
Abstract
Background:
Medial patellofemoral ligament (MPFL) reconstruction is the treatment of choice for recurrent patellar instability in the skeletally immature patient. Avoiding the open physes during anatomic MPFL reconstruction is a challenge in this population.
Purpose:
To describe a novel method using magnetic resonance imaging (MRI) to determine the distance from the Schöttle point to the medial distal femoral physis among skeletally immature individuals with patellar instability.
Study Design:
Descriptive laboratory study.
Methods:
Preoperative MRI scans were analyzed from 34 patients with open distal femoral physes and lateral patellar instability. With the multiplanar reconstruction mode on a picture archiving and communication system (PACS), the location of the Schöttle point was determined according to previously reported distances from the posterior femoral cortical line and the posterior origin of the medial femoral condyle. This location was then extrapolated to the most medial sagittal slice on MRI showing the medial distal femoral physis. The distance was measured from this point to the most distal aspect of the physis.
Results:
The mean age of the study cohort was 13.6 years (range, 10.6-15.7 years); there were 13 males and 21 females. The mean distance from the medial distal femoral physis to the Schöttle point was 7.27 ± 1.78 mm. The Schöttle point was distal to the medial distal femoral physis in all cases. There was no significant correlation between age and mean distance in either the overall study population (r = 0.046, P = .798) or when stratified by sex (females, P = .629; males, P = .089). The distance between the Schöttle point and the medial distal femoral physis was shorter for females than for males (6.51 vs 7.71 mm, P = .043). After adjustment for age, females on average were 1.31 mm closer to the Schöttle point than were males (B = –1.31, P = .041).
Conclusion:
This technique can be used to determine the distance between the medial distal femoral physis and the Schöttle point. The Schöttle point was distal to the physis in all patients, and it was closer to the physis in skeletally immature females compared with age-matched males.
Clinical Relevance:
The long-term repercussions of improperly placed MPFL reconstruction include recurrent patellar instability, increased patellofemoral contact pressures and overtensioning of the ligament, and possibly patellofemoral arthritis. The current technique can be used preoperatively to determine the appropriate safe distance for drilling a socket distal to the physis.
Keywords
Patellar instability is a common injury in the active youth population, with an estimated annual incidence of first-time dislocations of 5.8 per 100,000 4 and incidence increasing to 43 per 100,000 in children younger than 16 years. 15 Fithian et al 4 found the highest risk to be among females aged 10 to 17 years. Skeletal immaturity is among other anatomic factors that have been associated with a higher risk of patellar dislocation. 6,10,11
Medial patellofemoral ligament (MPFL) reconstruction is the treatment of choice for patients with recurrent patellar instability. Using cadaveric specimens confirmed by fluoroscopy, Schöttle et al 19 and Redfern et al 17 identified anatomic landmarks on the medial femoral condyle to reproducibly identify the femoral insertion of the MPFL, which included a point 1 mm anterior to the posterior cortex extension line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to the level of the Blumensaat line on lateral radiograph. In MPFL reconstruction, anatomic reconstruction is recommended, as graft malpositioning has been shown to alter patellofemoral biomechanics and lead to increased force and contact pressure to the medial patellofemoral cartilage. 2,18 Parikh et al 16 showed that 47% of complications in MPFL reconstruction among young patients were due to preventable technical factors, with one-third of these complications associated with improper femoral tunnel placement.
In the skeletally immature patient, the relationship between the femoral insertion of the MPFL and the femoral physis is important. The challenge is achieving anatomic fixation on the femoral side while respecting the open physis. 14 Physeal safety is critical to prevent leg length discrepancy and angular deformity. Additionally, anatomic reproduction of the femoral insertion site of the MPFL is important for re-creating an isometric MPFL reconstruction and for potentially long-term outcomes regarding cartilaginous wear of the patellofemoral compartment. 2,12
Prior cadaveric and radiographic studies 1,5,8,13,20 –22 have shown anatomic variation in the distance between the femoral insertion of the MPFL and distal femoral physis, with the distance generally being within millimeters of the physis. Other factors, such as age and sex, have also been suggested to influence this distance in patients with open physes. 1,5,21 Magnetic resonance imaging (MRI) is normally obtained preoperatively after a patellar instability event to evaluate for concomitant injuries, including osteochondral fractures and/or loose bodies. MRI is a preferred imaging modality in the skeletally immature population given its lack of ionizing radiation.
We present a novel method for determining the distance from the Schöttle point to the medial distal femoral physis on MRI that can be translated to a safe intraoperative location for femoral socket placement in MPFL reconstruction via an all-epiphyseal technique. We hypothesized that this method will be reproducible between measurers. We also hypothesized that the distance between the Schöttle point and the distal femoral physis will be anatomically close and will decrease from the MPFL origin, becoming more proximal with increasing age and being less for females than males after adjusting for age.
Methods
After institutional review board approval, we retrospectively reviewed MRI scans (1.5- or 3.0-T magnets; General Electric Healthcare) performed from 2011 to 2017 in 34 children and adolescents after acute lateral patellar dislocation. An electronic picture archiving and communication system (PACS; Sectra IDS7) was used to identify patients who underwent knee MRI at a single institution. Patients were eligible for inclusion if they were between 10 and 16 years old and skeletally immature and had recently sustained a patellar dislocation. Exclusion criteria included previous surgical treatment and significant congenital or syndromic structural abnormality.
The MRI scans were independently reviewed by a sports medicine fellowship–trained attending physician with a practice focus on patellar instability (B.S.S.; senior author) and a current sports medicine fellow (M.E.B.). Using the sagittal proton density series and multiplanar reconstruction mode on our PACS to create a perfect lateral image, we determined the location of the Schöttle point based on previously reported distances from the posterior femoral cortical line and posterior origin of the medial femoral condyle (Appendix and Figure 1). This location was then extrapolated to the most medial sagittal slice on MRI showing the medial distal femoral physis. The distance was measured from this point to the most distal aspect of the physis (Figure 2).
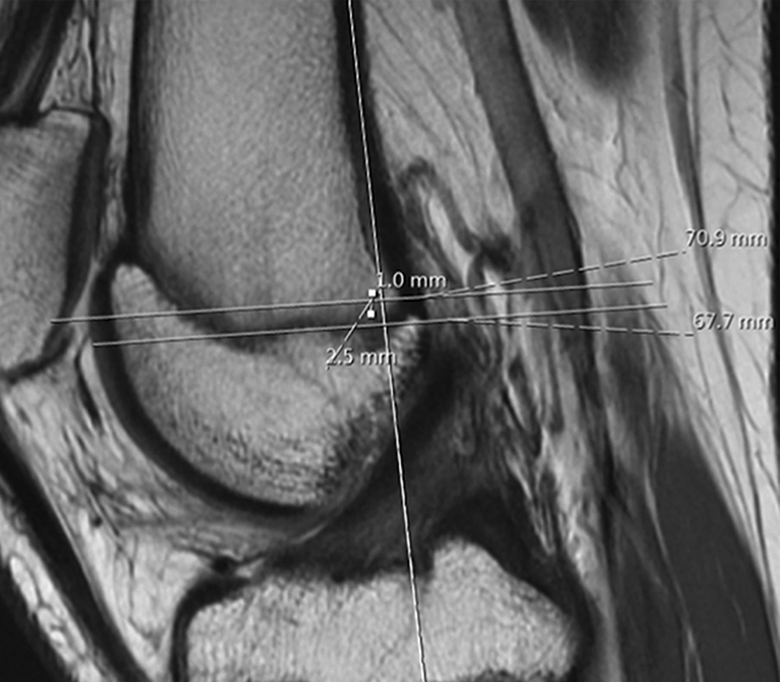
Using the sagittal series on magnetic resonance imaging, a line is made in line with the posterior femoral cortex on the image with the best view of the anterior cruciate ligament. A second line is drawn at the most posterior aspect of the Blumensaat line perpendicular to the posterior cortical line. A third line is drawn at the most proximal aspect of the posterior femoral condyle that is perpendicular to the posterior cortical line. A point is measured that is 1 mm anterior to the posterior cortical line and 2.5 mm distal to the medial femoral condyle line, designated as the Schöttle point.

Scroll to the farthest sagittal image where the physis is still visible on the medial femoral condyle. Measure the proximal-distal distance from the physis to the Schöttle point in a line perpendicular to the posterior femoral cortex. Here the distance is 6 mm.
Statistical Methods
Shapiro-Wilks tests were performed to evaluate the assumption of normality for all continuous variables. The intraclass correlation coefficient (ICC) was used to determine interrater reliability of mean distance measures between the senior author and the fellow. The Pearson correlation coefficient was used to evaluate the relationship between the continuous variables of age and mean distance, for the overall population as well as stratified by sex. An independent samples t test was used to compare the mean distance measurements between males and females. Age and sex were included as variables of interest in a multivariable regression model for the dependent variable of mean distance between the Schöttle point and the distal femoral physis. All analyses were performed with SPSS (v 23.0; IBM Corp). Statistical significance was defined as P ≤ .05.
Results
Shapiro-Wilks tests confirmed the assumption of normality for age (P = .157) and mean distance (P = .383). The mean age of the cohort was 13.6 years (range, 10.6-15.7 years). There were 13 males and 21 females (N = 34). The mean ± SD distance from the medial distal femoral physis to the Schöttle point was 7.27 ± 1.78 mm (range, 3.3-10.5 mm). The Schöttle point was distal to the medial distal femoral physis in all cases. The interrater reliability of mean distance between raters was excellent by the standards described by Landis and Koch 9 (ICC = 0.854; 95% CI, 0.708-0.927; P < .001). As reliability was so high between raters, the analysis of data reported is resultant from measurements from a single, randomly selected rater (B.S.S.).
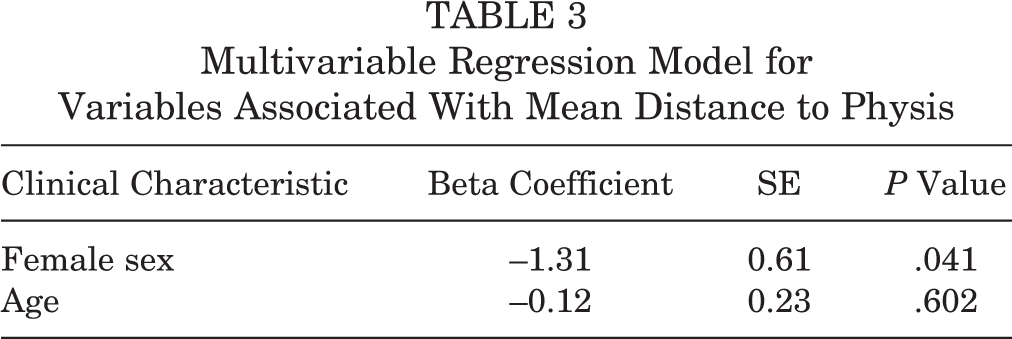
Bivariate correlation between age and mean distance showed no significance for the overall population (r = 0.046, P = .798) (Table 1). When stratified by sex, neither males (P = .089) nor females (P = .629) showed any correlation between age and distance. Results from the independent samples t test showed that on average, females (6.51 mm; range, 3.3-10.5 mm) had a shorter distance to the Schöttle point when compared with males (7.71 mm; range, 4.2-10.2 mm; P = .043) (Table 2). Multivariable regression analysis determined that after adjustment for age, females on average were 1.31 mm closer to the Schöttle point compared with males (B = –1.31, P = .041) (Table 3).
Bivariate Correlation Between Mean Distance to Physis and Patient Age a

a Results of Pearson correlation between the mean distance from the physis to the Schöttle point and patient age at the time of magnetic resonance imaging scan.
Comparison of Mean Distance With Physis and Patient Age Between the Sexes a

a Data are reported as mean ± SD. MRI, magnetic resonance imaging.
Multivariable Regression Model for Variables Associated With Mean Distance to Physis
Discussion
In this study, we demonstrated a reproducible method of measuring the distance between the Schöttle point and the medial distal femoral physis. This novel, reproducible technique can be utilized preoperatively to determine the appropriate safe distance from the physis for socket drilling and fixation entry point using preoperative MRI. Another valuable use for this technique is the ability to assess femoral MPFL location on postoperative MRI in patients with failed MPFL reconstruction. As there is anatomic variation among all patients, this method can offer individualized assessment of the MPFL to the medial distal femoral distance to best re-create anatomy while protecting the physis.
Ensuring physeal safety during MPFL reconstruction is critical in the skeletally immature population, as the standard adult surgical technique of using screw fixation in the distal femur has been shown to frequently disturb the medial distal femoral physis. 5 An understanding of the close proximity of the MPFL origin to the medial distal femoral physis is important when considering screw placement and trajectory, as placement distal to the physis with a distal oblique trajectory has been shown to safely avoid physeal and joint penetration as compared with parallel screw placement. 5 Determining a safe and anatomic starting point is critical during preoperative planning for MPFL reconstruction.
The distance between the femoral insertion of the MPFL and the distal femoral physis has shown anatomic variation in cadaveric 21,22 and radiographic 5,8,13,20 studies. While this has most commonly been measured on plain radiographs, 13,19,20 our study used preoperative MRI scans to accurately determine the distance between the femoral insertion of the MPFL and the medial distal femoral physis with a novel, reproducible method with high interrater reliability (ICC = 0.854, P < .001). This is a consistent method that is based on the patient’s own anatomic landmarks. Our method allows for the creation of a more perfect lateral image, accounting for some of the rotational variability with lateral radiographs. Unlike plain radiographs and computed tomography scans, MRI does not use ionizing radiation, which is another important consideration in the pediatric population, particularly in the instability population, who may be subjected to multiple imaging studies during the clinical course of their condition.
Our study revealed the mean distance between the Schöttle point and the medial distal femoral physis to be 7.27 ± 1.78 mm distal to the physis. This location is similar to prior radiographic and cadaveric studies with different measurement methods. Using MRI, Greenrod et al 5 reported that the femoral origin of the MPFL was distal to the distal femoral physis in all patients by a mean 10 mm (range, 2-16 mm), while Kepler et al 8 cited this distance as 5 mm distal to the femoral growth plate (range, 7.5 mm proximal to 16 mm distal). Using the Schöttle method on lateral plain radiographs, Shea et al 20 found the MPFL origin to be on average between 2 and 5 mm proximal to the physis depending on sex, while Nelitz et al 13 cited the location as being 3.2 mm proximal to the physis. However, when considering the anteroposterior measurements, Nelitz et al 13 indicated the median origin of the MPFL to be 6.4 mm (range, 2.9-8.5 mm) distal to the physis in all patients.
Our measurement of the Schöttle point being on average 7.27 mm (range, 3.3-10.5 mm) distal to the physis, as well as the distances from the MRI studies of Kepler et al 8 and Greenrod et al, 5 were slightly greater in distance from the physis and more frequently distal to the physis as compared with the studies using plain radiographs. 13,20 The cadaveric study by Farrow et al 3 revealed a mean distance similar to that of our study, with the MPFL attachment being a mean 8.5 mm distal to the medial aspect of the distal femoral physis. The similarity in findings between the MRI studies and the cadaveric study could be related to the increased accuracy of identification of anatomic landmarks on MRI over plain radiographs. Furthermore, Huston et al 7 reported significant interobserver variance on both adult and pediatric lateral knee radiographs using the Schöttle technique, although it was greater for adult knees. This finding was potentially related to the perceived landmark variability on plain radiographs.
While our study demonstrated no association between age and the distance of the Schöttle point to the distal femoral physis, we did find that this distance was 1.31 mm closer/more proximal in females compared with males of the same age. While our numbers may have been too low to detect a significant difference, females generally reach skeletal maturity before males. Although a difference of 1.31 mm may not be clinically significant, the closer distance to the physis and MPFL origin for age-matched females could suggest that the distance between the MPFL origin and physis decreases or the MPFL origin becomes more proximal when approaching skeletal maturity. In a recent cadaveric study, Shea et al 21 reported a more proximal femoral origin footprint of the MPFL in older specimens, with the majority ≥7 years old having an MPFL origin just proximal to the physis (0.8 mm proximal to physis ≥7 years old vs 4.7 mm distal <7 years old). Similarly, in an MRI review of skeletally immature knee anatomy, Edmonds et al 1 indicated that the MPFL origin starts distal to the physis and moves proximally with age (ρ = 0.33, P < .001) such that, by age 7 years, it is found at or above the femoral physis. This, however, differs from the MRI findings of Greenrod et al, 5 who found a statistically significant increase in the MPFL-to-physis distance (approximately 0.6 mm more distal per year; r = 0.51, P < .001) with advancing age. More research is necessary to better define the relationship among sex, age, and the distance of the MPFL origin to the distal femoral physis.
Limitations
There are several limitations to this study. This was an observational case series; thus, we were not able to monitor the changes in the distance of the Schöttle point to physis within specific individuals over time. We also included more females (n = 21) than males (n = 13), but this is representative of the young patellar instability population. 4 Our measurements included the sagittal view only, which does not fully consider the distal femoral growth plate anatomy in all planes. However, as the lateral image is important for determining the start point to drill the femoral socket in preoperative planning and intraoperatively, we believe that this is the most important view to assess placement. This method will not replace the standard intraoperative method of using fluoroscopy to identify the Schöttle point, but it will provide individual approximation of the distance between the Schöttle point and the medial distal femoral physis with advanced imaging to aid in preoperative planning. Unique to this study, the use of the multiplanar reconstruction mode of the PACS to create a perfect lateral image of the knee was important for accurate and reproducible measurements, although not all imaging systems may have this feature.
Further limitations include our sample numbers, which may not have been high enough to detect clinically significant differences in comparison by age and sex. Additionally, we did not include patients younger than 10 years in this analysis, as our aim was to include the nonsyndromic traumatic sports-related dislocator population. In comparing our study with previous relevant studies, we found notable differences in study subjects, including cadaveric versus living patients, imaging modalities (radiograph, computed tomography, and MRI), and method of localization of MPFL insertion (anatomic dissection, radiological landmarks, and direct identification of ligament insertion on MRI), making direct comparison imperfect. However, we tried to call attention to and address these differences in the analysis of the current study with what is available in the literature. Finally, we note that while obtaining an anatomic radiographic starting point for graft insertion is important, graft isometry still must be assessed and fixation adjusted if the point is not found to be isometric.
Conclusion
For patients with open physes, the novel technique we describe can be utilized preoperatively to determine the appropriate safe distance to be drilling a socket. We found the Schöttle point to be distal to the physis in all patients, with skeletally immature females having a closer distance to the physis compared with age-matched males. As there is anatomic variation among all patients, this method can offer individualized assessment of the distance between the Schöttle point and the medial distal femoral physis to best re-create anatomy while protecting the physis.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: M.E.B. has received educational support from Smith & Nephew; S.R.B. has received educational support from Arthrex; and B.S.S. has received speaking fees and educational support from Arthrex and hospitality payments from DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hospital for Special Surgery Institutional Review Board (No. 2014-123).