
Abstract
Background:
Investigations specifically delineating the safest and most efficacious components of physical therapy after ulnar collateral ligament (UCL) reconstruction of the elbow are lacking. As such, while a number of recommendations regarding postoperative therapy have been published, no validated rehabilitation guidelines currently exist.
Purpose:
To assess the variability of rehabilitation protocols utilized by orthopaedic residency programs in the United States (US) and those described in the scientific literature.
Study Design:
Cross-sectional study.
Methods:
Online UCL reconstruction rehabilitation protocols from US orthopaedic programs and from the scientific literature were reviewed. A comprehensive scoring rubric was developed to assess each protocol for the presence of various rehabilitation components as well as the timing of their introduction.
Results:
Overall, 22 protocols (14%) from 155 US Electronic Residency Application Service (ERAS) orthopaedic programs and 8 protocols published in the scientific literature detailing UCL reconstruction postoperative rehabilitation were identified and reviewed. After reconstruction, the majority of ERAS and review article protocols (77% and 88%, respectively) advised immediate splinting at 90° of elbow flexion. The mean time to splint discontinuation across all protocols was 2.0 weeks (range, 1-3 weeks). There was considerable variability in elbow range of motion recommendations; however, most protocols detailed goals for full extension and full flexion (>130°) at a mean 5.3 weeks (range, 4-6 weeks) and 5.5 weeks (range, 4-6 weeks), respectively. Significant diversity in the inclusion and timing of strengthening, proprioceptive, and throwing exercises was also apparent. Thirteen ERAS (59%) and 7 review article (88%) protocols specifically mentioned return to competition as an endpoint. ERAS protocols permitted return to competition significantly earlier than review article protocols (29.6 vs 39.0 weeks, respectively; P = .042).
Conclusion:
There is notable variability in both the composition and timing of rehabilitation components across a small number of protocols available online. While our understanding of postoperative rehabilitation for UCL reconstruction evolves, outcome-based studies focused on identifying clinically beneficial modalities and metrics are necessary to enable meaningful standardization.
The ulnar collateral ligament (UCL) serves as the primary static restraint to valgus force at the elbow. An injury to the UCL can be particularly devastating for high-performance overhead athletes and continues, unfortunately, to become increasingly common. 9 Injured athletes may have severe limitations in throwing ability, medial elbow pain, decreased muscular strength, and instability. Additionally, before Dr Frank Jobe’s first description of UCL reconstruction to restore valgus stability to the elbow, this was considered a career-ending injury for throwers. 10 Since that time however, there have been numerous advances in surgical techniques, such that most throwers have excellent outcomes with UCL reconstruction. 7 Of the various techniques developed, systematic reviews have suggested that the docking technique may result in lower complications and have the best rate of return to play compared with other surgical procedures. 2
While the surgical techniques to address a ruptured UCL have progressed substantially, there remain a number of other significant factors for successful UCL reconstruction, including appropriate preoperative indications, patient selection, intraoperative decision making, the addressing of concomitant abnormalities (eg, ulnar neuropathy or valgus extension overload), and postoperative rehabilitation. Although the majority of these factors have been extensively studied, the ideal postoperative rehabilitation regimen has yet to be established. The significance of an appropriate rehabilitation regimen in safely restoring motion, strength, conditioning, and normal throwing in a timely and efficient manner cannot be overemphasized. As such, rehabilitation after UCL reconstruction has been a topic of investigation in recent years. 5,6,18,20,21
We have previously assessed the quality and variability of postoperative rehabilitation protocols for anterior cruciate ligament reconstruction, 13 proximal hamstring repair, 11 and Achilles tendon repair 12 and found significant diversity among recommendations, many of which were not supported by evidence. Given that multiple orthopaedic studies have found a correlation between improved clinical outcomes and standardization of clinical care, 1,8 an initial investigation of the variability across UCL rehabilitation protocols is warranted. The purpose of the current study was to assess the variability of UCL reconstruction postoperative rehabilitation protocols published online by Electronic Residency Application Service (ERAS) orthopaedic programs as well as those identified in the scientific literature. We hypothesized that there would be significant variability among all identified protocols as well as between ERAS and review article protocols.
Methods
This investigation reviewed publicly available rehabilitation protocols from ERAS orthopaedic programs and from the published literature to provide 2 cohorts for comparison. This methodology is in line with prior rehabilitation-focused studies. 11 –13 For ERAS protocols, a general web-based search (www.Google.com) was performed using the following search term: “[Program/affiliate hospital/affiliate medical school name] UCL reconstruction rehabilitation protocol.” Protocols from the published literature that primarily focused on rehabilitation were selected using PubMed using the search term “UCL reconstruction rehabilitation protocols.” This search accounted for overlapping protocols, identifying those original studies in which protocols were first proposed. Protocols were excluded from the review if they were designed for pediatric patients, involved concomitant procedures, or lacked sufficient detail such as commencement time points for rehabilitation components.
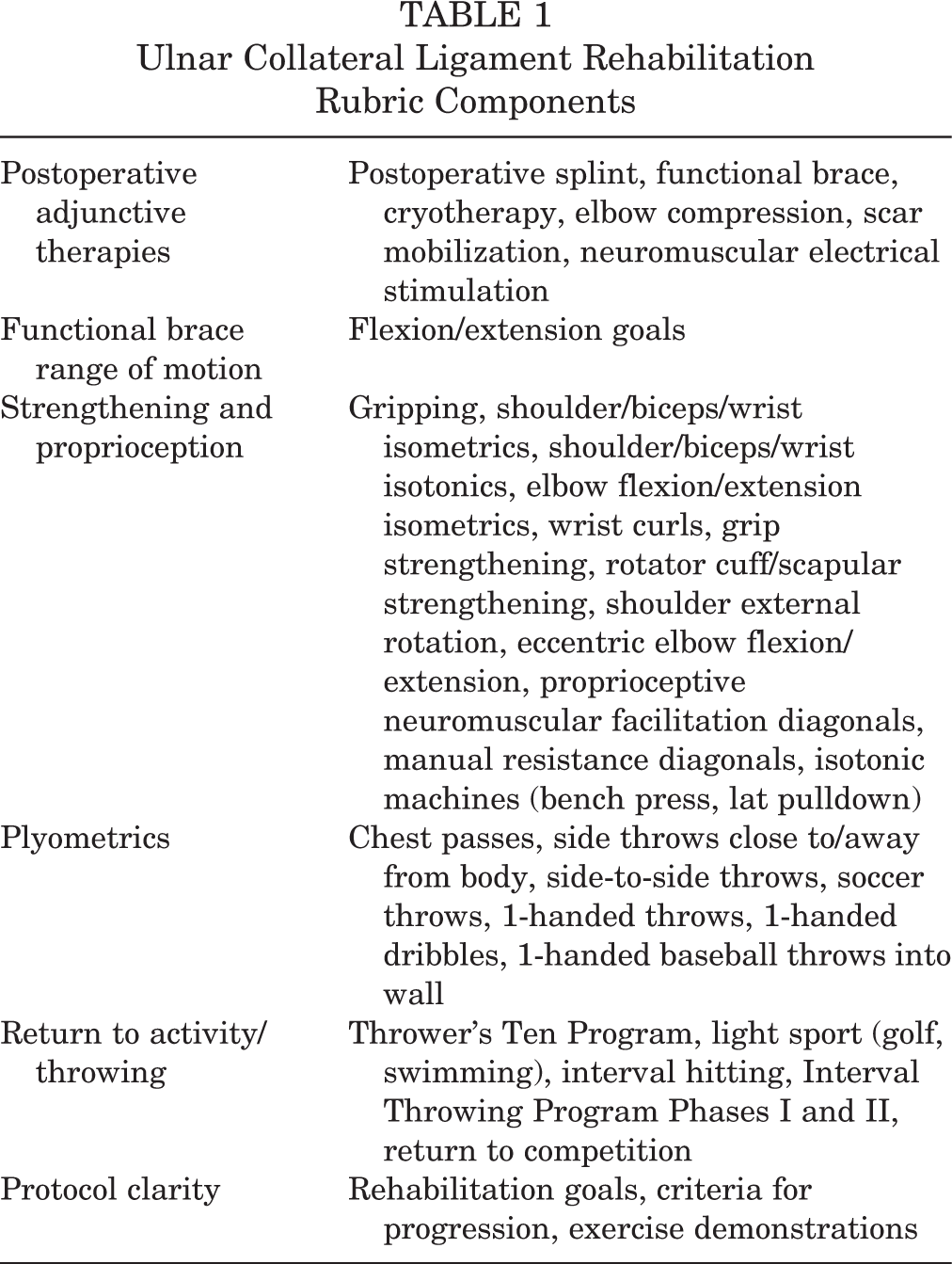
A custom scoring rubric was designed after a comprehensive review of available protocols. The rubric consisted of specific sections for metrics; binary coding was used to assess the inclusion of specific rehabilitation components, while numerical scoring was used to evaluate the range of commencement dates. The following broad categories were defined in the rubric: postoperative adjunctive therapies, functional brace range of motion, strengthening and proprioception, plyometrics, return to activity/throwing, and protocol clarity (Table 1).
Ulnar Collateral Ligament Rehabilitation Rubric Components
Results
A total of 155 ERAS orthopaedic programs were included for review; of these, 22 (14%) provided online rehabilitation protocols that met eligibility criteria. A total of 8 protocols were reviewed from the published literature, primarily publications with evidence levels 4 and 5 focusing on UCL rehabilitation. 5,6,15,16,18,19 Within the scientific literature, 1 study provided separate protocols for reconstruction using an autogenous graft versus the docking procedure. 6 A second investigation also outlined 2 protocols, both for reconstruction with a palmaris longus autograft. 15
Postoperative Adjunctive Therapy
Six types of postoperative adjunctive therapy were assessed (Figure 1): postoperative splinting, functional brace use, cryotherapy, elbow compression, scar mobilization, and neuromuscular electrical stimulation. The majority of ERAS and review article protocols (77% and 88%, respectively) recommended immediate postoperative splinting at 90° of elbow flexion. The mean time to splint discontinuation across all protocols was 2.0 weeks (range, 1-3 weeks). Afterward, functional braces were advised by 100% of ERAS protocols and 88% of review article protocols and were discontinued at a mean of 5.4 weeks (range, 4-6 weeks) and 5.8 weeks (range, 5-6 weeks), respectively. Over half of all protocols included cryotherapy (20/30; 67%) and elbow compression (16/30; 53%) in their regimens. Of note, 9 ERAS protocols recommended scar mobilization; however, this modality was not recommended in published studies. Only 3 total protocols (10%) recommended neuromuscular electrical stimulation as needed throughout the course of rehabilitation.
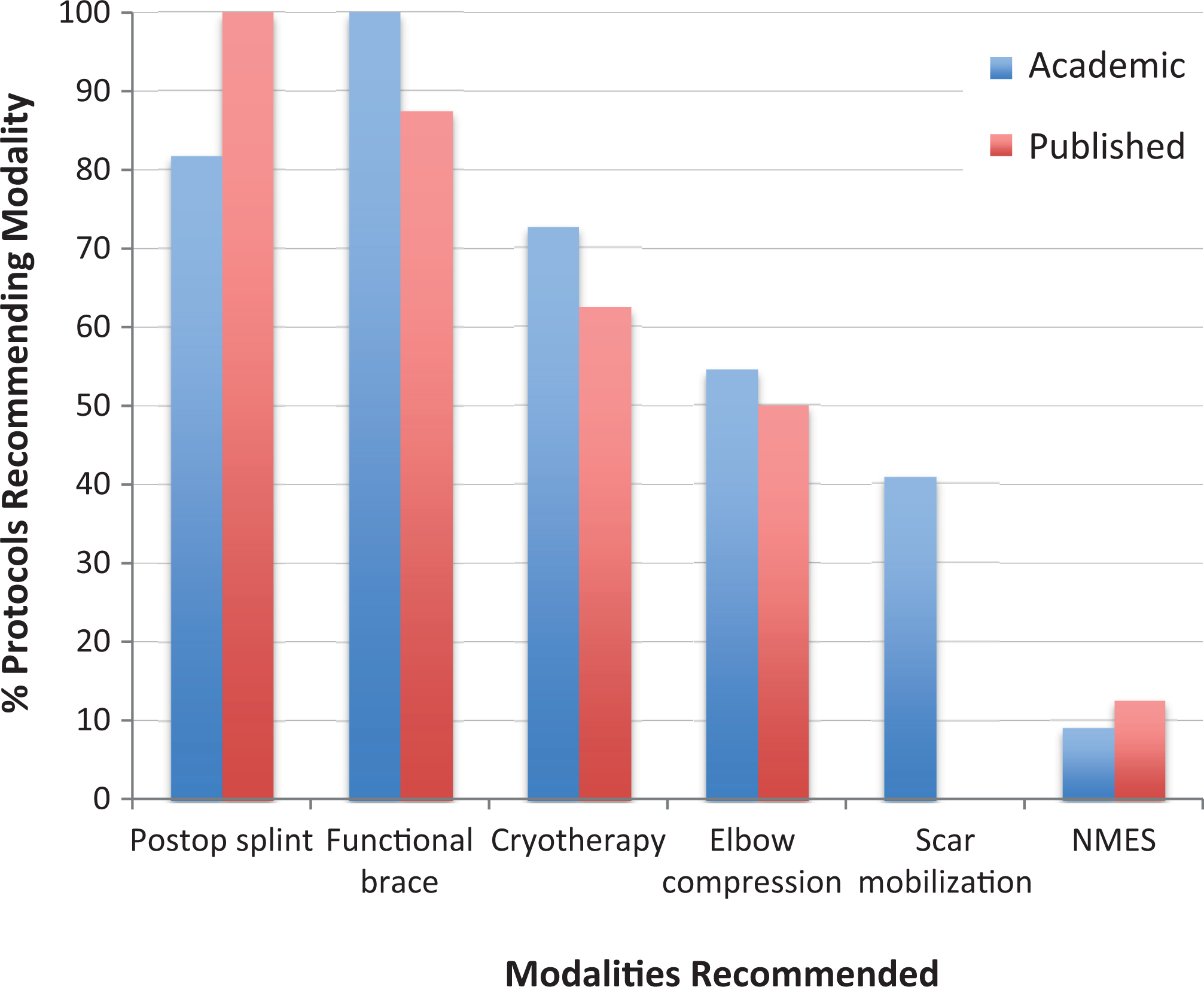
Variability in postoperative adjunctive therapies between rehabilitation protocols. While the majority of all protocols recommended immediate postoperative splinting, followed by functional bracing, scar mobilization was only recommended by ERAS protocols. ERAS, Electronic Residency Application Service; NMES, neuromuscular electrical stimulation.
Range of Motion
There was considerable variability in the inclusion and timing of specific range of motion limitations and goals. In progressing toward full extension, 30° and 15° flexion goals were recommended by 11 (50%) and 14 (64%) ERAS protocols at a mean of 1.6 weeks (range, 1-2 weeks) and 2.9 weeks (range, 2-3 weeks), respectively. In the published literature, flexion goals of 30° and 15° were advocated by 75% of protocols at a mean of 2.0 weeks and 3.3 weeks (range, 3-4 weeks), respectively. Across all protocols, 27 (90%) and 25 (83%) set goals of full extension and full flexion (>130°) to be achieved at a mean of 5.3 weeks (range, 4-6 weeks) and 5.5 weeks (range, 4-6 weeks), respectively. There were no significant variations in the timing of any range of motion goals between ERAS and review article protocols.
Strengthening and Proprioception
Twelve basic strengthening exercises were assessed in the rubric for UCL reconstruction rehabilitation protocols (Table 1). Across all protocols, 8 of the 12 exercises appeared in more than 50% of the protocols (Figure 2A). Among the most common strengthening exercises, gripping and shoulder isometrics without external rotation were routinely prescribed within the first postoperative week. However, a wide variation was found with regard to commencement dates for most of the remaining exercises (Figure 2B). The highest variability in start dates existed for rotator cuff/scapular strengthening (9-week range from the earliest recommended start date) as well as eccentric elbow flexion/extension exercises and proprioceptive neuromuscular facilitation diagonals (both with a 6-week range from an earliest allowable start date of 6 weeks). In comparing the initiation of various strengthening exercises between ERAS and review article protocols, significantly earlier mean start times were identified in ERAS protocols for isometric shoulder strengthening without external rotation (0.1 vs 1.4 weeks, respectively; P = .003), rotator cuff and scapular strengthening (3.9 vs 6.3 weeks, respectively; P = .004), external rotational shoulder strengthening (5.8 vs 6.8 weeks, respectively; P = .008), and proprioceptive neuromuscular facilitation (7.4 vs 10.0 weeks, respectively; P = .036).

(A) Strengthening and proprioceptive exercises. A significant variation was found between protocols from orthopaedic programs versus the published literature with regard to the types of exercises included in rehabilitation protocols. (B) A significant variation was also found with regard to recommended start times for strengthening exercises. The numbered circle within each range represents the mean of the data set. -ER, without external rotation; PNF, proprioceptive neuromuscular facilitation; RC, rotator cuff.
Plyometrics
Eight plyometric exercises for UCL reconstruction rehabilitation protocols were assessed (Table 1). None of the 8 appeared in more than 50% of the protocols (Figure 3A). Side throws were mentioned in 6 (27%) ERAS protocols but were not recommended in the published literature. Furthermore, soccer throws, included by 32% of ERAS protocols, were recommended by only 1 review article protocol. There was considerable variation in the timing of plyometric initiation, in particular with more advanced exercises. Across all protocols, 1-handed exercises demonstrated a 9-week range from the earliest recommended start date of 12 weeks (Figure 3B).

(A, B) Plyometric exercises. A significant variation was found between protocols from orthopaedic programs versus the published literature in the inclusion of exercises as well as recommended start times for exercises. The numbered circle within each range in (B) represents the mean of the data set.
Return to Activity/Throwing
Regarding return to basic throwing activities, the Interval Throwing Program Phase I was recommended by all protocols included in the study (Figure 4A). The Interval Throwing Program Phase II was incorporated by 41% of ERAS and 13% of review article protocols. The Thrower’s Ten Program was initiated among protocols at a mean start date of 7.2 weeks (range, 5-12 weeks), and the Interval Throwing Program Phases I and II were started at a mean of 16.3 weeks (range, 14-21 weeks) and 22.6 weeks (range, 22-28 weeks), respectively (Figure 4B). Light sport, consisting of golf and swimming, was recommended by 73% of ERAS protocols and by 50% of review article protocols; however, there was substantial variability as to when these activities were initiated. Similarly, there was a 10-week range across protocols recommending interval hitting. There were no significant differences in the timing of any of the above activities between ERAS and review article protocols.

(A) Return to athletic activity/throwing and (B) start dates. The numbered circle within each range in (B) represents the mean of the data set.
Thirteen ERAS protocols (59%) and 7 review article protocols (88%) specifically mentioned return to competition as an endpoint for UCL rehabilitation (Figure 4A). For ERAS protocols, this occurred at a mean of 29.6 weeks (range, 22-52 weeks). For protocols described in the published literature, return to competition was advised at a mean of 39.0 weeks (range, 26-52 weeks; P = .042).
Protocol Clarity
Examining protocol clarity consisted of assessing guidelines for the explicit mention of rehabilitation goals, criteria for progression, and accompanying demonstrations of the proper exercise form. While there were several notable exceptions, the vast majority of ERAS protocols (17/22; 78%) did not list rehabilitation goals and criteria for progression. Furthermore, only 1 ERAS protocol included drawings of recommended exercises. In contrast, 88% of review article protocols listed goals and criteria for progression, and 63% included images and/or photographs of exercises.
Discussion
The results of this study reveal that a small minority of ERAS orthopaedic programs (14%) publishes UCL reconstruction rehabilitation protocols online. Furthermore, few scientific investigations specifically focused on UCL rehabilitation have been published, and those published primarily consist of expert opinion. 5,6,15,16,18,21 Across available protocols, there is significant variability with regard to both the inclusion of physical therapy modalities and the timing of rehabilitation milestones. Such findings highlight the need for outcome-based research and represent an opportunity to improve care through increased standardization. Process standardization has been shown to result in improved functional outcomes and more efficient use of resources in total joint arthroplasty. 1,8 In this way, we felt it important to evaluate and compare accessible online ERAS protocols with studies dedicated to examining concepts in UCL rehabilitation.
From our investigation, one of the most consistent aspects of UCL rehabilitation was initial immobilization in the form of splinting, followed by early range of motion in a functional brace to prevent scar tissue formation and contracture. Such practice is in accordance with studies emphasizing the re-establishment of full elbow extension in the initial phase of rehabilitation. 3,16 –18
In contrast to this consistency, substantial variability was observed across recommended strengthening exercises, plyometric modalities, and progression to return to activity and throwing. In 1993, Wilk et al 18 highlighted the importance of performing specific strengthening, neuromuscular control, and plyometric exercises throughout the course of physical therapy to develop the endurance and stamina needed to return to throwing activities. In this effort, the Thrower’s Ten Program was developed as the culmination of several electromyographic and biomechanical studies to prepare the throwing musculature for progression to the Interval Throwing Program. This program, consisting of Phase I, long toss, and Phase II, off the mound, was first described by Wilk et al 19 to provide a guide for effort progression, pitches thrown, and graduation to game situations. Interestingly, in the present study, Phase I of the Interval Throwing Program was recommended by 100% of protocols with a 7-week range in the mean start date; however, only 41% of ERAS and 13% of review article protocols subsequently implemented Phase II.
With respect to return to competitive throwing, a review of the published protocols, including 1 current concepts study citing the follow-up of 1294 athletes treated with a modified Jobe procedure, 6 showed a mean return of 39.0 weeks, nearly 10 weeks longer than the mean allowable time frame of the ERAS protocol cohort. In considering the amount of time that a thrower is out of play, this is certainly not an insignificant number. Accelerated rehabilitation recommendations were also seen with regard to the timing of various strengthening modalities when comparing ERAS with review article protocols. Specifically, the initiation of shoulder strengthening without external rotation, rotator cuff and scapular strengthening, external rotational shoulder strengthening, and proprioceptive neuromuscular facilitation all occurred earlier in ERAS protocols. Whether such differences are clinically significant in promoting the return of proper throwing mechanics or return to play remains to be determined.
After a systematic review of the included physical therapy protocols, the importance of protocol clarity and patient understanding became apparent. To this end, the incorporation of explicit expectations as well as drawings, photographs, and accompanying videos depicting the proper form are invaluable. Unfortunately, the vast majority of publicly available ERAS protocols lacked this information. As patients are increasingly using the internet to independently access health care information, 14 clear, comprehensible online resources are critical to ensuring safe and effective patient care.
The present investigation has several limitations. To date, there is a paucity of outcome-based studies focused specifically on UCL rehabilitation. As such, protocol comparisons in this study were made without a guiding, evidence-based standard of care. In this effort, although 155 total ERAS programs were considered, only 14% of programs provided protocols satisfying our eligibility criteria. Based on our initial searches, this number represents a minority of all online UCL reconstruction rehabilitation protocols. Many physicians and practice groups have personalized websites where their particular protocols can be found. Alternatively, many well-established UCL centers do not provide online access to rehabilitation protocols. However, our methodology is in accordance with similar rehabilitation studies. 4,11 –13 Second, it is common practice for orthopaedic surgeons to provide protocols directly to patients or to physical therapists. Such protocols are more likely to be individualized, incorporating preoperative considerations and intraoperative decisions. While this individualization is an important component in patient care, it excludes such protocols from group analysis. Third, while rehabilitation protocols in this study were limited to isolated UCL reconstruction, the protocols rarely specified the surgical technique. Differences in surgical fixation may warrant unique rehabilitation considerations, as suggested in a recent review of Jobe, docking, and DANE procedures. 20 Furthermore, it was clear from our work that protocols have changed over time; however, for the sake of group analysis and establishing a review article cohort, such differences were overlooked. Finally, as noted above, certain rehabilitation protocols were clearly more thorough than others, the most comprehensive of which cited published work. Such protocols may be more representative of best practice but were weighted equally in our data analysis.
Conclusion
This investigation comparing online ERAS UCL physical therapy protocols with protocols described in the published literature highlights the variability in the composition and timing of rehabilitation guidelines. Furthermore, there was a lack of patient-directed readership. While our understanding of UCL rehabilitation evolves, the need for outcome-based rehabilitation studies with the goal of identifying clinically beneficial metrics and modalities is clear. Ultimately, this will permit evidence-based standardization of protocols and will promote a more navigable and safe recovery course for patients.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: E.C.M. has received educational support from Pinnacle and Smith & Nephew, consulting fees from Smith & Nephew, and hospitality payments from Smith & Nephew and Stryker. C.S.A. has received consulting fees from Arthrex, speaking fees from Arthrex, royalties from Arthrex, and hospitality payments from DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.