
Abstract
Background:
Bone marrow lesions (BMLs) have been found on magnetic resonance imaging in patients with meniscal tears.
Purpose:
We sought to determine the prevalence and location of BMLs, the association between BMLs and chondral lesions, and the association between BMLs and pain in patients without radiographic evidence of degenerative joint disease who underwent arthroscopic partial meniscectomy (APM).
Study Design:
Cohort study; Level of evidence, 2.
Methods:
We performed a secondary analysis of the Chondral Lesions And Meniscus Procedures (ChAMP) randomized controlled trial. BMLs were assessed on preoperative magnetic resonance imaging, and chondral lesions were documented at the time of surgery. Pain was assessed preoperatively and at 1 year after APM using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and the Knee injury and Osteoarthritis Outcome Score (KOOS). The chi-square test was used to examine the association between BMLs and chondral lesions, and the F test was used to examine the association between BMLs and pain.
Results:
Of 241 patients, 58.9% had ≥1 BMLs, and most were located on the medial tibial plateau (MTP; 74.6%) and/or medial femoral condyle (MFC; 28.9%). Most MTP BMLs were submeniscal (56%), and most MFC BMLs extended beyond the meniscus (73%). There were more MFC chondral lesions for patients with any MFC BMLs (P = .01) and submeniscal MFC BMLs (P = .02) versus those without BMLs, and there was no association between BMLs and chondral lesions on the MTP. There was also no association between BMLs and preoperative or postoperative pain scores.
Conclusion:
In patients without radiographic evidence of degenerative joint disease who underwent APM, BMLs were found in 58.9% of knees and were primarily located in the medial compartment. There was a borderline statistically significant association between BMLs and chondral lesions for the MFC; however, BMLs were not associated with pain scores preoperatively or at 1 year after surgery.
A bone marrow lesion (BML) on magnetic resonance imaging (MRI) likely represents hemorrhage, edema, or infarction resulting from trabecular microfracture. 15 Diminished signal intensity on T1-weighted MRI and increased signal intensity on T2-weighted fat-suppressed MRI indicate a BML. 14 BMLs have been primarily studied in patients undergoing anterior cruciate ligament reconstruction and likely represent the footprint of the mechanism of injury; however, BMLs have also been found in 39% to 43% of patients with meniscal tears. 9,16,22 Most BMLs occur in the medial compartment of patients with suspected meniscal tears. 22
BMLs have additionally been found in patients with radiographic evidence of knee osteoarthritis and are predictive of cartilage loss. 7,12,17 However, in patients without evidence of degenerative joint disease (DJD) on radiographs, it is not known if BMLs are associated with chondral lesions or are caused by changes in joint-loading patterns because of a meniscal tear. Two studies have found an association between BMLs and function after arthroscopic partial meniscectomy (APM), but none has reported an association with postoperative pain. 9,11 Also, Bisson et al 4 found greater improvement in clinical outcomes after APM for patients without chondral lesions versus those with chondral lesions left in situ. Determining the association between BMLs, chondral lesions, and pain in patients undergoing APM can help guide treatment regimens and assist in counseling patients about proper expectations after treatment.
We conducted a secondary analysis using data from the Chondral Lesions And Meniscus Procedures (ChAMP) randomized controlled trial, which was designed to examine the effect on knee pain of arthroscopic debridement versus observation (no debridement) of Outerbridge grade II to IV unstable chondral lesions found during APM in patients aged ≥30 years. 3 The aims of the present study were (1) to examine the prevalence and location of BMLs in patients with normal radiographs and symptomatic meniscal tears, (2) to examine the association between BMLs and chondral lesions, and (3) to examine the association between BMLs and pain before and after APM. We hypothesized that BMLs would be prevalent, be associated with chondral lesions identified at the time of surgery, and be associated with increased pain before and after surgery.
Methods
Study Design
The ChAMP trial was a double-blind randomized controlled trial that examined the effect of observation versus debridement of unstable chondral lesions on pain in patients undergoing APM. 3 The ChAMP trial is registered at ClinicalTrials.gov (NCT01527201) and was approved by an institutional review board.
Screening and Group Assignment
Six sports medicine fellowship-trained orthopaedic surgeons (L.J.B., W.M.W., M.S.F., G.A.B., M.A.R., J.M.M.) recruited consenting study participants between January 2012 and April 2015 at a single center. Preoperative inclusion criteria were age ≥30 years, persistent symptoms of a meniscal tear for at least 3 months (ie, joint-line tenderness and pain with joint compression and rotation), no definitive evidence of DJD on weightbearing radiographs (ie, Kellgren-Lawrence [K-L] grades 0-1, no visible osteophytes, and <50% joint space narrowing on anteroposterior weightbearing radiographs), meniscal tear confirmed by MRI, and having elected to undergo APM. 10 These indications are consistent with the current recommendations set forth by the European Society of Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA). 1 Exclusion criteria are listed in Appendix Table A1. Patients and data collectors were blind to treatment assignment and surgical findings until 1 year from surgery. A total of 1591 patients were eligible for this study, of whom 340 enrolled; of these, 241 patients had MRI scans available for an assessment of BMLs and were included in the final analysis (Figure 1).
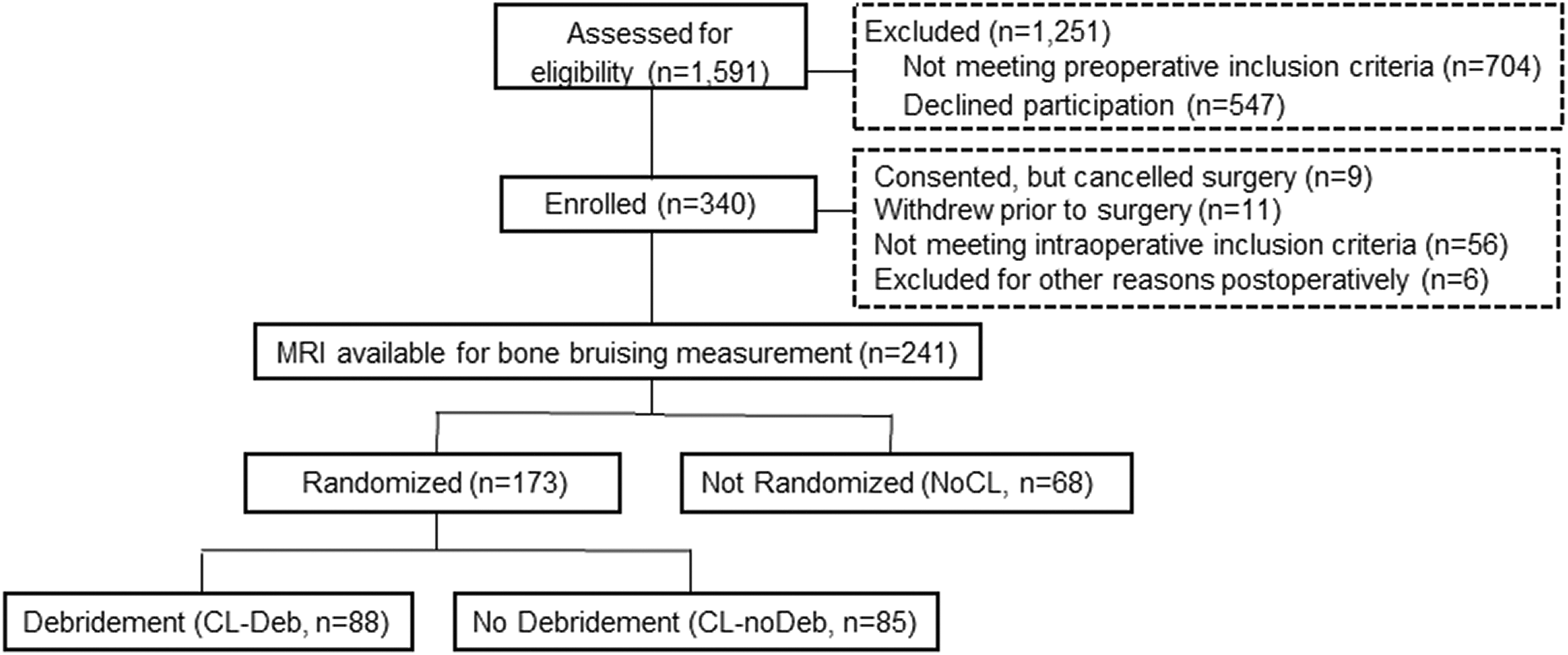
Sample flow chart. CL-Deb, debridement of unstable chondral lesions; CL-noDeb, no debridement of unstable chondral lesions; MRI, magnetic resonance imaging.
Intervention
All patients underwent diagnostic arthroscopic surgery, at which time the articular cartilage was examined, followed by APM of the medial, lateral, or both menisci. Patients with unstable chondral lesions in any compartment of the knee were randomized to receive debridement (CL-Deb group) or no debridement (CL-noDeb group) after APM. 3 During the study design, the surgeons met and blindly reviewed 13 arthroscopic photographs and videos to reach a consensus about defining unstable chondral lesions using the Outerbridge grading system. Unstable chondral lesions were defined as those greater than 1 cm2 with flaps that (1) could be displaced more than 5 mm with a probe or that (2) contained fibrillated cartilage involving greater than 50% of the depth of the cartilage. Good interrater reliability was found among the participating surgeons for chondral grading using the Outerbridge system (intraclass correlation coefficient, 0.94; P < .001).
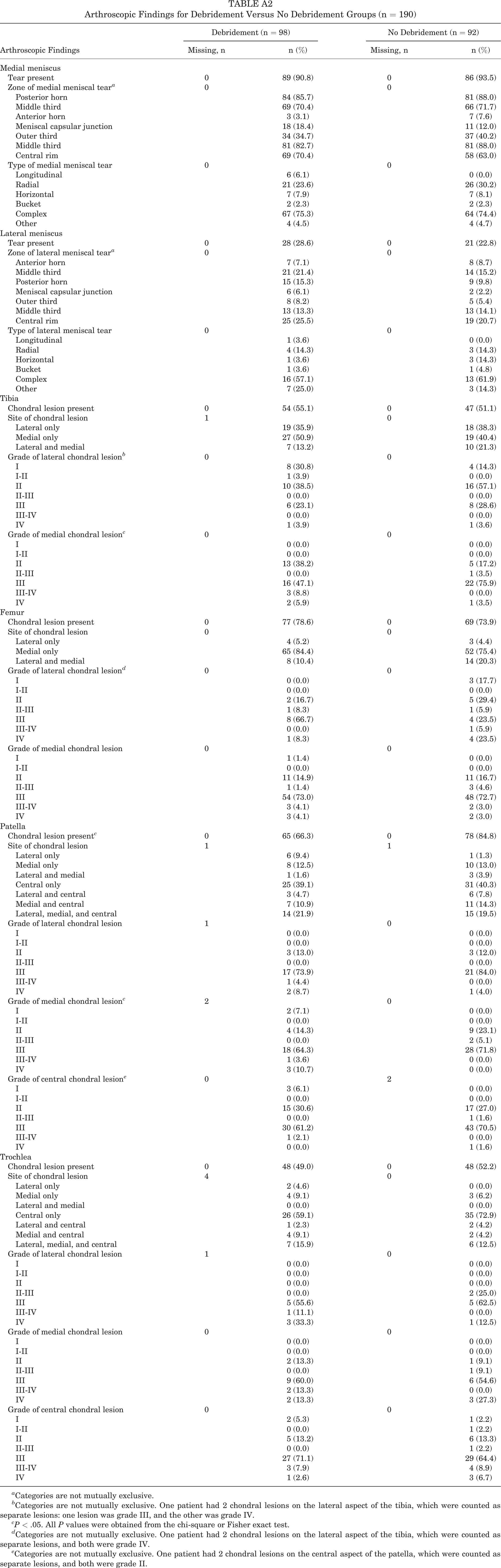
In the CL-Deb group, unstable chondral flaps of fibrillated cartilage were excised with a motorized shaver, but no subchondral debridement or microfracture was performed for any grade IV lesions. Arthroscopic findings for the CL-Deb and CL-noDeb groups from the original ChAMP trial study are presented in Appendix Table A2. Chondral lesions were left unaltered for patients in the CL-noDeb group. Patients without unstable chondral lesions were included in the nonrandomized no chondral lesion (NoCL) group and did not require surgical management of chondral lesions. An intra-articular injection of 20 mL of 0.5% bupivacaine was administered at the end of the procedure. All patients received a prescription for hydrocodone/acetaminophen 7.5 mg (1-2 pills orally twice a day as needed) after surgery, and physical therapy focused on eliminating of effusion, regaining of full range of motion, and progressive strengthening.
Measurement of BMLs on MRI
Preoperative MRI scans from all patients were examined by 2 independent reviewers (J.M., P.P.; orthopaedic residents trained in evaluating BMLs on MRI) for BMLs, as indicated by hyperintensity on sagittal, coronal, and axial cartilage-sensitive proton density–weighted high-resolution fast spin echo sequences when obtained at our institution or on similar sequences when patients brought outside scans. The location of BMLs was classified as the medial femoral condyle (MFC), lateral femoral condyle (LFC), medial tibial plateau (MTP), and/or lateral tibial plateau (LTP). The extent of BMLs was classified as none (no tibiofemoral BML), submeniscal (focally contained above or below the meniscus, extending to a maximum of 1 cm subchondrally), or extensive (extending beyond the meniscus and/or greater than 1 cm subchondrally). Patients with trochlear or patellar BMLs were excluded from the analysis. See Appendix Figures A1 through A4 for sample images of BMLs.
Demographic and Intra-articular Injury Data
Age at the initial visit (years), sex (male/female), and body mass index (BMI) were recorded. BMI was categorized as underweight (<18.50 kg/m2), normal weight (18.50–24.99 kg/m2), overweight (25.00-29.99 kg/m2), and obese (≥30.00 kg/m2). 21 Surgeons recorded arthroscopic findings on a standard data collection form after surgery. The presence, site, and Outerbridge grade of unstable chondral lesions on the tibia and femur were evaluated arthroscopically for this current study as well as the presence of medial meniscal (MM) and lateral meniscal (LM) tears.
Pain Scores
A description of all outcome scores that were collected during the ChAMP trial can be found elsewhere. 3 The current study used preoperative and 1-year postoperative Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and Knee injury and Osteoarthritis Outcome Score (KOOS) pain scores, both ranging from 0 (extreme pain) to 100 (no pain). 18,19
Statistical Analysis
Data from the 3 study groups (CL-Deb, CL-noDeb, and NoCL) were pooled together. Descriptive statistics were calculated for demographics stratified by the presence of BMLs and for the location (MTP, MFC, LTP, and LFC) and extent (submensical and extensive) of BMLs. The chi-square test was used to examine the association between the extent of BMLs and the presence of chondral lesions (yes/no) on the MTP and MFC. The MTP and MFC were selected because the majority of BMLs were located at these sites. Because of the small size of our groups, we did not perform subgroup analyses broken down by anatomic sites smaller than the medial or lateral condyles or plateaus. Patients with submeniscal and extensive BMLs were compared separately and collectively with those without BMLs.
To determine whether the presence or extent of a BML was associated with preoperative or postoperative pain, we performed 2 analyses. For analysis 1, we considered the ideal situation and examined whether the presence of a BML in the compartment containing the meniscal tear affected preoperative or 1-year postoperative pain scores. To do so, we pooled patients with the most common site of meniscal tears (MM) and compared those with any medial compartment BML (MFC and/or MTP) to those with no BMLs. The F test was used to examine the association between the extent of medial BMLs (located on the MFC and/or MTP) and preoperative and 1-year postoperative WOMAC and KOOS pain scores with adjustment for the presence of chondral lesions and for study group (debridement, no debridement, and no chondral lesions) in patients with MM tears. We also compared pain scores in all patients with the presence of any medial BML (submeniscal and/or extensive) with those with no BMLs. For analysis 2, to make the results generalizable to the real-life clinical situation (ie, where BMLs may not always be isolated to the compartment containing the meniscal tear), the F test was used to examine the association between BMLs located at any anatomic site (MTP, MFC, LTP, and/or LFC) and preoperative and 1-year postoperative WOMAC and KOOS pain scores with adjustment for the presence of chondral lesions and for study group (CL-Deb, CL-noDeb, and NoCL). The reason that both analyses 1 and 2 were adjusted for the presence of chondral lesions was because chondral lesions have been shown to influence postoperative pain and for treatment group was because we wanted to ensure that this factor did not confound our findings. 4 It should be noted that the primary ChAMP trial study results found no difference between the 2 treatment groups at 1 year after surgery. 5
Results
Patient Characteristics and Prevalence of BMLs
The mean patient age was 53.5 years, and the majority of patients were male (66.8%) and obese (42.7%). No patients had a subchondral fracture. BMLs were present on preoperative MRI in 142 (58.9%) patients with normal radiographs and arthroscopically confirmed meniscal tears. Demographics did not differ between those with and without BMLs (Table 1). The MM was involved in 75% of the meniscal tears; the location of the meniscal tear(s) did not differ between those with and without BMLs (Table 1). Most BMLs were located on the MTP (74.6%) and/or MFC (28.9%) (Table 2). The majority of MTP BMLs were submeniscal (56%), and the majority of MFC BMLs were extensive (73%). Overall, 29% of patients with MTP BMLs had MTP chondral lesions, and 78% with MFC BMLs had MFC chondral lesions. Of the patients with MM tears 85% had MFC and/or MTP BMLs.
Demographic Factors and Knee Injuries (N = 241) a

a Data are reported as n (%) unless otherwise indicated. BML, bone marrow lesion.
b Two patients were missing data.
Extent and Location of BMLs (n = 142) a

a Data are not mutually exclusive. Submeniscal BMLs were focally contained above or below the meniscus, extending a maximum of 1 cm subchondrally. Extensive BMLs extended beyond the meniscus and were greater than 1 cm subchondrally. BML, bone marrow lesion.
BMLs and Chondral Lesions
Submeniscal and/or extensive MTP BMLs were not associated with chondral lesions on the MTP (Table 3). There were more MFC chondral lesions for patients with any MFC BMLs (P = .01) and submeniscal MFC BMLs (P = .02) versus those without BMLs, and there was a borderline association (P = .05) between extensive MFC BMLs and chondral lesions on the MFC (Table 4).
Association Between Extent of BMLs and Chondral Lesions on Medial Tibial Plateau a

a Extent of BMLs was categorized as (1) submeniscal BMLs, which were focally contained above or below the meniscus, extending a maximum of 1 cm subchondrally, and (2) extensive BMLs, which extended beyond the meniscus and were greater than 1 cm subchondrally. One patient was missing data for the presence of chondral lesions, and 1 patient was missing data for the extent of BMLs. BML, bone marrow lesion.
bP values were calculated by the chi-square test.
Association Between Extent of BMLs and Chondral Lesions on Medial Femoral Condyle a
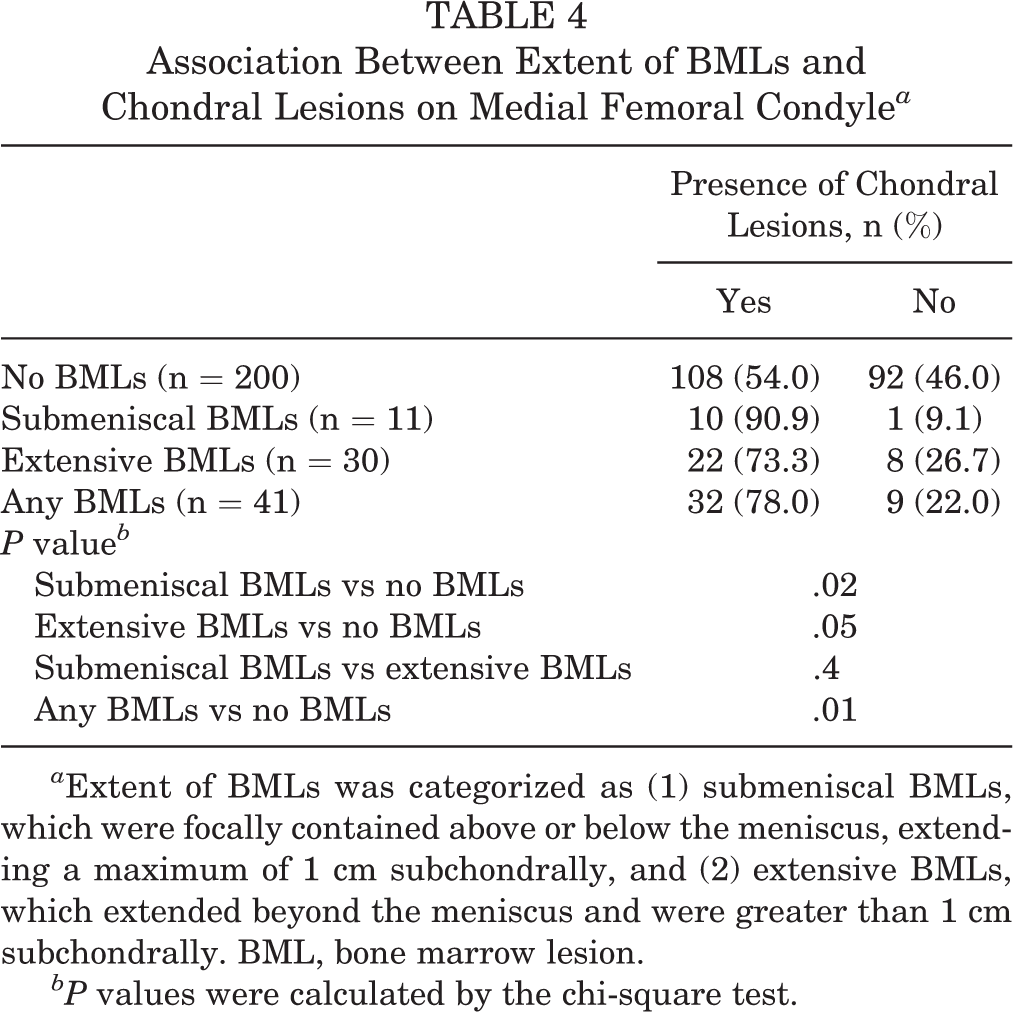
a Extent of BMLs was categorized as (1) submeniscal BMLs, which were focally contained above or below the meniscus, extending a maximum of 1 cm subchondrally, and (2) extensive BMLs, which extended beyond the meniscus and were greater than 1 cm subchondrally. BML, bone marrow lesion.
bP values were calculated by the chi-square test.
BMLs and Pain Scores
For analysis 1, submeniscal or extensive medial BMLs were not associated with preoperative or 1-year postoperative pain scores in patients with MM tears when adjusted for chondral lesions and treatment group (Table 5). For analysis 2, medial and/or lateral BMLs were not associated with preoperative or 1-year postoperative pain scores when adjusted for chondral lesions and treatment group (Table 6).
Association Between Extent of Medial BMLs and Preoperative and Postoperative Pain Scores in Patients With Medial Meniscus Tears a

a Data are reported as mean ± SD unless otherwise indicated. Extent of BMLs was categorized as (1) submeniscal BMLs, which were focally contained above or below the meniscus, extending a maximum of 1 cm subchondrally, and (2) extensive BMLs, which extended beyond the meniscus and were greater than 1 cm subchondrally. Medial BMLs included BMLs on both the medial tibial plateau and medial femoral condyle. Patients with (1) both medial submeniscal and extensive BMLs and (2) both medial and lateral meniscal tears were excluded. BML, bone marrow lesion; KOOS, Knee injury and Osteoarthritis Outcome Score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Postoperative represents 1 y ± 1 mo.
c The 1-year difference is equal to preoperative minus postoperative scores.
dP values were calculated by the F test and were adjusted for the presence of chondral lesions and study group (debridement, no debridement, and no chondral lesions).
Association Between Preoperative and Postoperative Pain Scores and BMLs a

a Data are reported as mean ± SD unless otherwise indicated. The presence of BMLs located on any anatomic site were included (medial tibial plateau, medial femoral condyle, lateral tibial plateau, and lateral femoral condyle). BML, bone marrow lesion; KOOS, Knee injury and Osteoarthritis Outcome Score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Postoperative represents 1 y ± 1 mo.
c The 1-year difference is equal to preoperative minus postoperative scores.
dP values were calculated by the F test and were adjusted for the presence of chondral lesions and study group (debridement, no debridement, and no chondral lesions).
Discussion
We examined the prevalence of BMLs and their association with chondral lesions and pain in patients undergoing APM by conducting a secondary analysis of the ChAMP trial, which was designed to compare debridement versus observation of chondral lesions encountered during APM. 3 The ChAMP trial found no difference in outcomes for patients randomly assigned to CL-Deb or CL-noDeb and also found that patients with unstable chondral lesions (regardless of observation or debridement) had worse results than those without such lesions. 4,5
In the present study, we hypothesized that BMLs would be prevalent, be associated with chondral lesions identified at the time of surgery, and be associated with increased pain before and after surgery. We found that more than half of our sample had BMLs on preoperative MRI, and there was an association between BMLs and chondral lesions located on the MFC. Contrary to our hypothesis, BMLs were not associated with pain scores preoperatively or postoperatively. Instead, meniscal tears and/or chondral lesions may be more predictive of pain than BMLs.
The prevalence of BMLs in our study (58.9%) was greater than in some previous studies (39%-43%) of patients with meniscal tears, and 85% of patients had concomitant medial BMLs and MM tears. 9,22 Zanetti et al 22 also found that BMLs in patients with suspected meniscal tears were primarily found in the medial compartment. However, similar to our study, Bergin et al 2 found subchondral marrow edema in 60% of patients with MM tears and in 90% with LM tears. We found that BMLs on the MTP were primarily submeniscal or focally contained below the meniscus, extending ≤1 cm subchondrally (56%), and that BMLs on the MFC primarily extended beyond the meniscus and were >1 cm subchondrally (73%). This could imply different causes of the BMLs at different sites, for instance, chondral loss on the femur and increased contact pressure due to the loss of meniscal integrity on the tibia.
Regarding the relationship between BMLs and chondral lesions, MFC BMLs were associated with MFC chondral lesions, but MTP BMLs were not associated with MTP chondral lesions. This could be explained if BMLs on the MTP were caused by changes in local contact pressure due to the meniscal tear itself. It should be noted that our study was confined to patients without definitive radiographic signs of osteoarthritis (K-L grade 0-1). It is also a secondary analysis, so our results should be considered preliminary. Finally, our outcomes were collected at 1 year, and those patients with BMLs may progress to osteoarthritis over a longer time period. Several studies have observed BMLs in patients with radiographic knee osteoarthritis. 12,17,20 Women with knee osteoarthritis were 4.3 times more likely to have a BML, and BMLs greater than 1 cm were associated with full-thickness cartilage lesions. 20 Link et al 12 found increased BMLs with increasing K-L grade in patients with various degrees of knee osteoarthritis. Raynauld et al 17 found that tibiofemoral BMLs in the medial and/or lateral compartment were associated with the progression of knee osteoarthritis. While our present study found no difference between groups in pain scores at 1 year, we are collecting clinical and radiographic results at 5 years, which should help clarify whether patients with BMLs at the time of arthroscopic meniscectomy are at a higher risk for later osteoarthritis compared with those without BMLs. Also, we do not know if the BMLs resolved or worsened after meniscectomy.
We performed 2 analyses to explore the association between BMLs and pain. Analysis 1 was intended to isolate the contribution of BMLs to pain and therefore included only patients meeting ideal criteria (ie, patients with isolated meniscal tears and BMLs only in the compartment containing the meniscal tear). To meet these criteria, we included only isolated MM tears and compared any confined and extensive medial BMLs with no medial BMLs. In this analysis, medial BMLs were not associated with pain in patients with MM tears; however, this subanalysis resulted in a smaller sample size and may not have been powerful enough to detect an association between BMLs and pain. Analysis 2 was intended to reflect the heterogeneous clinical scenario in which individual patients have medial, lateral, or MM and LM tears, and BMLs may be present at multiple sites. This makes the results more generalizable to actual patient populations but increases the risk of confounding. In analysis 2, we examined the association between BMLs located at any anatomic site and pain in patients with MM and/or LM tears and also found this association to be null. We were therefore unable to demonstrate an association between BMLs and preoperative or postoperative pain, and a post hoc power analysis demonstrated adequate power to determine that an association in our population does not exist.
Other studies have sought to explore the contribution of BMLs to pain in patients with meniscal tears. In patients undergoing APM, Katz et al 9 found that medial BMLs predicted worse function but that BMLs in any compartment were not associated with pain. Kijowski et al 11 found worse International Knee Documentation Committee (IKDC) scores for severe MFC BMLs, comorbid MM tears and medial BMLs, and comorbid LM tears and LFC BMLs after APM. Their populations included more patients with radiographic osteoarthritis, however, and this makes their results difficult to compare to ours. There is also some preliminary research showing that subchondroplasty may alleviate pain in the short term after surgery in patients with BMLs. 6 Obtaining a better understanding of the effect of BMLs on preoperative MRI and outcomes after APM can aid in patient counseling and developing proper treatment regimens.
Strengths of this study include its prospective design and measurements of both the location and extent of BMLs, which have not been reported in previous studies of patients undergoing APM. 9,11,22 Also, we were able to examine the association between the location of BMLs and chondral lesions, which has not been reported before. Limitations include the fact that we only used preoperative MRI scans, and some were obtained from outside facilities. Variation in MRI machines and radiology technician skill levels may have led to random errors, but all MRI scans were of sufficient quality to determine the presence, location, and extent of any BMLs. We did not routinely obtain long-leg standing films to assess alignment, leading to the possible inclusion of patients with malalignment, which was not evident on standard anteroposterior weightbearing radiographs. We did not seek to correlate the site of any BML(s) with the location of the meniscal tear because this relationship would vary with knee flexion angle for BML(s) on the femur and because tibial BMLs may not be anatomically co-located with the meniscal tear because of contact force changes on the tibia that could be found remotely from the site of the meniscal tear. We also do not know if BMLs were from acute trauma or chronic stresses, and we did not perform follow-up MRI to assess the healing rate of BMLs, which may have prevented us from finding an association between BMLs and postoperative pain because BMLs could have healed during the course of follow-up. The time to resolution of BMLs has been found to range from 3 weeks to 2 years. 13
Despite these limtations, the finding that the presence of ≥1 BMLs on preoperative MRI does not portend a worse 1-year postoperative result is valuable information to have when counseling patients about what to expect after APM. Another theoretical limitation is that osteoarthritis as used in our analyses was defined arthroscopically rather than radiographically. In the original ChAMP trial study, using standing anteroposterior rather than 45° posteroanterior flexed radiographs may have allowed some patients with greater degrees of osteoarthritis to be included theoretically; however, this did not occur based on arthroscopic findings (ie, no patients in the study had diffuse grade IV chondromalacia in any compartment). Standing long-leg radiographs to assess axial alignment were not routinely obtained during the study, but our inclusion of only patients with K-L grades 0 and 1 prevented the inclusion of malalignment due to osteoarthritis. We are unaware of a reliable and reproducible method to quantify the amount of meniscus resected and cannot provide a subgroup analysis of the effect of the amount of meniscus resected on outcomes. Our sample consisted primarily of male and obese patients; however, these factors were not associated with the presence of BMLs, and thus, selection bias should not have been an issue. These demographics also reflect the population of patients generally indicated for arthroscopic meniscectomy. For instance, the prevalence of obesity in our sample is nearly identical to the national prevalence of obesity in middle-aged adults (42.3%). 8 Age, sex, and BMI did not differ between patients with and without BMLs and thus were not adjusted for in our analysis. There may have been other factors not measured in this study that could have confounded our results.
Finally, this study was a secondary analysis and was not powered to detect an association between BMLs and chondral lesions or pain. Overall, there was 15% loss to follow-up. However, a post hoc power analysis showed that our sample had 97% power to detect a 25% difference in MTP chondral lesions between those with and without MTP BMLs and 86% power for analysis 1 to detect a 10-point difference in the WOMAC pain score between those with and without medial BMLs. Thus, there may truly be no association between (1) MTP BMLs and MTP chondral lesions and (2) the WOMAC pain score and medial BMLs; however, a definitive answer to this question would require a study designed specifically to examine the association between BMLs, chondral lesions, and pain.
Conclusion
In patients with meniscal tears, with no radiographic evidence of DJD and who elected to undergo APM, BMLs were common and primarily located in the medial compartment. There was an association between BMLs and chondral lesions located on the MFC and no association between BMLs and chondral lesions on the MTP. When BMLs are encountered on the femur, clinicians should therefore strongly consider the existence of chondral lesions. Finally, we found that BMLs were not associated with preoperative or 1-year postoperative pain, once the presence of any associated chondral lesions was taken into account. These findings should help clinicians counsel patients with minimal radiographic arthritis and BMLs on MRI who are seeking treatment for meniscal tears.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Ralph C. Wilson, Jr. Foundation. L.J.B. has received research support from Arthrex and educational support from Zimmer Biomet and Prodigy Surgical Distribution. W.M.W. has received hospitality payments from Arthrex, Prodigy Surgical Distribution, and Sanofi-Aventis. M.S.F. has received hospitality payments from Arthrex and Prodigy Surgical Distribution. G.A.B. has received educational support from Arthrex and Prodigy Surgical Distribution and hospitality payments from Linvatec, Smith & Nephew, and Stryker. M.A.R. has received consulting fees from Integer Holdings, has received educational support from Arthrex and Prodigy Surgical Distribution, receives royalties from Stryker, and has received hospitality payments from Smith & Nephew and Trice Medical. J.M.M. has received research support from Carestream Health, hospitality payments from Linvatec, and educational support from Arthrex. AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University at Buffalo Institutional Review Board.
APPENDIX
Arthroscopic Findings for Debridement Versus No Debridement Groups (n = 190)
| Arthroscopic Findings | Debridement (n = 98) | No Debridement (n = 92) | ||
|---|---|---|---|---|
| Missing, n | n (%) | Missing, n | n (%) | |
| Medial meniscus | ||||
| Tear present | 0 | 89 (90.8) | 0 | 86 (93.5) |
| Zone of medial meniscal tear a | 0 | 0 | ||
| Posterior horn | 84 (85.7) | 81 (88.0) | ||
| Middle third | 69 (70.4) | 66 (71.7) | ||
| Anterior horn | 3 (3.1) | 7 (7.6) | ||
| Meniscal capsular junction | 18 (18.4) | 11 (12.0) | ||
| Outer third | 34 (34.7) | 37 (40.2) | ||
| Middle third | 81 (82.7) | 81 (88.0) | ||
|
|
69 (70.4) | 58 (63.0) | ||
|
|
0 | 0 | ||
| Longitudinal | 6 (6.1) | 0 (0.0) | ||
| Radial | 21 (23.6) | 26 (30.2) | ||
| Horizontal | 7 (7.9) | 7 (8.1) | ||
| Bucket | 2 (2.3) | 2 (2.3) | ||
| Complex | 67 (75.3) | 64 (74.4) | ||
|
|
4 (4.5) | 4 (4.7) | ||
| Lateral meniscus | ||||
| Tear present | 0 | 28 (28.6) | 0 | 21 (22.8) |
| Zone of lateral meniscal tear a | 0 | 0 | ||
| Anterior horn | 7 (7.1) | 8 (8.7) | ||
| Middle third | 21 (21.4) | 14 (15.2) | ||
| Posterior horn | 15 (15.3) | 9 (9.8) | ||
| Meniscal capsular junction | 6 (6.1) | 2 (2.2) | ||
| Outer third | 8 (8.2) | 5 (5.4) | ||
| Middle third | 13 (13.3) | 13 (14.1) | ||
|
|
25 (25.5) | 19 (20.7) | ||
|
|
0 | 0 | ||
| Longitudinal | 1 (3.6) | 0 (0.0) | ||
| Radial | 4 (14.3) | 3 (14.3) | ||
| Horizontal | 1 (3.6) | 3 (14.3) | ||
| Bucket | 1 (3.6) | 1 (4.8) | ||
| Complex | 16 (57.1) | 13 (61.9) | ||
|
|
7 (25.0) | 3 (14.3) | ||
| Tibia | ||||
| Chondral lesion present | 0 | 54 (55.1) | 0 | 47 (51.1) |
| Site of chondral lesion | 1 | 0 | ||
| Lateral only | 19 (35.9) | 18 (38.3) | ||
| Medial only | 27 (50.9) | 19 (40.4) | ||
| Lateral and medial | 7 (13.2) | 10 (21.3) | ||
| Grade of lateral chondral lesion b | 0 | 0 | ||
| I | 8 (30.8) | 4 (14.3) | ||
| I-II | 1 (3.9) | 0 (0.0) | ||
| II | 10 (38.5) | 16 (57.1) | ||
| II-III | 0 (0.0) | 0 (0.0) | ||
| III | 6 (23.1) | 8 (28.6) | ||
| III-IV | 0 (0.0) | 0 (0.0) | ||
| IV | 1 (3.9) | 1 (3.6) | ||
| Grade of medial chondral lesion c | 0 | 0 | ||
| I | 0 (0.0) | 0 (0.0) | ||
| I-II | 0 (0.0) | 0 (0.0) | ||
| II | 13 (38.2) | 5 (17.2) | ||
| II-III | 0 (0.0) | 1 (3.5) | ||
| III | 16 (47.1) | 22 (75.9) | ||
| III-IV | 3 (8.8) | 0 (0.0) | ||
| IV | 2 (5.9) | 1 (3.5) | ||
| Femur | ||||
| Chondral lesion present | 0 | 77 (78.6) | 0 | 69 (73.9) |
| Site of chondral lesion | 0 | 0 | ||
| Lateral only | 4 (5.2) | 3 (4.4) | ||
| Medial only | 65 (84.4) | 52 (75.4) | ||
| Lateral and medial | 8 (10.4) | 14 (20.3) | ||
| Grade of lateral chondral lesion d | 0 | 0 | ||
| I | 0 (0.0) | 3 (17.7) | ||
| I-II | 0 (0.0) | 0 (0.0) | ||
| II | 2 (16.7) | 5 (29.4) | ||
| II-III | 1 (8.3) | 1 (5.9) | ||
| III | 8 (66.7) | 4 (23.5) | ||
| III-IV | 0 (0.0) | 1 (5.9) | ||
| IV | 1 (8.3) | 4 (23.5) | ||
| Grade of medial chondral lesion | 0 | 0 | ||
| I | 1 (1.4) | 0 (0.0) | ||
| I-II | 0 (0.0) | 0 (0.0) | ||
| II | 11 (14.9) | 11 (16.7) | ||
| II-III | 1 (1.4) | 3 (4.6) | ||
| III | 54 (73.0) | 48 (72.7) | ||
| III-IV | 3 (4.1) | 2 (3.0) | ||
| IV | 3 (4.1) | 2 (3.0) | ||
| Patella | ||||
| Chondral lesion present c | 0 | 65 (66.3) | 0 | 78 (84.8) |
| Site of chondral lesion | 1 | 1 | ||
| Lateral only | 6 (9.4) | 1 (1.3) | ||
| Medial only | 8 (12.5) | 10 (13.0) | ||
| Lateral and medial | 1 (1.6) | 3 (3.9) | ||
| Central only | 25 (39.1) | 31 (40.3) | ||
| Lateral and central | 3 (4.7) | 6 (7.8) | ||
| Medial and central | 7 (10.9) | 11 (14.3) | ||
| Lateral, medial, and central | 14 (21.9) | 15 (19.5) | ||
| Grade of lateral chondral lesion | 1 | 0 | ||
| I | 0 (0.0) | 0 (0.0) | ||
| I-II | 0 (0.0) | 0 (0.0) | ||
| II | 3 (13.0) | 3 (12.0) | ||
| II-III | 0 (0.0) | 0 (0.0) | ||
| III | 17 (73.9) | 21 (84.0) | ||
| III-IV | 1 (4.4) | 0 (0.0) | ||
| IV | 2 (8.7) | 1 (4.0) | ||
| Grade of medial chondral lesion c | 2 | 0 | ||
| I | 2 (7.1) | 0 (0.0) | ||
| I-II | 0 (0.0) | 0 (0.0) | ||
| II | 4 (14.3) | 9 (23.1) | ||
| II-III | 0 (0.0) | 2 (5.1) | ||
| III | 18 (64.3) | 28 (71.8) | ||
| III-IV | 1 (3.6) | 0 (0.0) | ||
| IV | 3 (10.7) | 0 (0.0) | ||
| Grade of central chondral lesion e | 0 | 2 | ||
| I | 3 (6.1) | 0 (0.0) | ||
| I-II | 0 (0.0) | 0 (0.0) | ||
| II | 15 (30.6) | 17 (27.0) | ||
| II-III | 0 (0.0) | 1 (1.6) | ||
| III | 30 (61.2) | 43 (70.5) | ||
| III-IV | 1 (2.1) | 0 (0.0) | ||
| IV | 0 (0.0) | 1 (1.6) | ||
| Trochlea | ||||
| Chondral lesion present | 0 | 48 (49.0) | 0 | 48 (52.2) |
| Site of chondral lesion | 4 | 0 | ||
| Lateral only | 2 (4.6) | 0 (0.0) | ||
| Medial only | 4 (9.1) | 3 (6.2) | ||
| Lateral and medial | 0 (0.0) | 0 (0.0) | ||
| Central only | 26 (59.1) | 35 (72.9) | ||
| Lateral and central | 1 (2.3) | 2 (4.2) | ||
| Medial and central | 4 (9.1) | 2 (4.2) | ||
| Lateral, medial, and central | 7 (15.9) | 6 (12.5) | ||
| Grade of lateral chondral lesion | 1 | 0 | ||
| I | 0 (0.0) | 0 (0.0) | ||
| I-II | 0 (0.0) | 0 (0.0) | ||
| II | 0 (0.0) | 0 (0.0) | ||
| II-III | 0 (0.0) | 2 (25.0) | ||
| III | 5 (55.6) | 5 (62.5) | ||
| III-IV | 1 (11.1) | 0 (0.0) | ||
| IV | 3 (33.3) | 1 (12.5) | ||
| Grade of medial chondral lesion | 0 | 0 | ||
| I | 0 (0.0) | 0 (0.0) | ||
| I-II | 0 (0.0) | 0 (0.0) | ||
| II | 2 (13.3) | 1 (9.1) | ||
| II-III | 0 (0.0) | 1 (9.1) | ||
| III | 9 (60.0) | 6 (54.6) | ||
| III-IV | 2 (13.3) | 0 (0.0) | ||
| IV | 2 (13.3) | 3 (27.3) | ||
| Grade of central chondral lesion | 0 | 0 | ||
| I | 2 (5.3) | 1 (2.2) | ||
| I-II | 0 (0.0) | 1 (2.2) | ||
| II | 5 (13.2) | 6 (13.3) | ||
| II-III | 0 (0.0) | 1 (2.2) | ||
| III | 27 (71.1) | 29 (64.4) | ||
| III-IV | 3 (7.9) | 4 (8.9) | ||
| IV | 1 (2.6) | 3 (6.7) | ||
a Categories are not mutually exclusive.
b Categories are not mutually exclusive. One patient had 2 chondral lesions on the lateral aspect of the tibia, which were counted as separate lesions: one lesion was grade III, and the other was grade IV.
cP < .05. All P values were obtained from the chi-square or Fisher exact test.
d Categories are not mutually exclusive. One patient had 2 chondral lesions on the lateral aspect of the tibia, which were counted as separate lesions, and both were grade IV.
e Categories are not mutually exclusive. One patient had 2 chondral lesions on the central aspect of the patella, which were counted as separate lesions, and both were grade II.