination method preoperatively and at final follow-up. A subgroup analysis examining isolated repair versus repair with concurrent anterior cruciate ligament (ACL) reconstruction was performed.
Results:
The mean follow-up period was 63.2 months (range, 24-86 months). Based on clinical and radiological outcomes, 38 of the 43 repairs (88.3%) were successful, and the remaining 5 (11.6%) cases were considered to be failures. Overall, the combined results for both groups demonstrated an improvement in the Lysholm score, Tegner score, and patient satisfaction. There was no significant difference in the postoperative Lysholm score (91.4 vs 87.0, respectively; P = .223), Tegner score (5.4 vs 5.5, respectively; P = .872), or patient satisfaction (7.2 vs 7.4, respectively; P = .624) between bucket-handle repair and vertical longitudinal repair. The subgroup analysis demonstrated no difference in outcome scores for isolated repair versus repair with concurrent ACL reconstruction. Smoking was identified as a risk factor for repair failure.
Conclusion:
Comparable clinical and radiological outcomes were obtained after vertical longitudinal and bucket-handle lateral meniscal repairs using the all-inside or hybrid suture technique with different suture configurations, regardless of whether ACL reconstruction was performed. Smoking was identified as a risk factor for failure.
Menisci play a crucial role in load distribution, shock absorption, chondral protection, proprioception, lubrication, and joint stabilization. 15 Meniscectomy has been associated with osteoarthritis in the long term. 24 Therefore, meniscal preservation is important in knee function. Arthroscopic repair of torn menisci has been accepted as the mainstay treatment method if possible. 45 It has been reported that the repair of acute longitudinal tears located in the peripheral vascular zone in young patients with stable knees has the most successful outcomes. 32
The lateral meniscus has different structural and functional properties than the medial meniscus. 7 A lack of attachments to the popliteal hiatus and collateral ligament as well as relative greater mobility reduce the risk of ruptures. 15 An anterior cruciate ligament (ACL) injury commonly accompanies a lateral meniscal tear. 18 Lateral meniscal tears in a stable knee are relatively rare. 1
Vertical longitudinal tears are common in clinical practice. 26 The posterior horn of the lateral meniscus is susceptible to subluxation because of the absence of peripheral attachments of the meniscus in the popliteal hiatus, and this may result in vertical longitudinal tears. 40 Bucket-handle tears are vertical longitudinal tears with central displacement of the inner fragment, 29 and they constitute 10% of all meniscal tears. Usually, their bigger size, displacement, and complexity challenge surgeons. 25
According to the current evidence, meniscal preservation through arthroscopic repair is recommended if possible, depending on age, zone and length of the tear, tear chronicity, and physical activity level of the patient. 10,17,25 Also, it has been reported that ACL reconstruction provides a positive biomechanical environment for the meniscus to heal. 46 The clinical picture of this situation is controversial. 28 Several studies have reported both higher and similar healing rates with concomitant ACL reconstruction. 18,47 –49
To the best of our knowledge, there have been no direct comparative studies involving the repair of full-thickness vertical longitudinal and bucket-handle lateral meniscal tears. Therefore, the purpose of this study was to evaluate clinical outcomes and healing rates after arthroscopic repair of full-thickness vertical longitudinal and bucket-handle lateral meniscal tears.
Methods
Patients and Procedures
From January 2008 to December 2012, a total of 184 patients underwent arthroscopic repair of lateral meniscal tears by 2 surgeons (E.U., A.G.) in our hospital. After excluding patients with discoid meniscal tears (n = 13) or with partial-thickness (n = 64), horizontal (n = 39), and radial tears (n = 25), a total of 43 full-thickness vertical longitudinal (n = 22) and bucket-handle tears (n = 21) located in the red-red (RR) and red-white (RW) zones of the lateral meniscus were included. An ACL rupture was present in 17 of the 43 (39.5%) patients, who underwent concomitant meniscal repair and ACL reconstruction. The remaining 26 repairs (60.5%) were performed in knees with an intact ACL.
In all patients, the diagnosis of the lateral meniscal tear was based on patient history, symptoms, physical examination findings, and magnetic resonance imaging (MRI) results. Concomitant medial meniscal tears were not included. Written informed consent was obtained from all patients. This retrospective study protocol was reviewed and approved by our institutional review board.
Surgical Technique
The meniscal repair procedure was performed, with or without ACL reconstruction, using vertical, oblique, and horizontal sutures via an all-inside or hybrid technique (all-inside and inside-out technique). Different repair techniques were used in different patients. We primarily used an all-inside repair technique, with an inside-out approach, in tears extending from the middle horn to anterior horn. All surgical procedures were performed under combined spinal and epidural anesthesia. A tourniquet was used to enhance visualization during surgery. Anteromedial and anterolateral arthroscopic portals were used. In tears with extension to the anterior horn, an accessory medial portal, in addition to anteromedial and anterolateral portals, was used for inside-out repair. Also, zone-specific curved cannulas were used for the inside-out repair technique.
All 3 compartments of the knee were examined, with the meniscal tear probed to confirm if it was full-thickness and to determine if the tear was in the RR or RW zone of the meniscus. For displaced bucket-handle tears, a reduction maneuver was performed before the repair procedure. After optimal reduction of the tear, vertical, oblique, or horizontal sutures were used for repair. Superior or posterior sutures were placed first, followed by inferior or anterior sutures. This repair process was repeated, with stitches placed every 5 to 8 mm along the length of the tear. For the inside-out technique, a 2-cm skin incision was made for dissection through the joint capsule, and the Zone Specific II Meniscal Repair System (Linvatec) was used for the repair procedure. The Fast-Fix 360 Meniscal Repair System (Smith & Nephew) was used for all-inside repair. Sutures were tightened and tied over the capsule, with posterior sutures tightened with the knee in 45° to 60° of flexion and anterior sutures tightened with the knee in 0° to 20° of flexion. After completing the repair procedure, the tear was probed to assess the stability of the meniscal construct.
For patients with an ACL deficiency, autologous semitendinosus and gracilis tendon grafts were harvested. Then, inside-out sutures were passed, if required. Femoral and tibial tunnels were drilled, the harvested ACL graft was placed in the tunnels, and inside-out sutures were tightened. Then, all-inside sutures were placed and tibial fixation of the ACL performed. For femoral fixation, the Endobutton CL Ultra (Smith & Nephew) was used. A bioabsorbable screw (Biosure HA; Smith & Nephew) and a staple (Smith & Nephew) were used for tibial fixation.
Postoperative Rehabilitation
Patients who underwent isolated meniscal repair and those who underwent meniscal repair with ACL reconstruction completed the same postoperative rehabilitation program. 5 Patients who had undergone repair of a vertical longitudinal tear were permitted 0° to 90° of knee flexion over the first 4 weeks after surgery, while patients who had undergone repair of a bucket-handle tear were maintained in a position of full knee extension, using a brace, for the first 2 weeks after surgery, followed by gradual range of motion into knee flexion. All patients achieved 90° of knee flexion by 4 weeks after surgery. From 6 to 10 weeks after surgery, all patients gradually recovered their maximum range of knee flexion. All patients were allowed to bear weight 4 weeks after surgery. They gradually recovered their maximum range of knee flexion at 6 to 10 weeks after surgery.
Clinical and Radiographic Outcomes
After repair, a clinical assessment was conducted based on the Barrett criteria, including no swelling or locking of the knee joint, no pain or joint-line tenderness on palpation, free motion, and negative McMurray test findings. 6 A radiographic examination was performed using MRI (T1 and T2 coronal, sagittal, and axial views) in all patients at the final follow-up visit. If the patient had ≥3 clinical findings (Barrett criteria) and/or a grade 3 signal on T2 sequences (Figure 1), the repair was considered to have failed. If the patient had a positive McMurray test result, joint-line tenderness on palpation, and/or MRI evidence of fluid within the repair site, the repair was considered to be a failure. 15,47 Lysholm knee scores, Tegner activity scores, and patient satisfaction scores (on a scale of 1-10, with 10 being most satisfied) were evaluated for all patients preoperatively and at final follow-up. 43 A subgroup analysis was performed to examine differences between bucket-handle repair and vertical longitudinal repair in addition to isolated repair versus repair with concurrent ACL reconstruction. We also examined patient risk factors for repair failure, including patient age, affected side, tear length, tear type, location of the repair, concurrent ACL reconstruction, suturing technique, and patient smoking status.

(A) Coronal and (B) sagittal T2 magnetic resonance imaging sequences of a 35-year-old patient with failure of lateral meniscal repair.
Statistical Analysis
The following descriptive variables were calculated: mean, standard deviation, median, range, frequency, and percentage. The normality of the distribution for measured outcome variables was evaluated using the Kolmogorov-Smirnov test. The Mann-Whitney U test was used to evaluate quantitative data, and the chi-square test and Fisher test were used for qualitative data. A P value of <.05 indicated statistical significance. Data were analyzed using SPSS (v 22.0; IBM).
Results
The mean clinical follow-up period was 63.2 ± 12.7 months (range, 24-86 months). Table 1 provides a summary of overall patient characteristics, and Table 2 provides a comparison of relevant patient and tear characteristics between patients who underwent isolated lateral meniscal repair (n = 26) and those who underwent repair with concomitant ACL reconstruction (n = 17). A significant difference in operative time was identified between isolated repair (36.7 ± 9.2 minutes) and repair with concurrent ACL reconstruction (78.2 ± 6.8 minutes) (P < .05).
Overall Patient Demographics a

a Data are reported as mean ± SD or n (%). ACL, anterior cruciate ligament.
Patient and Tear Characteristics According to Study Group a
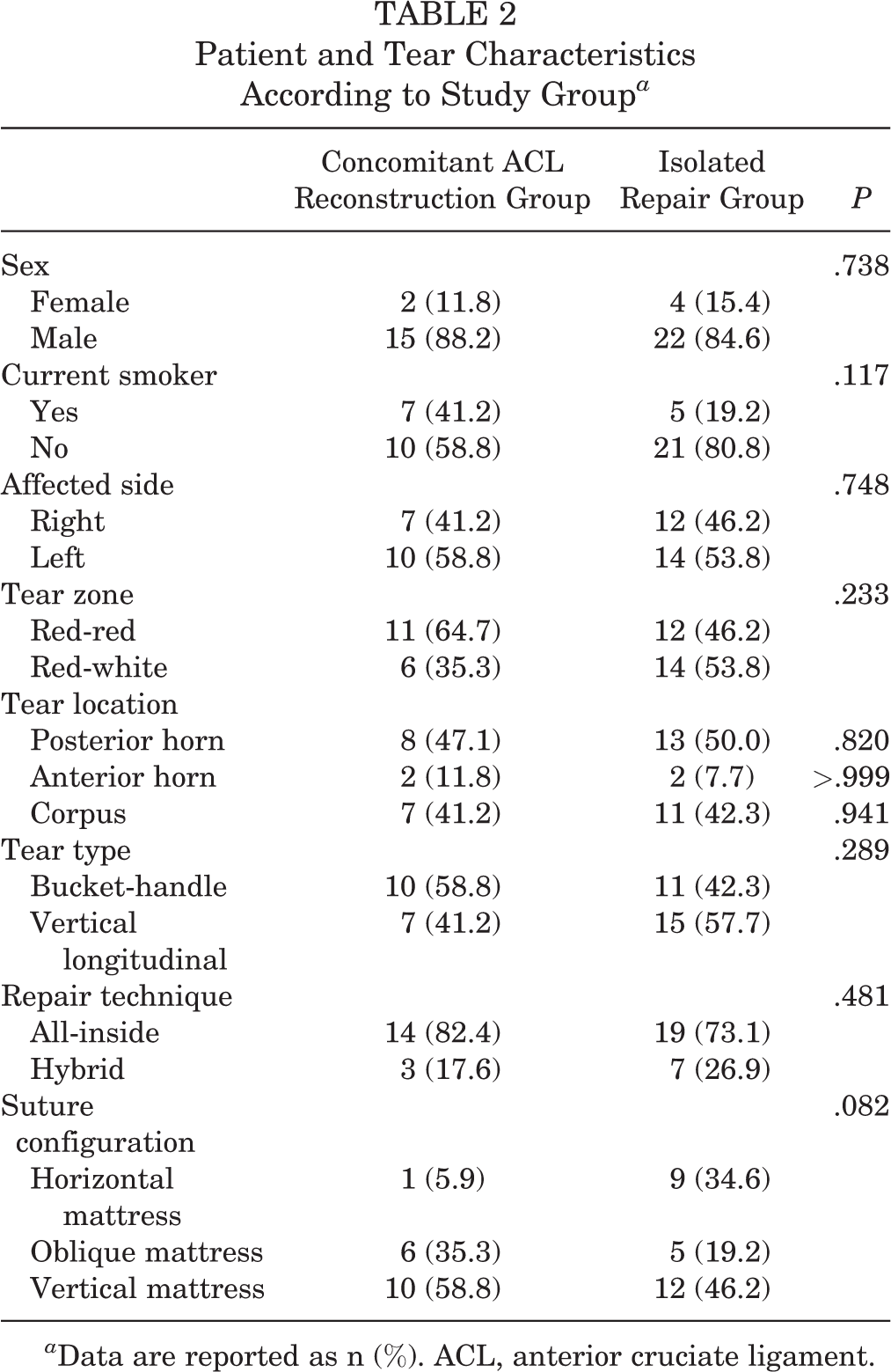
a Data are reported as n (%). ACL, anterior cruciate ligament.
An all-inside technique was used in 33 cases, and a hybrid technique used in 10 patients. The mean number of sutures used was 3.8 ± 0.8 (range, 2-6): 1.4 ± 0.8 (range, 1-2) inside-out sutures and 2.4 ± 0.7 (range, 1-4) all-inside sutures. Suture types and configurations used in repairs are shown in Tables 3 and 4.
Suture Types and Configurations a

a Data are reported as mean ± SD (range) or n (%).
Comparative Patient Characteristics a
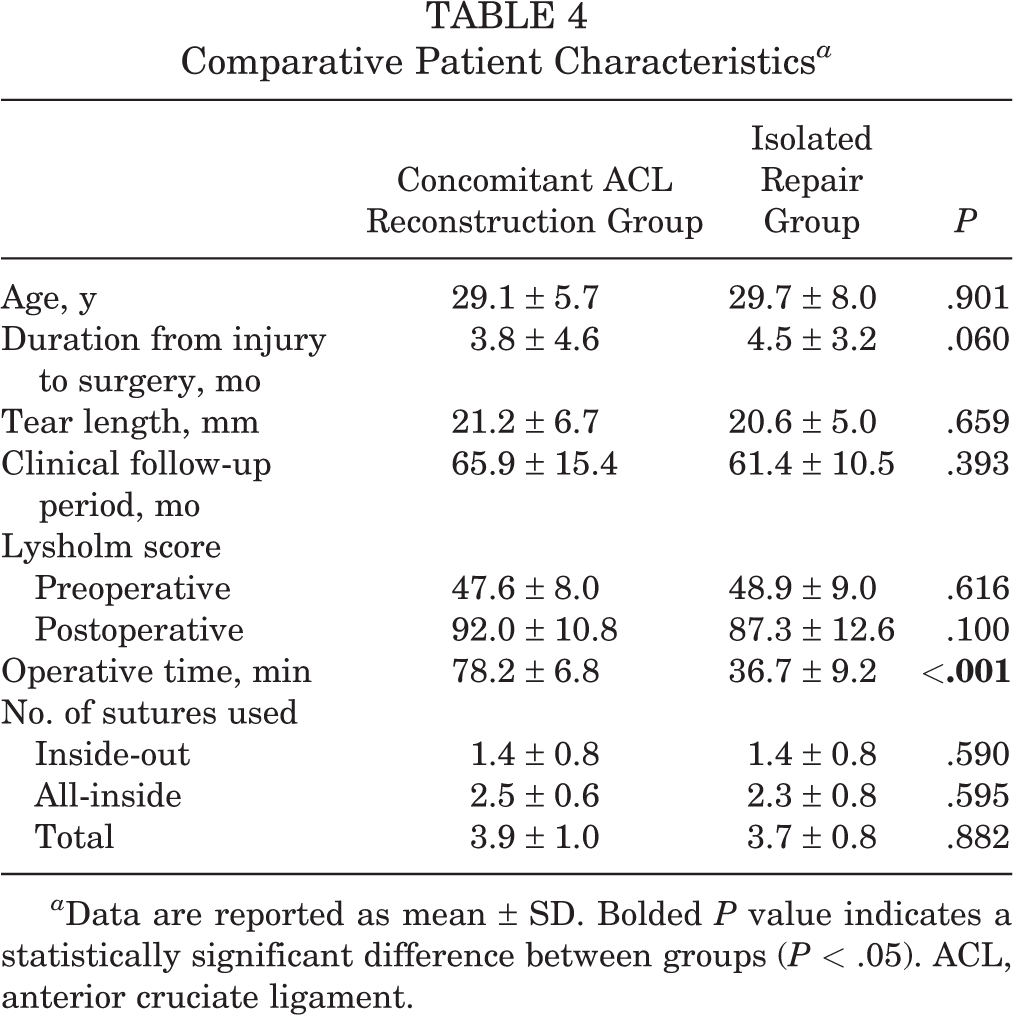
a Data are reported as mean ± SD. Bolded P value indicates a statistically significant difference between groups (P < .05). ACL, anterior cruciate ligament.
The mean Lysholm score in all patients improved from 48.4 ± 8.5 (range, 32-62) preoperatively to 89.2 ± 12.0 (range, 60-100) at the final follow-up visit (P < .001). The median Tegner score improved from 3 (range, 2-6) preoperatively to 7 (range, 4-9) postoperatively (P < .05). The mean patient satisfaction score improved from 3.3 ± 2.8 (range, 1-5) preoperatively to 7.7 ± 2.2 (range, 6-10) postoperatively (P < .05).
There was no significant difference in the postoperative Lysholm score (91.4 vs 87.0, respectively; P = .223), Tegner score (5.4 vs 5.5, respectively; P = .872), or patient satisfaction (7.2 vs 7.4, respectively; P = .624) between the bucket-handle tear group and vertical longitudinal tear group (Table 5). Also, there was no significant difference in the postoperative Lysholm score (87.4 vs 90.7, respectively; P = .096), Tegner score (5.3 vs 5.7, respectively; P = .574), or patient satisfaction (6.9 vs 7.6, respectively; P = .227) between the isolated repair group and repair with concurrent ACL reconstruction group (Table 6).
Comparative Outcome Scores for Bucket-Handle Versus Vertical Longitudinal Tear Repair a

a Data are reported as mean ± SD. ACL, anterior cruciate ligament.
b Graded from 1 to 10 (most satisfied).
Comparative Outcome Scores for Isolated Repair Versus Repair With Concurrent ACL Reconstruction a

a Data are reported as mean ± SD. ACL, anterior cruciate ligament.
b Graded from 1 to 10 (most satisfied).
Of the 43 patients included in this study, the repair was considered to be clinically successful in 38 (88.3%) cases, with patients being symptom-free at the final follow-up visit and having no (or minimal) limitation in activities of daily living; patients in both the bucket-handle and vertical longitudinal tear groups returned to their preinjury activity levels within 6 months after surgery. Based on the clinical scores, Barrett criteria, and MRI findings, clinical failure was identified in 5 (11.6%) cases at the final follow-up visit. Clinical failure was detected in 4 (80.0%) cases and MRI failure in 5 (100.0%) cases. The mean time to failure, from the time of repair, was 12.8 ± 8.1 months (median, 11 months; range, 5-24 months) postoperatively.
With respect to the failure rates of vertical longitudinal and bucket-handle lateral meniscal repairs, no differences were identified in terms of age, affected side, tear length, tear type, location of the repair, concurrent ACL reconstruction, or suturing technique (P > .05) between patients with and without failure of the repair. Smokers were found to have a higher rate of repair failure for both vertical longitudinal and bucket-handle repairs (P < .05). Among the 5 cases of failure, 1 was caused by an infection, localized around sutures, which was treated with debridement, partial meniscectomy, and intravenous antibiotic therapy. Of the remaining 4 patients with repair failure, 3 cases (2 isolated vertical longitudinal repairs and 1 isolated bucket-handle repair) were treated with partial meniscectomy, while the remaining case (vertical longitudinal repair in conjunction with ACL reconstruction) was suitable for revision, with the repair completed using a hybrid technique. Three of these patients were smokers, their meniscal tears were located in the RW zone, and a horizontal or oblique mattress configuration was used in their repairs. In the MRI examination, increased intrameniscal signal intensity that reached the articular surface and/or meniscal shape abnormalities (contour irregularity, volume reduction, or fragment displacement) were observed.
Discussion
Our study provided evidence of successful clinical outcomes after arthroscopic repair of vertical longitudinal and bucket-handle lateral meniscal tears, with low failure rates and complications. It is well known that the prognosis of meniscal repairs depends on the type of meniscal tear and the presence or absence of an articular cartilage lesion. 45 In our series, we found no significant difference in healing rates or functional scores between vertical longitudinal tears and bucket-handle tears. None of the patients in either group had an articular cartilage lesion. Osti et al 33 reported that athletes with isolated longitudinal tears of the lateral meniscus had the best clinical outcomes after arthroscopic repair, with all athletes in their case series achieving good to excellent results and a full return to athletic activities at a mean of 41 days after meniscal repair. However, athletes with complex meniscal tears required, on average, 64 to 78 days to return to their full sports activities. For vertical longitudinal and bucket-handle tears, return to sports was allowed at 3 months. 12 In our study, return to sports activities was within 71 to 127 days.
Meniscal repair in conjunction with ACL reconstruction has been reported to create a favorable environment for meniscal healing because of an increase in bone marrow–derived intra-articular stem cells and knee joint stability. 11,19,27,38,46 Moreover, a prolonged recovery and rehabilitation protocol after ACL reconstruction may provide a protective effect, forcing low activity levels postoperatively. 22 In fact, age-specific physical therapy protocols have been developed to lower the risk of recurrent injuries after meniscal repair. 2,3,21,51 Tachibana et al 42 reported a healing rate of 74%, on second-look arthroscopic surgery, for meniscal repair performed concurrently with ACL reconstruction, with a 15% rate of incomplete healing and an 11% rate of nonhealing. In our study, there was no significant difference in healing rates between repairs of the lateral meniscus performed in isolation or concurrently with ACL reconstruction. The similar healing rates might be associated with similar knee stability levels in both groups. Therefore, our results do not support a previous work reporting a lower risk of failure for lateral meniscal repair performed with concurrent ACL reconstruction verus in isolation. 22
Patient age is a controversial issue regarding its role in healing of a meniscal tear. Gobbi et al 13 reported a higher rate of subsequent meniscectomy in patients younger than 30 years. In contrast, Noyes and Barber-Westin 30,31 reported comparable rates of healing for younger and older patients, even for tears in the avascular middle zone of the meniscus, where healing has previously been thought to be less likely. In our case series, 3 of our 5 (60.0%) cases of failure were in patients younger than 30 years.
Based on the current evidence, a failure rate of meniscal repair of 0% to 23% has been estimated. 28 Healing after meniscal repair depends on multiple factors that include the size of the tear, location of the tear and blood supply, time from injury to surgery, rehabilitation protocol, and surgical technique. Surgical technique plays a significant role in patient outcomes, and therefore, the optimal repair technique should be carefully considered on a case-by-case basis. 35 The inside-out technique is considered to be the gold standard repair method but is associated with an increased risk of neurovascular injuries and perioperative morbidity. 50 The all-inside meniscal repair technique is less invasive than the inside-out technique and requires a shorter operative time, which is associated with a lower rate of morbidity and complications. 23,37,41 However, a systematic review comparing the clinical outcomes of inside-out and all-inside meniscal repair techniques, for isolated peripheral, longitudinal, unstable meniscal tears, did not identify a clear benefit of one technique over the other in terms of structural healing or perioperative complications. 14 An anteromedial accessory portal and zone-specific cannulas were used in the inside-out approach.
With regard to the failure mode, pullout through the meniscal material has been reported as the predominant cause of tissue failure for horizontal suture repair, whereas suture breakage has been the predominant cause for vertical suture repair. 39 These mechanical characteristics are attributable to the ability of vertical sutures to capture more of the circumferentially oriented collagen fibers that run along the long axis of the meniscus than horizontal sutures. 4,35,42 In our case series, horizontal sutures had been used in 3 of the 5 cases of repair failure, with oblique sutures used in 1 other case and a vertical configuration in the remaining case. In terms of horizontal sutures, those placed slightly farther from the region of the meniscal tear provided superior repair fixation compared with sutures placed closer to the lesion, as previously described. 20 Therefore, the failure rate of repairs may be decreased using this approach when horizontal sutures are used. Currently, the optimal number of stitches required to stabilize a meniscal tear is not known. Most authors advocate the placement of sutures spaced every 3 to 5 mm along the tear when using an inside-out technique, with 4.9 to 8.2 sutures used on average. 9,11,44 For all-inside repair, 2 to 3 sutures are used, on average, to complete the repair procedure. 42 In our case series, we used 3.8 sutures, on average, to complete the repair. As additional suture placement may increase the risk of damage to the meniscus, longer and unstable tears can be treated with hybrid repair using an all-inside plus inside-out suture technique.
Recently, Moatshe et al 25 reported comparable outcomes after acute and chronic bucket-handle and vertical repairs of medial and lateral menisci at a mean 3.1-year follow-up. Their repair technique included multiple vertical mattress sutures using an inside-out technique, with a mean of 11 sutures for bucket-handle repair and 7 sutures for vertical repair. They reported no meniscal healing failure. Their study included both medial and lateral meniscal repairs. In our study, we evaluated patient outcomes at a mean 5.3-year follow-up. Our repair procedure included vertical, oblique, and horizontal mattress sutures using all-inside and hybrid (all-inside and inside out) techniques. We used a mean of 3.0 (range, 2-5) sutures for bucket-handle repair and 2.5 (range, 2-4) sutures for vertical longitudinal repair. Five repairs (11.6%) failed. Our higher failure rate may be associated with the relatively low suture count, the oblique and horizontal mattress configuration, and the inside-out or hybrid repair technique. Because of the lack of tear length data in their article, 25 we could not compare the suture count per centimeter, and their technique may not be cost-effective. Future randomized controlled studies with different suture counts and the same techniques may show an optimum suture count.
The effect of smoking on soft tissue healing, including the meniscus, has been previously investigated. 8,15,16,51 Blackwell et al 8 reported that smoking was associated with a significantly increased risk of early failure of meniscal repair. In their comparison of the clinical outcomes after meniscal repair among 14 smokers and 11 nonsmokers with 33 lateral meniscal tears, Blackwell et al 8 reported a 15% risk of repair failure specifically associated with smoking. In our study, the overall rate of repair failure was 11.6%. When considering smoking as a specific risk factor, the failure rate among smokers was 25.0% (3 failures among 12 repairs) compared with 3.2% for nonsmokers (1 failure among 31 repairs).
An increase in the rate of secondary meniscal injuries, especially when surgery is postponed beyond 3 months, has previously been reported in patients with ACL-deficient knees. 34,36 In our study, the mean time from injury to surgery was 3.8 ± 4.6 months in the repair with concomitant ACL reconstruction group. The mean time between injury and surgery might have contributed to increased tearing within the lateral meniscus.
The limitations of our study need to be acknowledged. These include a relatively small number of patients, a relatively short follow-up period, and no second-look arthroscopic assessment, except in cases of failed repairs. The retrospective design of our study is an inherent weakness, with a potential for selection bias. Our study cohort included only patients with either vertical longitudinal or bucket-handle tears of the lateral meniscus. All patients underwent the same meniscal repair procedure but with different suture configurations and combinations selected on a case-by-case basis. In addition, the rehabilitation program differed between patients depending on the repair technique and characteristics of the tear. Despite these limitations, our study focused specifically on isolated repair of full-thickness vertical longitudinal and bucket-handle lateral meniscal tears in ACL-intact knees versus repair with concomitant ACL reconstruction.
Conclusion
Successful and comparable clinical outcomes and high patient satisfaction with low failure rates were obtained for arthroscopically repaired vertical longitudinal and bucket-handle lateral meniscal tears using the all-inside or hybrid technique with different suture configurations, regardless of whether ACL reconstruction was performed. Smoking was identified as a risk factor for failure.
Footnotes
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Erciyes University Clinical Investigations Ethics Committee (No. 2014-530).