
Abstract
Background:
Labral reconstruction has been described as a solution for the irreparable labrum. Initial techniques employed autografts, while more recent procedures have utilized allografts. No study, to our knowledge, has compared graft types.
Purpose:
To compare outcomes between patients who underwent primary labral reconstruction with a hamstring allograft versus hamstring autograft.
Hypothesis:
No significant differences in outcomes will be found between patients who underwent primary labral reconstruction with an allograft versus autograft.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data from September 2010 to March 2015 were reviewed. Inclusion criteria were primary hip arthroscopic surgery with labral reconstruction using either a hamstring allograft (ALLO group) or autograft (AUTO group), with minimum 2-year follow-up scores for the modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), Hip Outcome Score–Sports-Specific Subscale (HOS-SSS), and visual analog scale (VAS) for pain. Exclusion criteria were previous ipsilateral hip surgery, previous hip conditions, preoperative Tönnis osteoarthritis grade >1, and workers’ compensation claims. Significance was set at P = .05.
Results:
Twenty-nine patients (29 hips) were included (85.3% follow-up). There were 17 patients (17 hips) in the ALLO group and 12 patients (12 hips) in the AUTO group. All patient-reported outcome scores demonstrated significant improvements at latest follow-up except for the mHHS for the AUTO group (P = .064). Comparisons between the ALLO and AUTO groups at the preoperative and latest follow-up time points showed no significant differences (preoperative mean [range]: mHHS, 67.5 [33.0-100.0] and 65.8 [29.0-96.0], respectively [P = .826]; NAHS, 65.6 [26.3-92.5] and 58.5 [35.0-79.0], respectively [P = .322]; HOS-SSS, 43.7 [12.5-100.0] and 40.1 [19.0-78.0], respectively [P = .707]) (latest follow-up mean [range]: mHHS, 86.4 [56.0-100.0] and 81.4 [57.0-100.0], respectively [P = .46]; NAHS, 87.7 [60.0-100.0] and 82.4 [56.3-100.0], respectively [P = .396]; HOS-SSS, 81.7 [0.0-100.0] and 70.9 [27.8-100.0], respectively [P = .423]).
Conclusion:
Primary arthroscopic hip labral reconstruction yielded improvements in patient-reported outcome scores and high patient satisfaction. In this small series, no differences were found in clinical outcomes between hamstring allografts and autografts. Based on these results, hamstring allografts and autografts may be considered comparable graft choices for primary reconstruction. Because of the avoidance of donor site morbidity and the possible increase in patient satisfaction, allografts may be the preferred choice in a surgical setting when they are accessible.
Several studies have reported the importance of the labrum in the hip joint for regulating normal function by creating intra-articular fluid pressurization through the hip fluid seal. 2,16,27,34,39 Hip arthroscopic surgery for femoroacetabular impingement (FAI) with labral debridement or repair has resulted in significant improvements in long-term patient-reported outcomes (PROs). 24 Currently, there is a consensus that preserving the labrum is associated with improved results after hip preservation surgery. 13 –15,28,41
Several authors have reported good outcomes after arthroscopic labral repair, 19,32 with scientific evidence supporting histological healing. 32 Nevertheless, repair is not always possible. In young or active adults, irreparable tears and nonviable or calcified labra are usually common indications to proceed with more advanced techniques, such as labral reconstruction. 17 Domb et al 11 found that arthroscopic labral reconstruction is superior to labral resection for patients with irreparable labral tears. Multiple arthroscopic techniques have been described for labral reconstruction. § In a recent systematic review centered on labral reconstruction, no superiority was found among techniques. 2 The authors concluded that more research is needed regarding graft alternatives and their potential impact on PROs after labral reconstruction. Presently, there is a paucity of literature reporting and comparing graft choices for primary or revision labral reconstruction.
The purpose of this study was to compare clinical outcomes and survivorship between 2 groups of patients who underwent primary labral reconstruction with the hamstring tendon: 1 group with an allograft (ALLO group) and the second group with an autograft (AUTO group). We hypothesized that no significant differences in PRO scores or the survivorship rate would be found between these 2 groups.
Methods
Patient Selection Criteria
All patients participated in the American Hip Institute Hip Preservation Registry. While the present study represents a unique analysis, data on some patients in this study may have been reported in other studies. All data collection received institutional review board approval. Data were prospectively collected and retrospectively reviewed for all procedures performed between September 2010 and March 2015. The inclusion criteria were as follows: primary hip arthroscopic surgery with labral reconstruction using either a hamstring allograft or hamstring autograft as well as preoperative and minimum 2-year follow-up scores for the modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), Hip Outcome Score–Sports-Specific Subscale (HOS-SSS), and visual analog scale (VAS) for pain. The exclusion criteria were previous ipsilateral hip surgery, previous hip conditions (such as Legg-Calve-Perthes disease and slipped capital femoral epiphysis), rheumatological disease, preoperative Tönnis osteoarthritis grade >1, and workers’ compensation claims.
Clinical Evaluation
The senior surgeon (B.G.D.) performed a comprehensive physical examination on all patients, which included an assessment of range of motion and signs of FAI through lateral, anterior, and posterior impingement tests.
With the intention of assisting during surgical procedures, all patients underwent standard preoperative and postoperative radiographic imaging, which included a 45° modified Dunn view, anteroposterior pelvis view in both supine and upright positions, and false-profile view. The degree of osteoarthritis was assessed using the Tönnis scale. Other measurements, such as lateral center-edge angle, anterior center-edge angle, and alpha angle, were also calculated. The lateral center-edge angle and anterior center-edge angle were used to assess the degree of acetabular coverage, while alpha angles >60° indicated femoral cam-type deformities. In addition, all patients underwent magnetic resonance arthrography to confirm the diagnosis of a labral tear and to further evaluate the hip for extra- and intra-articular defects.
Indications for Hip Arthroscopic Surgery
Before being considered for surgery, all patients underwent conservative treatment for their hip pain, including rest, physical therapy, and nonsteroidal anti-inflammatory drugs. After at least 3 months of this conservative treatment, any patients with continued symptoms and evidence of FAI and labral tears were recommended for arthroscopic surgery by the senior author (B.G.D.).
Surgical Technique
Arthroscopic surgery was performed with patients in the modified supine position on a traction extension table (Smith & Nephew). Four portals were created: standard anterolateral, midanterior, distal anterolateral accessory, and posterolateral (Figure 1A). To access the hip joint, capsulotomy was performed using a beaver blade, cutting parallel to the labrum using direct visualization. To evaluate the labrum, intra-articular cartilage, and ligamentum teres, diagnostic arthroscopic surgery was performed. Acetabular chondral defects were graded using the acetabular labrum articular disruption (ALAD) 38 and Outerbridge classifications. 6 Femoral head cartilage defects were classified using the Outerbridge classification. Labral tears were classified using the Seldes classification, 36 and for the ligamentum teres, the Domb and Villar classifications were used. 4

(A) Right hip with the patient in a supine position; the patient’s head is to the left. Portal placement for segmental labral reconstruction. AL, anterolateral; DALA, distal anterolateral accessory; MA, midanterior; PL, posterolateral. (B) Both the semitendinosus allografts and autografts, G, were prepared in a doubled-over fashion with Krackow stitches to approximately 2 mm longer than the measured defect distance on each side.
When indicated, concomitant procedures were performed. When patients reported capsular laxity, reported microinstability, or were borderline dysplastic, capsular plication was performed at the conclusion of arthroscopic surgery. 8,12,15,18 Debridement was used to treat any fraying or tearing of the ligamentum teres. Pincer and cam morphologies were corrected using a bur under fluoroscopic guidance. Patients who reported painful internal snapping hip syndrome were treated with iliopsoas fractional lengthening. Iliopsoas fractional lengthening involved using a beaver blade to cut only the tendon portion of the iliopsoas at the muscle-tendon junction near the iliopectineal ridge at the level of the labrum. 15
Indications for Labral Reconstruction
The decision of whether to repair or reconstruct the labrum was made intraoperatively by the senior author. 12 Patients were considered for labral reconstruction if segmental labral defects and/or nonviable labral tissue were found during diagnostic arthroscopic surgery. For patients with insufficient labral tissue, reconstruction was identified as a more effective treatment than labral repair (Figure 2A). Arthroscopic reconstruction was performed using either a hamstring allograft or autograft. Originally, the senior author used hamstring autografts for this procedure. Subsequently, to decrease the risk of donor site morbidity, the reconstruction protocol changed to hamstring allografts, unless the patient specifically requested otherwise. 35 The portion of the diseased labrum that was nonfunctioning was debrided with a 5-mm shaver. The defect size was determined using a measuring probe from the labral repair/reconstruction kit (Arthrex) (Figure 2B).

Segmental labral reconstruction in the setting of an irreparable labral tear. Right hip with the patient in a supine position and viewing from the anterolateral portal with a 70° arthroscope. Before reconstruction: (A) perspective showing the labral tear from the 12-o’clock to 2-o’clock position and (B) measurement of the defect. After reconstruction: (C) perspective from the 12-o’clock to 3-o’clock position and (D) restoration of the suction seal. A, acetabulum (segmental defect); C, capsule; F, femoral head; L, irreparable labral tear; LR, labrum reconstructed; SS, suction seal.
Both the semitendinosus allografts and autografts were prepared in a doubled-over fashion with Krackow stitches to approximately 2 mm longer than the measured defect distance on each side (Figure 1B). At the anterior edge of the segmental loss of the labrum, the anterior portion of the graft was anchored using a 2.9-mm PushLock anchor (Arthrex). The remainder of the graft was affixed with 3.0-mm Knotless SutureTak anchors (Arthrex) or 2.9-mm PushLock anchors 36 (Figure 2, C and D; also see the Video Supplement).
Rehabilitation Protocol
After labral reconstruction, patients used crutches with partial weightbearing (20 lb [9 kg]) and wore a hip brace (DonJoy X-Act ROM hip brace; DJO Global) for 6 weeks. This brace was used to limit hip flexion to 90° and extension to 0°. Physical therapy began 6 weeks after surgery. To restore each patient’s strength and range of motion, patients were also instructed to begin using a stationary bicycle or continuous passive motion machine immediately after surgery.
Surgical Outcomes
To establish baseline mHHS, NAHS, HOS-SSS, and VAS pain scores, all patients completed preoperative questionnaires in the month before surgery. After surgery, these same outcome scores were collected, along with International Hip Outcome Tool–12 (iHOT-12), Veterans RAND 12-Item Health Survey (VR-12), and 12-Item Short Form Health Survey (SF-12) scores as well as patient satisfaction ratings (0-10) and any subsequent ipsilateral hip surgery.
Follow-up was achieved at 3 months postoperatively, at 1 year postoperatively, and annually thereafter. Follow-up was completed through encrypted emails, during clinical appointments, or through telephone interviews. Patients who did not have these outcome scores recorded at a minimum of 2 years after surgery were considered lost to follow-up.
The frequency of patients achieving the minimal clinically important difference (MCID) for the mHHS was calculated, defined as an improvement of 8 points. 22 The frequency of patients reaching the patient acceptable symptomatic state (PASS) for the mHHS was also calculated at a minimum 2-year follow-up, using the cutoff value of 74. 22,31
Revision surgery and survivorship rates were calculated for both groups. Patients who either reinjured their hips or who had continued symptoms after primary arthroscopic surgery were radiographically and clinically evaluated and offered conservative treatment before being recommended for revision surgery. Patients with unresolved symptoms and/or progression toward osteoarthritis were recommended for total hip arthroplasty (THA). Postoperative scores for patients who converted to THA were removed from the PRO analysis and discussed separately.
Statistical Analysis
An a priori power analysis was conducted to determine the number of patients needed to achieve 80% power. Based on a standard deviation of 10 (Cohen d = 3.0) and expected mean difference in the mHHS of 10, it was determined that 17 patients would be required for each group. 11 The F test and Shapiro-Wilk test were used to assess continuous data for equal variance and normality, respectively. Based on the results of these tests, continuous data were compared using the Student t test or Mann-Whitney U test. Categorical data were compared using the Fisher exact and chi-square tests. The threshold for significance was set to P = .05. All statistical analyses were performed using Excel (Microsoft) and its Real Statistics add-on package.
Results
During the study period, a total of 1689 primary arthroscopic procedures were performed by the senior author. Of these, 62 cases met the inclusion criteria. After exclusion criteria were applied, there were 28 patients in the ALLO group and 13 in the AUTO group. In the ALLO group, 21 patients (21 hips) were eligible for follow-up, and 17 patients (17 hips) had the necessary follow-up (81.0%). In the AUTO group, 13 patients (13 hips) were eligible for follow-up, and 12 patients (12 hips) had the required follow-up (92.3%) (Figure 3). Table 1 compares the demographics of the AUTO and ALLO groups. The ALLO group consisted of 9 (52.9%) male and 8 (47.1%) female patients, while the AUTO group consisted of 7 (58.3%) male and 5 (41.7%) female patients. No significant differences were found between groups in terms of age or body mass index.

Flowchart of patient selection.
Patient Demographics a

a Data are reported as mean ± SD (range) unless otherwise indicated.
In terms of preoperative radiographic measurements, the only measure that yielded a significant difference between groups was the alpha angle. The mean alpha angle for the ALLO group was 66.1° (range, 52°-89°), and the mean alpha angle for the AUTO group was 57.9° (range, 46°- 81°). Additionally, the ALLO group had a mean follow-up time of 29.9 months (range, 24.0-37.5 months), and the AUTO group had a mean follow-up time of 50.7 months (range, 25.7-72.0 months), which proved to be a significant difference (Table 1).
Intraoperative Findings
Table 2 illustrates the intraoperative findings documented during diagnostic arthroscopic surgery. No differences were noted between the 2 groups in terms of the ALAD grade, acetabular Outerbridge grade, Seldes-defined labral tears, or femoral head Outerbridge grade.
Intraoperative Findings Noted During Diagnostic Arthroscopic Surgery a

a Data are reported as n (%). ALAD, acetabular labrum articular disruption; LT, ligamentum teres.
Intraoperative Procedures
Table 3 shows the intraoperative procedures performed in the ALLO and AUTO groups. No patients underwent an isolated femoroplasty procedure, but 17 patients in the ALLO group and 10 patients in the AUTO group (83.3%) underwent combined acetabuloplasty and femoroplasty.
Intraoperative Procedures Performed During Hip Arthroscopic Surgery a

a Data are reported as n (%). All patients underwent labral reconstruction.
Outcome Scores
Differences in outcome scores from preoperative to latest follow-up were compared between the ALLO and AUTO groups (Table 4 and Figures 4 and 5). There were no differences between the ALLO and AUTO groups in outcome scores, but there was a significant between-group difference in patient satisfaction (8.8 vs 6.6, respectively; P = .03).
Preoperative and Follow-up Outcome Scores a

a Data are reported as mean ± SD (range). HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; NA, not applicable; NAHS, Non-Arthritic Hip Score; VAS, visual analog scale.
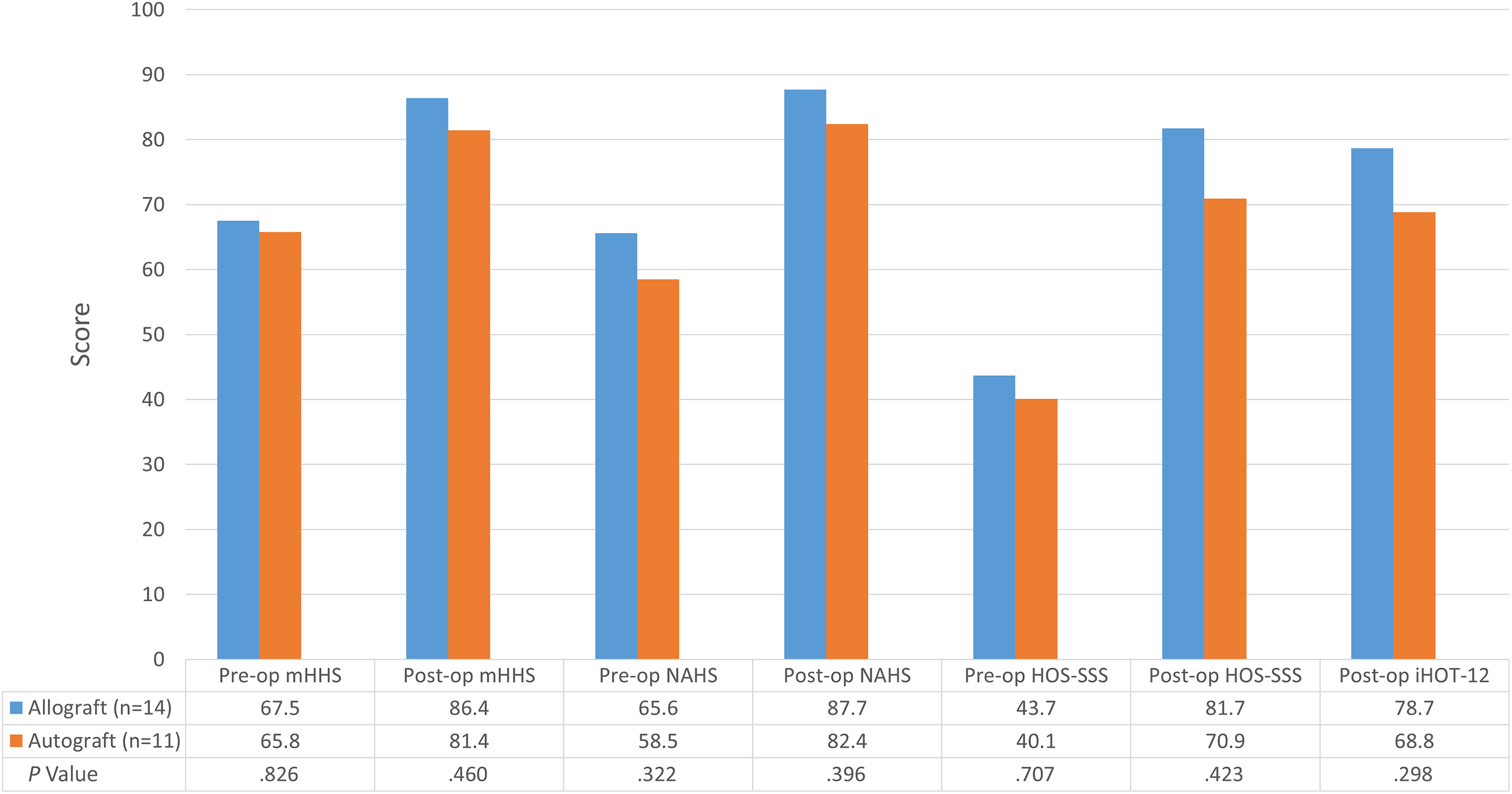
Preoperative and follow-up patient-reported outcome scores for hamstring allograft and autograft groups. Scores are reported as means. HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score.

Preoperative and follow-up visual analog scale (VAS) for pain scores and patient satisfaction scores for hamstring allograft and autograft groups. Scores are reported as means. Asterisk indicates statistical significance.
Table 5 and Figure 6 detail the comparison between the preoperative and latest follow-up time points within each group. Patients in both groups saw significant improvements on all outcome scores at latest follow-up, with the exception of the mHHS for the AUTO group (Table 5).
Improvements in Patient-Reported Outcome Scores at Latest Follow-up a

a Data are reported as mean ± SD (range). Comparisons were performed independently within groups. HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; NA, not applicable; NAHS, Non-Arthritic Hip Score; VAS, visual analog scale.

Improvement between preoperative and follow-up patient-reported outcome scores in the hamstring allograft and autograft groups. HOS-SSS, Hip Outcome Score–Sports-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score.
Ten patients (71.4%) in the ALLO group met the PASS for the mHHS (≥74) compared with 8 patients (72.7%) in the AUTO group (P > .99). In addition, the mean change in the mHHS score was 17.7 in the ALLO group and 15.6 in the AUTO group. In the ALLO group, 9 (64.3%) patients achieved the MCID, which was not significantly different (P > .99) from 8 (72.7%) patients in the AUTO group.
Future Revision and Conversion to THA
The rates of secondary arthroscopic surgery for each group are summarized in Table 6. There were no significant differences in the frequency of secondary arthroscopic surgery, in the duration of time to revision, or in the survivorship rate between the ALLO and AUTO groups.
Revision and Conversion to THA a

a NA, not applicable; THA, total hip arthroplasty.
Postoperative Complications
The overall complication rate was 21.4% (3 patients) in the ALLO group and 0.0% in the AUTO group, which was not a statistically significant difference. The 3 complications in the ALLO group included 2 cases of numbness down the leg and 1 case of unusual swelling.
Discussion
The current study found no significant differences in PRO scores between patients who underwent labral reconstruction using an allograft and autograft at 2-year follow-up after primary arthroscopic surgery.
In a recent systematic review, Ayeni et al 2 concluded that labral reconstruction is a new technique that shows short-term improvement in PRO and functional scores postoperatively. While the outcomes were similar to those in our study, the authors included revision surgery and did not compare semitendinosus allografts and autografts in their review. They also concluded that more research is necessary to determine whether graft choice plays a contributing role in patient outcomes after labral reconstruction.
There is a paucity of literature comparing patient outcomes between allografts and autografts for labral reconstruction in primary or revision hip arthroscopic surgery. In an in vitro study, labral reconstruction using an iliotibial band autograft and semitendinosus allograft was performed in cadaveric models; the researchers found no significant differences between graft types with respect to the contact area, contact pressure, or peak force in either 20° of extension or 60° of flexion. 21 However, given that this was a cadaveric model, clinical significance is hard to extrapolate from those results.
Several labral reconstruction techniques using different graft options have been published. ∥ All of these studies showed improvement in PROs at short-term follow-up. Geyer et al 17 published one of the largest series of labral reconstruction using iliotibial autografts in 75 patients. This study reported improvements in the mHHS of 24.1 points. 17 In a more recent study, White et al 40 published outcomes after labral reconstruction using allografts in 142 patients (156 hips) with a minimum 2-year follow-up. They also reported an improvement in the mHHS of 34 points and an overall patient satisfaction rating of 9 of 10. 40 These results are similar to our findings, as we also observed nonsignificantly higher PRO scores in the ALLO group, even though our data only included primary arthroscopic surgery. However, more research is needed before drawing conclusions on this matter.
Although donor site morbidity that results from hamstring autograft harvesting has been seen in anterior cruciate ligament reconstruction, in general, these cases appear to be minimal for labral reconstruction. 10,20 Neither donor site morbidity nor minimal graft preparation time has been cited as a potential advantage for the use of semitendinosus allografts over autografts for labral reconstruction. 23 Possible disadvantages of allograft use are disease transmission and delayed graft incorporation. 3 Moya Gómez et al 26 reported evidence of vascular ingrowth in all layers of the peroneus brevis allograft 8 weeks postoperatively, with cellular migration represented mainly by mature fibroblasts. While our study could not establish a clear preferred graft choice in terms of clinical outcomes, there was no known incidence of disease transmission, and patients in the ALLO group avoided any possibility of donor site morbidity. However, the mean patient satisfaction rating was significantly higher for the ALLO group, which might be related to the lack of donor site morbidity. Combined with the benefit of avoiding donor site morbidity and the comparable clinical outcomes, this improved patient satisfaction may suggest that an allograft is the preferred hamstring graft choice. Nevertheless, allograft cost (an average of US$850 from our sources) and availability are important variables that must be recognized by the surgeon in the decision-making progress. The present study did not evaluate the cost-effectiveness of using allografts.
Conversion to THA after labral reconstruction has been published by some authors, including the senior author. 7 Boykin et al 5 and Geyer et al 17 reported rates of conversion to THA of 9.5% and 23.7%, respectively. Both of these studies included revision surgery and made use of iliotibial band autografts. While these findings are similar to our results (see Table 6), more research is needed to compare the difference in conversion rates between primary and revision labral reconstruction. 5,17
In the current study, while age was not significantly different between the 2 groups, patients were not matched, and future research is needed to determine the role that age plays in choosing between hamstring allografts and autografts.
There are several strengths of this study, including the use of multiple validated functional hip outcome measures to evaluate patients undergoing primary hip arthroscopic labral reconstruction at a minimum 2-year follow-up. By incorporating both the PASS and MCID in our analysis, this study provided clinical significance to our findings. Additionally, even though the 2 patient groups (AUTO and ALLO) were not matched, there were no statistically significant differences between the groups in sex, age, or body mass index. Furthermore, this study is one of the first to compare hamstring autografts and allografts for patients undergoing primary labral reconstruction.
Limitations
There are also limitations to our study, which must be acknowledged. First, this study was nonrandomized and retrospective in design, and the AUTO group had a significantly longer follow-up time than the ALLO group. Second, the small sample may limit generalizability. The fact that all analyzed cases are from a single high-volume hip preservation surgeon may further limit generalizability. Third, the preoperative alpha angle was significantly different between groups, which is a potential confounding factor. Fourth, a longer follow-up is still needed to determine the durability of our findings. Fifth, subjective or objective measurements of hamstring donor site morbidity were not taken into account. Sixth, the senior author transitioned from autografts to allografts during the study period, so the ALLO group underwent surgery further out on the “learning curve.” Finally, the ALLO and AUTO groups were not matched based on the other procedures performed; thus, these associated procedures may influence the results.
Conclusion
Primary arthroscopic hip labral reconstruction yielded improvements in PROs and high patient satisfaction. In this small series, no differences were found in clinical outcomes between hamstring allografts and autografts. Based on these results, hamstring allografts and autografts may be considered comparable graft choices for primary reconstruction. Because of the avoidance of donor site morbidity and possible higher patient satisfaction, allografts may be the preferred choice in a surgical setting when they are accessible.
A Video Supplement for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/2325967119833715
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.C.L. has received research support from Arthrex, educational support from Medwest and Smith & Nephew, and hospitality payments from Stryker. B.G.D. has ownership interests in Hinsdale Orthopaedics, the American Hip Institute, SCD#3, North Shore Surgical Suites, and Munster Specialty Surgery Center; has received research support from Arthrex, ATI, the Kauffman Foundation, and Pacira Pharmaceuticals; has received consulting fees from Adventist Hinsdale Hospital, Arthrex, MAKO Surgical, Medacta, Pacira Pharmaceuticals, and Stryker; has received educational support from Arthrex, Breg, and Medwest; has received speaking fees from Arthrex and Pacira Pharmaceuticals; and receives royalties from Arthrex, DJO Global, MAKO Surgical, Stryker, and Orthomerica. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Advocate Health Care Institutional Review Board (No. 5276).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.