
Abstract
Background:
Repetitive loading and shear stress across the proximal femur account for the high prevalence of cam deformity in athletes.
Purpose:
To systematically review the literature to identify the reported number, age, mean alpha angle measurements, and differences between male and female athletes with radiographic cam deformity based on sport.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was conducted of studies in the literature between January 1990 and March 2018 that reported on athletes with radiographic cam deformity based on sport. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed, and PubMed, Biosis Previews, SPORTDiscus, PEDro, and EMBASE databases were used. Inclusion criteria included studies documenting radiographic cam deformity based on alpha angle measurements categorized according to the athlete’s primary sport and according to sex. Exclusion criteria were (1) studies not documenting primary sport, (2) studies not reporting total number of athletes with radiographic cam deformity, and (3) studies not separating cam deformity based on sex or using alpha angle measurements. Statistical analysis was used to compare mean reported age and alpha angle measurements between males and females.
Results:
A total of 28 studies consisting of 1160 male and 53 female athletes with radiographic cam deformity were identified. Cam lesions were most commonly reported in soccer athletes among both males and females, followed by hockey and American football. Male athletes had significantly higher mean alpha angle measurements (59.9° ± 5.5°) compared with female athletes (48.3° ± 6.9°) (P = .001). No significant difference in age was appreciated between males (21.1 ± 4.0 years) and females (21.7 ± 3.0 years) (P = .62).
Conclusion:
Radiographic cam deformity is most commonly reported in athletes participating in soccer and hockey. Males possessed significantly greater mean alpha angle measurements compared with females, whereas no significant difference in mean age at the time of diagnosis was appreciated between sexes.
Repetitive loading and shear stresses placed across the proximal femur in athletes are associated with the development of structural hip abnormalities, specifically cam-type impingement deformities. 4,10,12,52,66 Cam formation has been proposed as a structural adaptation to rigorous high-impact sporting activities in adolescence during skeletal growth, when the skeleton is most susceptible to mechanical loading. 49,50 Compared with nonathlete controls, both symptomatic and nonsymptomatic athletes have been shown to possess a significantly higher prevalence of clinical and radiographic cam deformity. 2,44,66 Young athletes with cam deformities are at high risk for labral and articular cartilage damage, potentially diminishing performance and participation from sport. 22,35,59,61
Improvements in the diagnosis and recognition of anatomic abnormalities of the hip associated with femoroacetabular impingement (FAI) syndrome, coupled with increased reporting in the literature over the past decade, have significantly improved awareness of cam impingement in the differential of youth and adult athletes presenting with hip and groin pain. 42,65 Despite the short-term implications associated with cam deformity, studies have shown an increasingly recognized role of cam impingement as a pathologic factor in the early development of hip osteoarthritis (OA). 3,5,6,8,26,57,75,76 Compared with nonathlete controls, athletes with cam lesions have been found to possess a 3 to 8.5 times higher prevalence of developing signs and symptoms of hip OA. 66 As such, identification of risk factors for the development of cam deformity, particularly factors associated with sport participation, is essential to guide implementation of appropriate preventive strategies to diminish hip and groin pain in the setting of cam impingement, while preventing further intra-articular damage and osteoarthritic changes. 53
The purpose of this investigation was to systematically review the literature to determine the reported number of radiographic cam deformities based on sport. Specifically, we sought to define (1) the reported number and age of athletes with radiographic cam deformity based on sport, (2) mean reported alpha angle measurements based on sport, and (3) differences in sport participation, reported number, athlete age, and alpha angle measurements between males and females. Drawing on prior literature, we hypothesized that radiographic cam deformities would be reported more commonly in male athletes participating in contact sports. 7,28,53,55,60
Methods
A systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, and a PRISMA checklist was used. 47 All literature related to athletes diagnosed with cam impingement deformity, as published from January 1990 to October 2018, was identified. Two authors (D.M.K., M.A.G.) independently conducted the search in October 2018 using the following databases: PubMed, Biosis Previews, SPORTDiscus, PEDro, and EMBASE. Each search included the following terms: sport AND athlete AND cam AND FAI AND impingement AND deformity.
Inclusion criteria consisted of articles in the English language or with English translations, studies of athletes with radiographic evidence of cam deformity based on alpha angle measurements, and articles reporting primary sport and athlete sex. Excluded were non–English language studies, studies reporting cam deformity in athletes without specific mention of primary sport, and studies not documenting total number of athletes with cam deformity, not separating cam occurrence based on sex, and not reporting imaging modality used to measure alpha angle.
A total of 98 citations were identified after the database search. The search process is shown in the flow diagram (Figure 1). After title and abstract assessment, 50 full-text articles were selected for further evaluation. To ensure that all available studies were identified, references within each of the included articles were cross-referenced for inclusion. Studies were grouped based on the primary sport reported.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of study.
Statistical analysis was performed to compare mean number of athletes diagnosed with radiographic cam deformity based on primary sport recorded. When provided, mean alpha angle and athlete ages were calculated and compared based on sex by use of an unpaired Student t test. All statistical analyses were performed using SPSS software (v 23; IBM).
Results
Of the 50 studies identified for full-text review following the initial literature review, 10 studies were excluded because athletes were not categorized based on single primary sport. A further 12 studies were excluded for the following reasons: 5 studies because of failure to separate cam deformity number based on sex, 4 studies because the overall number of athletes diagnosed with cam deformity was not reported, 2 studies because the number of hips with cam deformity was reported without mention of the number of athletes, and 1 study because it failed to report on the imaging modality used to measure alpha angle. Following application of the aforementioned inclusion and exclusion criteria, a total of 28 studies were identified for analysis in the review.
From the 28 studies meeting inclusion/exclusion criteria, 1160 male athletes and 53 female athletes with radiographic cam deformity were identified (Table 1). Soccer ¶ was the sport with the greatest reported number of affected male and female athletes, followed by hockey, 10,11,24,44,60,64,67,68 American football, 35,36,43,54 ballet/dance, 21,23,29 and track and field 37,40 (Table 2). Male athletes were more commonly reported than females in all sports except for ballet/dance, track and field, and volleyball. Overall, male athletes had a significantly higher alpha angle measurement (59.9° ± 5.5°) at the time of diagnosis compared with female athletes (48.3° ± 6.9°) (P = .001). Measurements were most commonly performed on radiographs, using anteroposterior (AP) and frog-leg lateral projections. Mean reported age at the time of diagnosis was 21.1 ± 4.0 years in male athletes and 21.7 ± 3.0 years in female athletes, although athlete age was not reported in a total of 4 studies. 24,32,43,68 No significant difference was appreciated based on age at the time of diagnosis between male and female athletes (P = .62).
Overview of Studies Included in Review a
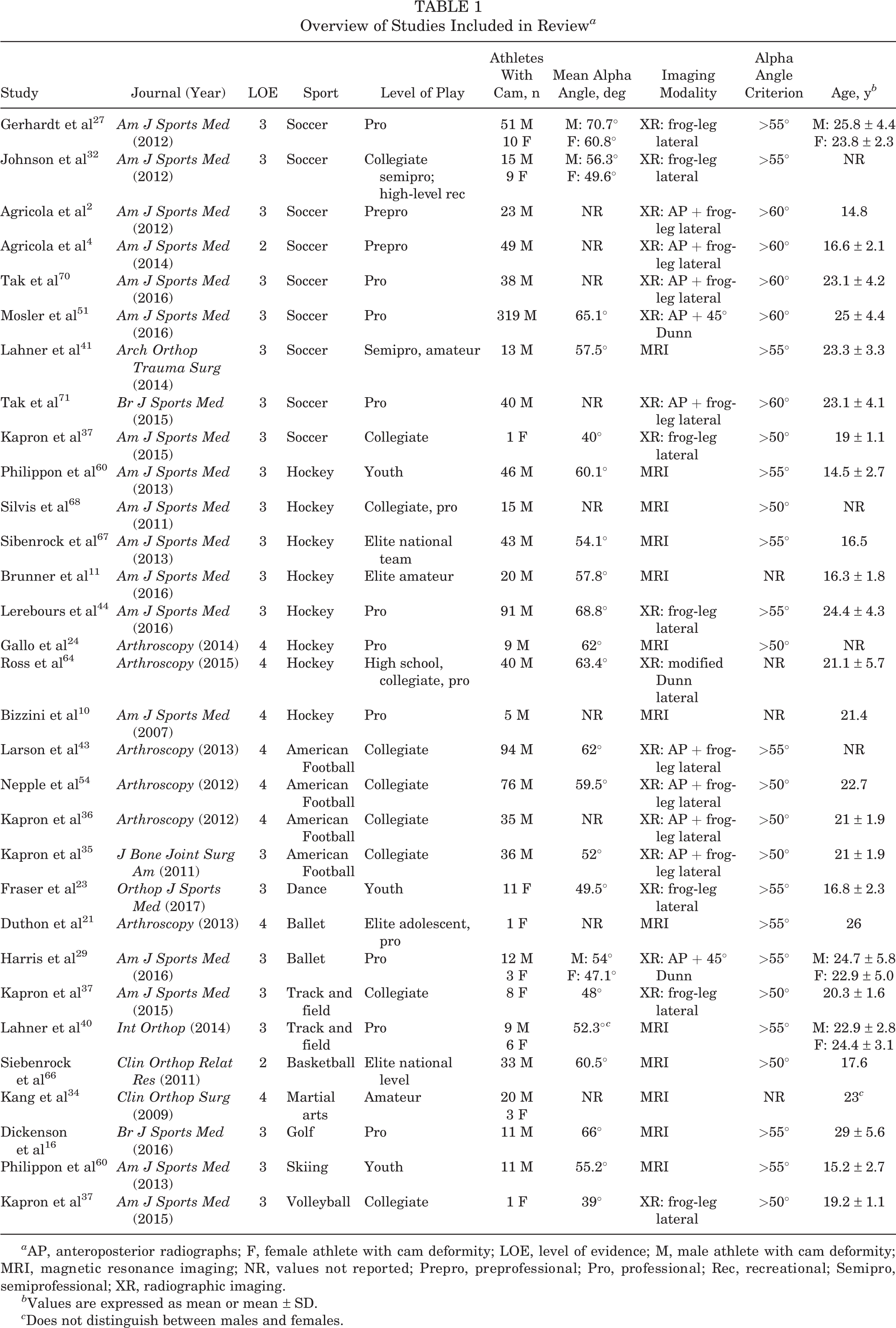
a AP, anteroposterior radiographs; F, female athlete with cam deformity; LOE, level of evidence; M, male athlete with cam deformity; MRI, magnetic resonance imaging; NR, values not reported; Prepro, preprofessional; Pro, professional; Rec, recreational; Semipro, semiprofessional; XR, radiographic imaging.
b Values are expressed as mean or mean ± SD.
c Does not distinguish between males and females.
Reported Number of Radiographic Cam Deformities Based on Sport a

a Dashes indicate no recordable data.
b Values are expressed as mean or mean ± SD.
Discussion
The purpose of this review was to determine the number of athletes with radiographic cam deformity reported in the literature based on sport. We identified 28 studies, comprising 1160 males and 53 females with cam deformity, with soccer being the sport with the highest number of athletes, followed by hockey and American football. Males possessed significantly greater alpha angle measurements compared with females, but no significant difference between sexes was found in age at the time of diagnosis. To our knowledge, this study represents the largest review examining the number of radiographic cam deformities in the literature based on sport. We were able to report on only the number of athletes with cam deformity, as the inherent limitations of the included studies and the strict inclusion/exclusion criteria prevented calculation of a true denominator, thus preventing estimations of cam deformity rate and prevalence.
Compared with nonathletes, athletes have been found to possess significantly greater numbers of cam deformities, suggesting a link between adolescent sport participation and the development of bony impingement. 2,52,66 Athletes participating in high-impact sports appear to be at greater risk for development of cam deformity. 4,38,45,58,73 In agreement with the preexisting literature, the highest reported number of athletes with cam deformities identified in this study participated in high-impact sports, namely soccer, hockey, and American football. 53 Ayeni et al 7 found that athletes participating in ice hockey were at 2.5 times greater odds of having cam impingement compared with nonathletes with similar demographics. Meanwhile, a recent meta-analysis found that the pooled prevalence rate by hip for cam deformity in male athletes was 41% versus 17% in male controls (P < .001). 55 As such, the increased number of athletes with cam deformities reported in the literature necessitates a thorough clinical and radiographic evaluation for each athlete presenting with hip or groin pain. Proper workup may help delay or effectively prevent the progression of chondrolabral damage by identifying athletes with deformities that are amenable to arthroscopic intervention, prior to the development of osteoarthritic changes. 19,46,66,74
The cause of cam development has been suggested to be a growth-related phenomenon, influenced not only by participation in athletic activity but also by the age of the athlete. Specifically, during skeletal maturation in which the proximal femoral growth plate is open, abnormal loading on the developing skeleton has been shown to lead to more adaptive, osteotrophic structural changes compared with the mature skeleton in response to repetitive, high-impact loading. 4,15,50,56 To date, the sex-based differences in cam development during maturation in youth athletes has not been examined, and this topic warrants investigation. In their investigation on the effect of hip loading during bone growth, Tak et al 71 reported a dose-response relationship between cam deformity development and age. Namely, the authors found that cam deformity was significantly more likely to develop in athletes who participated in soccer before age 12 years versus those beginning play at age 12. In a 2-year prospective study of preprofessional soccer athletes, Agricola et al 4 found a significant increase in the prevalence of cam deformity in athletes with open growth plates at baseline but found no significant increase in cam prevalence or severity following physeal closure. Furthermore, continued participation in high-impact versus endurance or low-impact sports has been shown to exacerbate deformity over time; Philippon et al 60 reported a significant correlation between age and elevated alpha angles associated with cam deformity in youth ice hockey athletes that was not seen in age-matched skiers.
Moreover, modern athletes are likely at higher risk for deformity secondary to overuse and excessive training, as increasing numbers of adolescent athletes specialize in a single sport at an early age. 1,17 The impact of rigorous sporting activity on open physes has been examined in other joints, with similar pathologic processes developing in the proximal humeral physis in adolescent pitchers and in the distal radius in gymnasts. 13,18,48 As such, intense exercise and high-impact loading in skeletally immature athletes appear to increase the risk of cam development, emphasizing the importance of proper rest and preventive measures to potentially decrease the development of hip- and groin-related pain secondary to impingement.
The majority of studies in the available literature primarily document cam deformity solely in male athletes, with few studies reporting on the number of females with cam deformity. While differences in cam development between sexes is not well understood, 9 authors have theorized that increased male participation and reporting in sports that require high impact and placement of the hip in positions of risk, such as hockey and American football, account for this reported discrepancy. 59,62,69 In contrast, female-predominant sporting activities such as ballet and dance require supraphysiologic range of motion with less impact and shear stresses placed across the proximal femur, accounting for the higher reported number of symptomatic pincer lesions. 14,25 Similar to data from prior studies in which mean alpha angle values were 5.9° to 12.7° less in females compared with male counterparts, 27,33 findings from this study demonstrated significantly lower mean alpha angles in females with cam deformity compared with males. The increased prevalence in males has also been verified in the general population, with Gosvig et al 28 reporting that in their study of 4151 asymptomatic adults in the Copenhagen Osteoarthritis Substudy, cam deformity was found in 17% of males versus only 4% of females. Meanwhile, prior radiographic investigations have estimated the distribution of cam deformity to be 14:1 among males versus females. 72 With increased female participation in contact sports over the past decade however, further investigations examining the rate and long-term impact of cam deformity in the female athlete are warranted.
Soccer was the most common sport reporting athletes with radiographic cam deformity, comprising the greatest number of both male and female athletes. As soccer is primarily characterized by running and kicking, 32 it is believed that the forced flexion, adduction, and internal rotation during kicking result in repetitive abutment of the femoral neck against the acetabulum. As these motions are analogous to the maneuvers used during impingement testing, high stress is placed across the proximal femur, initiating and exacerbating cam deformities with the potential for resultant chondrolabral damage. 39,41 Overall, hip and groin pain have been shown to account for a significant amount of time lost from play in soccer, representing 11% to 16% of time loss injuries. 31 As such, coupled with the necessity of placing the hip in positions of risk, the popularity of soccer in the skeletally immature youth and adolescent populations places soccer athletes at high risk for the development of cam deformity.
Similar to soccer athletes, the high reported number of cam deformities in hockey athletes is likely secondary to the unique skating and cutting demands of the sport, placing the hip in vulnerable positions for high physical stress and pathologic contact between the proximal femoral physis and acetabulum during growth. 60,67,69 Specifically, 2 unique at-risk positions have been identified: hip abduction with external rotation as experienced during the push-off phase of the skating cycle, and hip flexion with internal rotation associated with the recovery phase of the skating cycle. 69 Further increasing the risk of impingement and demand stress placed across the proximal femur, hockey goalies may be required to place their hips in the “butterfly” position, requiring maximal flexion and internal rotation with associated axial loading as the knees hit the ice. 64 When all positions were examined for cam deformity, studies by both Ross et al 64 and Lerebours et al 44 found that hockey goalies possessed the highest prevalence of cam-type deformity in addition to the least acetabular coverage. Compared with nonathlete controls, hockey athletes have been found to be at 2.5 times higher risk for the development of cam deformity. 7 When comparing youth hockey athletes with youth skiers, Philippon et al 60 found that hockey athletes had a significantly greater prevalence of alpha angles associated with cam deformity. Moreover, a significant correlation between increasing athlete age and increasing alpha angles was found in male hockey athletes but not skiers, supporting the notion that continuation of the unique demands placed on the hip during hockey represents a significant etiological factor behind cam development. 60 No correlation among female hockey athletes performing the same maneuvers has been reported, and this topic merits further study.
The presence of cam deformity in American football athletes has received increased attention within the past decade, given the high risk for impingement secondary to positional requirements, coupled with the increased musculature and body mass of American football athletes. 34 Multiple investigations have demonstrated a high percentage of radiographic findings indicative of cam impingement in both symptomatic and asymptomatic football athletes. 35,36,43,54 Kapron et al 35 found that despite being only weakly associated, both athlete weight and athlete body mass index were significantly correlated with elevated alpha angles indicative of cam deformity in collegiate American football athletes. In their retrospective evaluation of 107 athletes (123 hips) evaluated at the National Football League Scouting Combine from 2007 to 2009, Nepple et al 54 found that despite not reaching statistical significance, cam prevalence and increased alpha angles were more common in athletes playing positions requiring greater hip flexion, namely linemen, tight ends, and linebackers. Given the multitude of injuries experienced by American football athletes, it is crucial to rule out pain secondary to cam impingement versus strains of the hip flexors and adductors, or core muscle injury, in order to introduce treatment strategies to prevent the initiation or progression of chondrolabral injury and arthritis. 54
This study is not without limitations. Given the method of the investigation, the true prevalence of radiographic cam deformity in athletes was not calculated, because no accurate denominator could be derived based on the strict inclusion/exclusion criteria used. The diagnosis of cam deformity was based on alpha angle measurements; however, various cutoff values and imaging modalities were used. Because of the lack of a universally accepted consensus on the cutoff value identifying cam deformity, recorded alpha angle threshold values have ranged from 50° 24,35 –37,54,66,68 to 60°, 2,4,51,70,71 while others have suggested that values of 63° be used. 63 As a result, athletes diagnosed with cam deformity in one investigation may have been excluded in another, likely underestimating the true reported number of cam deformities in the literature.
Although alpha angle measurements have been shown to demonstrate poor interobserver reliability, alpha angle measurements were the most commonly reported value and were thus used as the standard to define radiographic cam deformity, as few studies 27,37,54 reported head-neck offset measurements. Both radiographic imaging and magnetic resonance imaging were used to measure alpha angle values. It is possible that the degree of deformity was underestimated in athletes evaluated for cam deformity by use of AP and frog-leg lateral radiographs, as radiographic measurements have been shown to underestimate radiographic values compared with 3-dimensional imaging. 20 As such, cam deformity remains primarily a clinical diagnosis, with no universally accepted pathognomonic value based on alpha angle. 15 Because not all athletes with radiographic cam deformities are symptomatic, the optimal treatment of athletes with asymptomatic cam deformity remains controversial and dependent on a number of clinical and patient-specific factors.
The presence and extent of chondrolabral injuries were not reported in all included studies, preventing any meaningful analysis of the extent of damage or osteoarthritic changes based on sport. Similarly, leg dominance was infrequently reported; however, impingement lesions have been shown to develop independent of leg dominance. 4 While most athletes have demonstrated elements of mixed impingement, 9,25,30 with both cam and pincer deformity, the number of athletes with pincer lesions and mixed pathologic changes was infrequently reported; thus we were only able to record those with radiographic cam deformity.
Conclusion
Results of this review indicate that soccer and hockey are the most commonly reported sports in the current literature documenting athletes with radiographic cam deformity; males possess significantly greater mean alpha angle measurements, with no significant difference between the sexes in mean age at the time of diagnosis. Further prospective studies are necessary to better understand athletes at greatest risk for the development of symptomatic cam impingement based on sport to establish measures aimed at limiting time lost from play while preventing the progression of chondrolabral damage and hip OA.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.N. has received research support from Allosource, Arthrex, Athletico, DJ Orthopaedics, Linvatec, Miomed, Smith & Nephew, and Stryker; is a paid consultant for Ossur and Stryker; and receives royalties from Pivot Medical and Elite Orthopaedics. J.E.V. is a paid consultant for Arthrex, Linvatec, and Stryker. M.J.S. is a paid consultant for Smith & Nephew and receives royalties from Linvatec and Elite Orthopaedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.